
Abstract
The purpose of this study was to investigate the prevalence of deep vein thrombosis (DVT) and to clarify the risk factors of DVT in patients with acute spinal cord injury (SCI) complicated with cervical fractures at admission. From January 2018 to December 2021, a total of 175 patients with acute SCI complicated with cervical fractures in our hospital were retrospectively analyzed. Duplex ultrasound was used to diagnose the DVT. All patients' medical record data, including demographic variables, medical history, and laboratory results, were collected. The patients were divided into DVT group and non-DVT group according to ultrasