
Abstract
The purpose of this study is to investigate the risk factors for postoperative deep vein thrombosis (DVT) in patients with traumatic spinal fractures complicated with Spinal Cord Injury(SCI). We conducted a retrospective analysis of 110 patients with traumatic spinal fractures and SCI admitted to our hospital from March 2021 to April 2024. DVT was diagnosed using ultrasound. Patient history, general data, surgical data, laboratory tests, and thromboelastogram (TEG) results were collected. The patients were divided into a DVT group and a non-DVT group according to the results of ultrasound one week after surgery. The risk factors and diagnostic value were analyzed using binary logistic regression and receiver operating characteristic (ROC) curves in both univariate and multivariate analyses. Multivariate and ROC analysis results showed that D-dimer, lower extremity, duration of bedrest, and MA values of TEG were independent risk factors for DVT in SCI, with D-dimer having the highest diagnostic value (AUC = 0.883). The AUC values for lower extremity, duration of bedrest, and MA were 0.731, 0.750, and 0.625. In conclusion, Postoperative D-dimer > 5.065 mg/l, lower extremity < 3, duration of bedrest, and MA value of TEG are independent risk factors for postoperative DVT in SCI patients, D-dimer having the highest diagnostic value. When the above risk factors occur, clinicians need to be vigilant and take appropriate prevention and treatment measures.
Introduction
Traumatic spinal fracture refers to spinal fracture caused by high energy injuries such as traffic accidents, falling, and heavy objects. It is often accompanied by spinal cord injury(SCI), which can lead to physical disability and even death and increase the economic burden. Deep vein thrombosis (DVT) and pulmonary embolism (PE), collectively known as venous thromboembolism (VTE), are complications associated with SCI. SCI usually requires surgical treatment, and the risk of postoperative DVT is high. 1 Different studies have reported that the incidence of DVT varies from 10% to 90%.2,3 However, DVT is insidious, and some patients are asymptomatic and easily overlooked. When patients experience symptoms such as lower limb pain, swelling, dyspnea, or chest pain, it often suggests DVT. In severe cases, pulmonary embolism may occur, endangering the patient's life. 4 Few studies have investigated the risk factors for postoperative DVT in SCI, and no consistent conclusions have been reached. These patients generally experience high-energy injuries, prolonged bedrest rest, traumatic stress, spinal cord injury, and multiple fractures, all of which promote DVT. Some scholars have used mechanical and drug prevention methods for DVT in patients with spinal fractures, achieving certain curative effects but not ideal prevention outcomes. 5 Therefore, identifying the risk factors for postoperative DVT in patients with traumatic spinal fractures complicated by SCI and implementing corresponding preventive measures to reduce the incidence of DVT and improve the prognosis of patients with SCI is of great significance. Consequently, we conducted a study to identify the risk factors affecting DVT after SCI and explored the diagnostic value of different risk factors to provide a reference for diagnosis and treatment.
Materials and Methods
Study Population
Data was collected from patients March 2021 to April 2024 with spinal cord injuries caused by high-energy injuries.The risk factors of DVT after spinal cord injury were analyzed retrospectively. Inclusion criteria: no DVT during preoperative examination; patients with spinal fractures and spinal cord injuries caused by high-energy injuries (falling injuries, traffic accidents, heavy object injuries); patients without hemophilia, abnormal coagulation, or lower extremity varicose veins; those who received chemical and mechanical DVT prophylaxis after admission. Exclusion criteria: no spinal cord injury; fractures at other sites or old spinal fractures > 4 weeks; osteoporotic or pathological spinal fractures; patients with continuous anticoagulation abnormalities; preoperative diagnosis of DVT; previous history of venous thromboembolism; and patients with incomplete medical records and imaging data.
A total of 110 patients were included, comprising 90 males and 20 females. The patients’ ages ranged from 18 to 84 years. The fracture sites were distributed as follows: 36 cervical, 18 thoracic, 27 lumbar, 23 thoracolumbar, 3 cervical with thoracic spine, 2 cervical with lumbar spine, and 1 involving cervical, thoracic, and lumbar spine. None of the patients developed epidural hematoma or pulmonary embolism. The study was approved by the hospital ethics committee, and all patients agreed to participate in the study and signed the relevant consent documents.
Research Technique
The hospital routinely applied the Caprini venous thrombosis risk assessment scale to assess DVT risk. Caprini venous thrombosis risk assessment scale defines a score greater than 5 as a very high risk level, with a 40%–80% incidence of DVT, a 1%–5% mortality rate, and the need for drug and physical prevention of DVT. All patients with spinal cord injury had scores greater than 5 and were classified as a very high risk group. After excluding those with subarachnoid hemorrhage, lower limb skin damage, bleeding tendency, or abnormal coagulation function, From the beginning of admission to the hospital until 12 h before surgery, 24 h after surgery until the period of getting out of bedrest, all patients received low molecular weight heparin (LMWH)(5000U, once a day, subcutaneous injection, Nanjing Jian You Company, China)and mechanical prevention (intermittent pneumatic pressure device, twice a day, 30 min each time) to prevent DVT. LMWH injection was stopped from 12 h before surgery to 24 h after surgery, continue LMWH injection 24 h after surgery. We divided DVT into two types: proximal DVT (in the popliteal vein or its proximal end) and distal DVT (in the distal popliteal vein). Mixed thrombus is defined when both proximal and distal thrombus are present. All patients underwent bilateral limb venous color ultrasound examination after admission, and within one week after surgery. Patients were divided into DVT group and non-DVT group according to the results of postoperative bilateral DVT ultrasound. Non-DVT patients received 5000U of LMWH and mechanical prevention once daily. DVT patients received 5000U of LMWH twice daily and discontinued mechanical prevention. If there were anticoagulant contraindications or proximal thrombosis, a vascular surgical consultation was requested to assist in developing an individual treatment plan to prevent pulmonary embolism.
Study Instruments and Assays
Patient specimens were analyzed by the thromboelastogram diagnostic instrument (Haemoscope Corporation TEG5000) and the Haemoscope kaolin activation assay using the Haemoscope reagent. Test results were recorded by the tester including reaction time (R) (reference range: 4–9 min), coagulation time (K) (1–3 min), coagulation angle (α) (53°–72°), and maximum amplitude (MA) value (50–70 mm). Data were analyzed by analysis software from Haemoscope . Coagulation parameters were determined using the fully automated coagulation analyzer ACL-TOP700 (Beckman) using the programs and reagents developed for the ACL-TOP. Hematology parameters were determined using the fully automated blood analyzer XN-9000 (Sysmex) using the programs and reagents developed for the XN-9000.
Data Collection
General data were collected, including age, gender, comorbidities(hypertension, coronary heart disease, diabetes), somking, lower extremity(<3/≥3), time from fracture to surgery, duration of bedrest, operation time, blood loss, and blood transfusion. Laboratory data were collected, including D-dimer (measured on the first day post-surgery), C-reactive protein(CRP), hemoglobin(HGB), neutrophil(NEUT), platelet count(PLT), red cell volume distribution width(RDW), fibrinogen(FIB), thrombin time(TT), activated partial thromboplastin time(APTT), prothrombin time(PT), hypoproteinemia. Coagulation parameters and Hematology parameters of the blood specimens were collected/measured on post-operative day 1. Thromboelastogram (TEG)data were collected on the first day to the hospital, including reaction time (R) (4–9 min), coagulation time (K) (1–3 min), coagulation angle (α) (53°-72°), and maximum amplitude (MA) value (50–70 mm).
Statistical Analysis
Statistical analysis were performed with SPSS (Version 25, IBM SPSS Inc, Chicago, IL, USA).Continuous variables were presented as mean ± standard deviation and compared with an independent t test. Categorical variables are shown proporproportion and compared using the chi-square test. Univariate variables with a significant index (P < 0.05) were included in the multivariate analysis. The diagnostic value of each risk factor was evaluated by analyzing the receiver operating characteristic (ROC) curve and the area under the ROC curve (AUC). Test level of P < 0.05 was considered statistically significant.
Results
The Incidence of Postoperative DVT
The incidence of postoperative DVT in 110 patients with traumatic spinal fractures combined with SCI was 52.7%. Seven patients (6.4%) had proximal thrombus, and 51 patients had distal thrombus (46.4%). Inferior vena cava filters were placed in all seven patients with proximal thrombi, and none of the patients developed pulmonary embolism or epidural hematoma.
Univariate Analysis of Postoperative DVT
The general data of the two groups are shown in Table 1. The DVT group had Duration of bedrest of 14.28 ± 2.76 days, while the non-DVT group had 10.96 ± 3.75 days (P < 0.05). Operation time was 280.78 ± 100.166 min in the DVT group and 243.58 ± 78.59 min in the non-DVT group (P < 0.05). There were significant differences in lower extremity and the incidence of coronary heart disease between the two groups (P < 0.05). Compared with the non-DVT group, DVT group had decreased lower extremity, longer duration of bedrest, operation time, and higher incidence of coronary heart disease, making them more prone to DVT. There were no significant differences in age, sex, hypertension, diabetes, smoking, time from fracture to surgery, blood loss, and blood transfusion (P > 0.05).
Comparison General Data of two Groups of Patients.
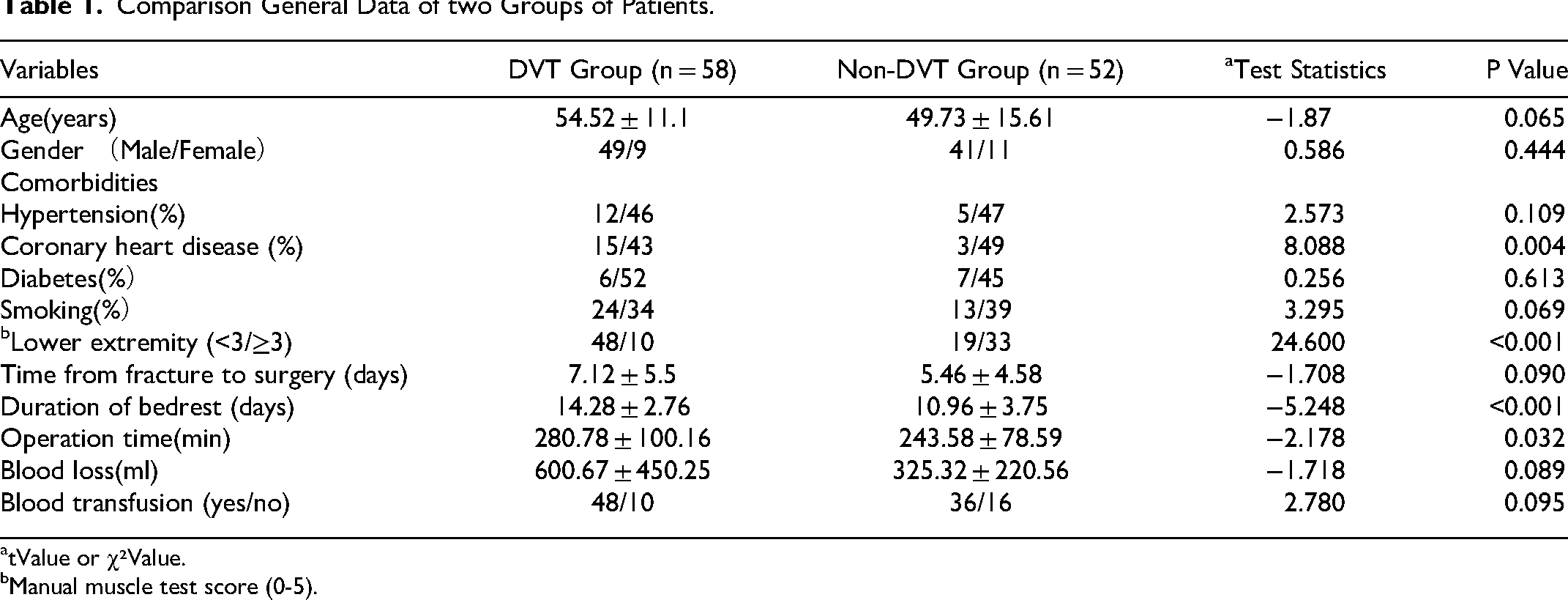
tValue or χ²Value.
Manual muscle test score (0-5).
Laboratory results from the two groups were compared, as shown in Table 2. D-dimer 9.93 ± 5.79 mg/l in DVT group and 2.99 ± 3.11 mg/l in non-DVT group (P < 0.05). CPR was 41.98 ± 40.08 mg/l in the DVT group and 20.15 ± 15.04 mg/l in the non-DVT group (P < 0.05). DVT group NEUT 10.57 ± 5.25 × 10^9/l, non-DVT group NEUT 8.58 ± 4.5 × 10^9/l, NEUT difference was significant (P < 0.05). RDW was 13.46 ± 1.28% in the DVT group and 12.85 ± 1.09% in the non-DVT group, with a significant difference in RDW (P < 0.05). FIB was significant in DVT group FIB 3.92 ± 1.57 g/l and non-DVT group FIB 3.32 ± 1.32 g/l (P < 0.05). In the DVT group, PT 13.88 ± 1.25 s, and non-DVT PT 13.46 ± 0.82 s(P < 0.05). Similarly, hypoproteinemia was significantly between the two groups (P < 0.05). There was no significant difference in HGB, PLT, TT and APTT between the two groups (P > 0.05).
Comparison of Laboratory Results Between two Groups of Patients.
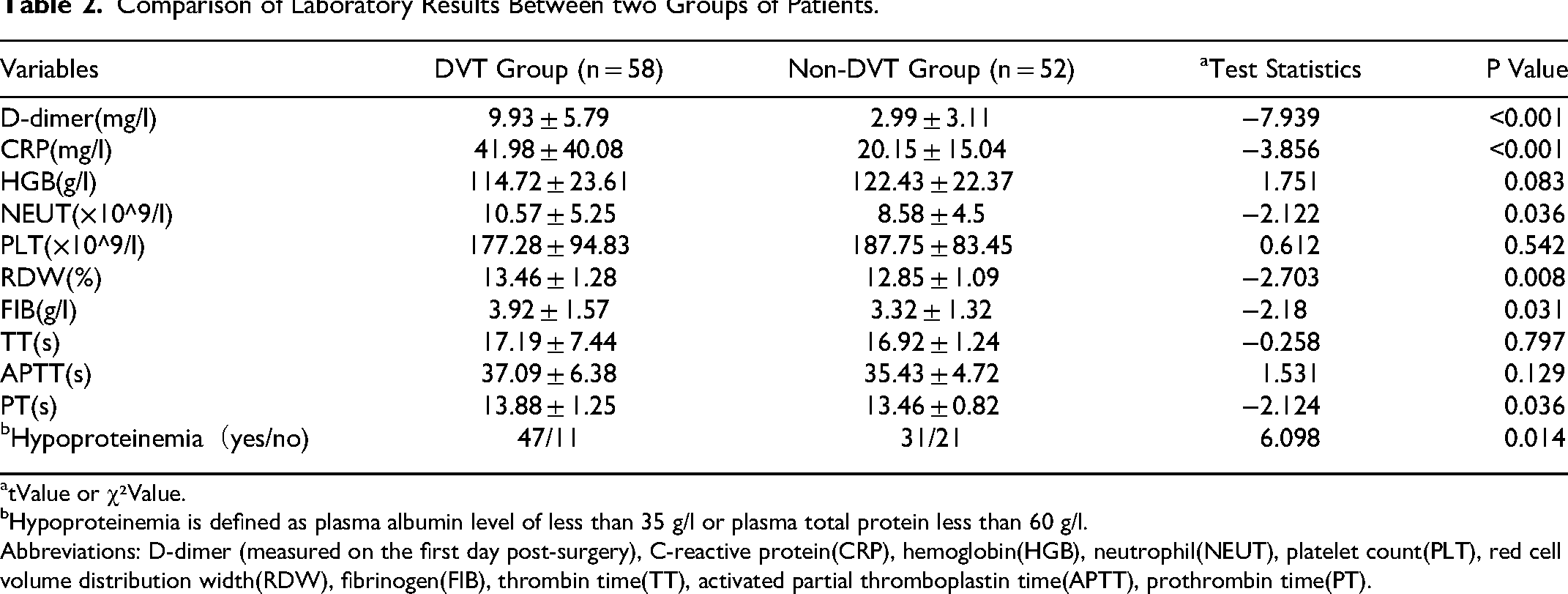
tValue or χ²Value.
Hypoproteinemia is defined as plasma albumin level of less than 35 g/l or plasma total protein less than 60 g/l.
Abbreviations: D-dimer (measured on the first day post-surgery), C-reactive protein(CRP), hemoglobin(HGB), neutrophil(NEUT), platelet count(PLT), red cell volume distribution width(RDW), fibrinogen(FIB), thrombin time(TT), activated partial thromboplastin time(APTT), prothrombin time(PT).
Comparing the two TEG groups, as shown in Table 3. R significant difference between DVT group 3.51 ± 0.83 min and non-DVT group 4.17 ± 0.81 min (P < 0.05). K was significant for 1.57 ± 0.79 min in DVT and non-DVT in 1.92 ± 0.61 min (P < 0.05). Angle was Angle67.52 ± 6.73°. DVT and Angle 64.84 ± 5.99°. Angle (P < 0.05). MA difference for DVT 61.95 ± 10.19 mm and non-DVT MA 58.16 ± 6.79 mm (P < 0.05).
Comparison the TEG of two Groups of Patients.
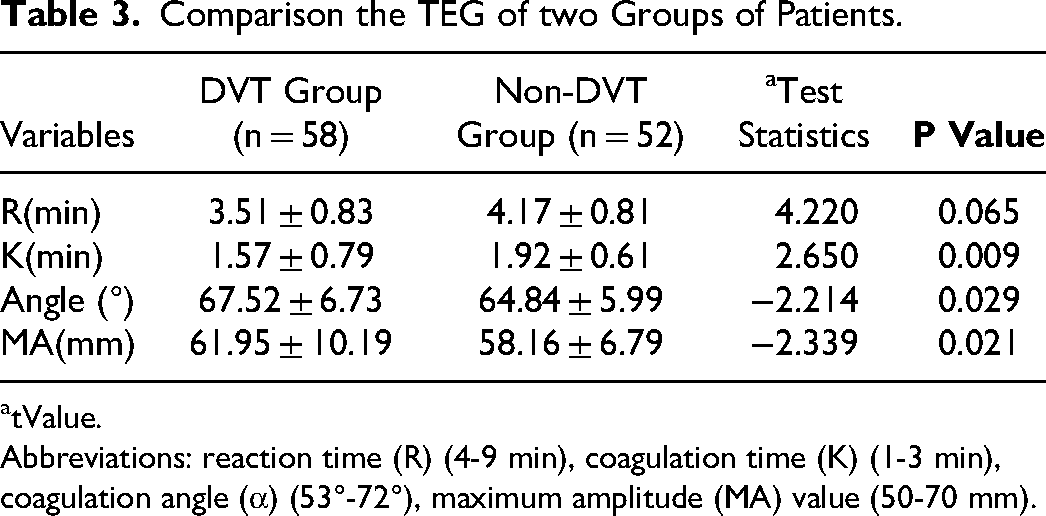
tValue.
Abbreviations: reaction time (R) (4-9 min), coagulation time (K) (1-3 min), coagulation angle (α) (53°-72°), maximum amplitude (MA) value (50-70 mm).
Multivariate Analysis of Postoperative DVT
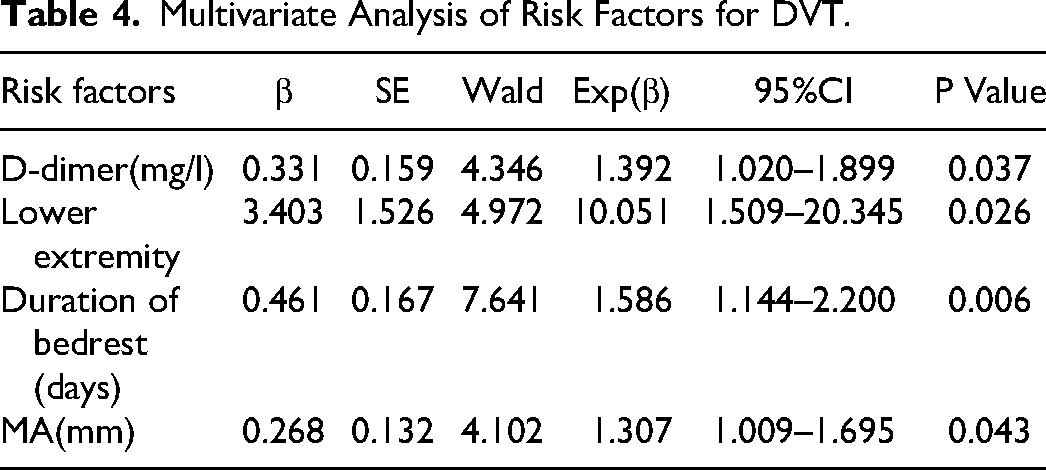
Binary logistic regression analysis of coronary heart disease, muscle strength of Lower extremity, duration of bedrestrest, operation time, D-dimer, CPR, NEUT, RDW, FIB, PT, Hypoproteinemia, R, K, Angle, MA was performed to explore the risk factors of DVT. As shown in Table 4.The results show that D-dimer (OR, 1.392; 95%CI 1.020–1.899; P < 0.05), Lower extremity (OR, 10.051; 95%CI 1.509–20.345; P < 0.05), Duration of bedrest (OR, 1.586; 95%CI 1.144–2.200; P < 0.05), MA (OR,1.307; 95%CI 1.009–1.695; P < 0.05) were independent risk factors for postoperative DVT in patients with traumatic spinal fractures combined with SCI.
Multivariate Analysis of Risk Factors for DVT.
ROC Analysis of Different Risk Factors
We used ROC analysis to determine the diagnostic value of different risk factors in postoperative DVT. The ROC curves for the four risk factors are shown in Figure 1. The AUC values indicate the diagnostic value of the predictors. D-dimer had the highest diagnostic value (AUC = 0.883). The AUC values for Lower extremity, Duration of bedrest, and MA were 0.731, 0.75, and 0.625, respectively (Table 5). For The diagnostic cut-off value was determined by the Youden index. The diagnostic cut-off value for D-dimer was 5.065 mg/L, with sensitivity of 81% and specificity of 82.7%. Other diagnostic cut-off value lower extremity < 3, duration of bedrest > 12.5 days, MA > 66.25 mm.
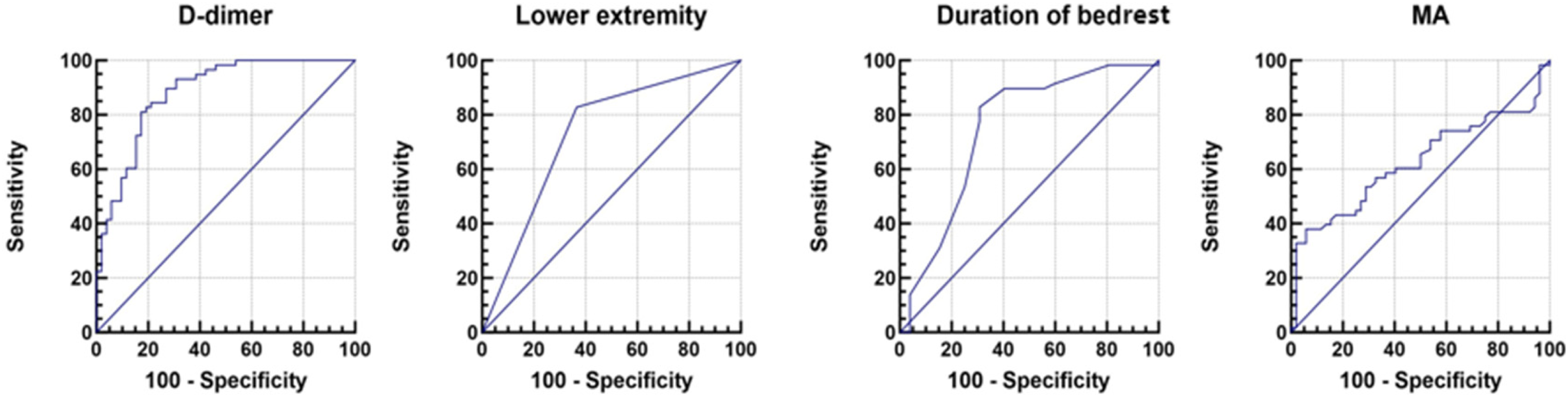
The ROC curves of different risk factors.
the ROC Results of Different Factors.

The cut-off points of scores were determined by the Youden index.
Discussion
Retrospective analysis reveals a notable postoperative DVT risk (52.7%), 7 (6.4%) proximal thrombus and 51 distal thrombus (46.4%)despite chemical and mechanical prevention of DVT. None of the patients developed pulmonary embolism or epidural hematoma. D-dimer, lower extremity, duration of bedrest and MA were independent risk factors for developing DVT. We also found that D-dimer had the highest diagnostic value among the four factors.
DVT and PE, collectively called venous thromboembolism syndrome, is one of the common complications after spinal fracture and spinal cord injury. 6 According to Virchow's triad, the three factors contributing to thrombosis are a hypercoagulable state of blood, endothelial injury of the vascular wall, and blood flow stasis.7,8 Patients with SCI have motor and sensory dysfunction below the injury plane and a loss of muscle strength in both lower limbs. Some patients have complete spinal cord injury, which will seriously affect the sympathetic control of cardiac function, leading to the reduction of myocardial contractility, reduced venous blood supply of the lower limbs, reduced effective blood volume, increased blood viscosity, and hypercoagulable blood. 9 Patients with spinal fracture need to bedrest, coupled with the lower limb motor dysfunction caused by spinal cord injury factors, weakened the function of lower limb muscle pump, slow venous blood reflux, blood stasis, easy to form a hypercoagulation state of blood, damaged vascular endothelium, platelet hyperfunction, which promotes the occurrence of DVT.10–14 Some studies have reported that the incidence of spinal cord injury is about 10.3% −62.5%. We believe that the incidence is related to the detection method and time of detection. We studied 110 patients with surgical treatment for spinal cord injury, and the incidence of DVT was 52.7%.
In our study, age, hypertension, diabetes, and somking were not found to be independent risk factors for postoperative DVT in SCI patients, which is consistent with the conclusions of some scholars.15,16 It was also found that coronary heart disease may affect the occurrence of DVT. This may be because such patients are older and have poor vascular elasticity, but combined coronary heart disease is not an independent risk factor for DVT. Coagulation indicators, HGB, albumin, and inflammation indicators in laboratory tests are not independent risk factors for DVT formation.
In our study, D-dimer > 5.065 mg/L on the first postoperative day was a risk factor for DVT after SCI. D-dimer is mainly a specific degradation product generated by the hydrolysis of fibrin monomer after cross-linking by activation factor, indicating a hypercoagulable state complicated by fibrinolysis. D-dimer is an important test for DVT diagnosis, with high negative predictive value and sensitivity, but its specificity is low because D-dimer levels can also increase in postoperative, infection, cancer, trauma, and other conditions.17,18 Although affected by many factors, the D-dimer is still considered the most powerful indicator of venous thromboembolic events. 19 Surgical procedures increase D-dimer levels, and changes are more pronounced in patients with DVT. 20 Lv et al 21 studied 175 cervical fractures with spinal cord injuries found D-dimer > 1.02 mg/L on admission as an independent risk factor for admission of DVT in SCI patients, with sensitivity 84.21% and specificity 78.10%. Masuda et al 22 using a prospective study of 211 patients with SCI, showed that 22 patients (10.4%) developed DVT. D-dimer could be used to predict the likelihood of DVT in acute cervical fracture with SCI. The optimal screening time was 2 weeks after injury, and the optimal threshold level of D-dimer for DVT 16 μg/dL. On the first postoperative day, our D-dimer > 5.065 mg/L had the highest diagnostic value (AUC = 0.883), with a sensitivity of 81% and a specificity of 82.7%. Our study only included the discussion of D-dimer on the first postoperative day, and factors such as the stimulation of surgery, the stimulation of trauma, the release of inflammatory mediators,anesthesia, intraoperative bleeding, and postoperative rehydration may all lead to the elevation of D-dimer. 23
Our study showed that lower extremity < 3 is one of the independent risk factors for postoperative DVT in SCI patients. Decreased lower extremity causes reduced muscle pump function, reduced venous blood return in the lower limbs, blood stasis, and a higher propensity for DVT. 24 Wang et al 25 research the predictors of preoperative deep vein thrombosis in 429 patients with high-energy injury suggested that lower extremity < 3 was an independent predictor of preoperative DVT, and that reduced lower extremity caused an 8.257-fold increased risk of preoperative DVT. Some scholars have studied the ossification of the posterior longitudinal ligament with acute spinal cord injury, showing that the impairment of lower limb motor function is a risk factor for DVT in the lower limbs. 26 Imyro et al 27 research 698 lumbar degenerative surgeries found that preoperativelower extremity < 3 was closely associated with the occurrence of DVT, which was consistent with our results. 27 Patients with spinal cord injury with dinnervation, complete loss of movement and sensation below the plane of injury, incomplete SCI patients with lower limb motor dysfunction. Our study patients with lower extremity < 3, the risk of postoperative DVT increased 10-fold. Therefore, patients admitted with lower extremity < 3 should take active measures to prevent DVT and reduce its incidence.
Prolonged duration of bedrest and reduced activity of the lower limbs can affect venous blood flow in the lower limbs, leading to less reflux, slower blood flow, blood stasis, and an increased likelihood of forming a hypercoagulable state, which can lead to DVT. 24 Wang et al 5 studied the risk factors for postoperative DVT in patients with thoracolumbar fractures due to high-energy injury under LMWH prevention, suggesting that time in bedrest stay > 12 days was an independent risk factor for postoperative DVT. In our study, the duration of bedrest was 14.28 ± 2.76 days in the DVT group and 10.96 ± 3.75 days in the non-DVT group. Duration of bedrest >12.5 days in SCI patients was an independent risk factor for postoperative DVT. After spinal fracture, the spine lacks stability, and patients with long-term bedrest from admission to surgery, especially those partially paralyzed with complete loss of lower limb motor function, are more prone to blood stasis and have a higher incidence of DVT in the lower limbs. Therefore, patients with SCI who retain lower limb motor function should get out of bedrest as soon as possible for functional exercise to prevent DVT.
The MA value in thromboelastogram(TEG) refers to the maximum blood clot strength and represents the maximum amplitude of the marker curve. This value reflects the maximum mechanical strength and stability of the blood clot during coagulation. The blood clot is composed of fibrin and platelets, and the amount, strength, and condensation of these components affect the MA value. However, the contribution of platelets to the MA value is larger than that of fibrinogen. 28 Liu et al 29 in elderly fracture patients found that increased MA values in TEG suggested hypercoagulable blood. In our study, we found that the MA value was 61.95 ± 10.19 mm in the DVT group and 58.16 ± 6.79 mm in the non-DVT group. The best cut-off value of MA for predicting the formation of DVT was 66.25 mm.
Finally, Only routine clinical laboratory assays were used in our study and thus our findings can be easily applied to any hospital setting.
Our current study has some limitations. First, this was a retrospective study with selection bias. Secondly, our sample size was small, and some influencing factors were not included in the study. Third, we only discussed the impact of D-dimer measurements on the first postoperative day; multiple tests before operation and on postoperative days 1, 3, and 5 should be included in future studies. Finally, future prospective studies with larger samples and multiple centers are needed to confirm our results.
Conclusion
Postoperative D-dimer > 5.065 mg/l, lower extremity < 3, duration of bedrest, MA value are independent risk factors for postoperative lower limb DVT in SCI patients, with D-dimer having the highest diagnostic value.When the above risk factors occur, clinicians need to be vigilant and take appropriate prevention and treatment measures.
Footnotes
Ethical Approval
The Ethics Committee of Yichang Central People's Hospital approved this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.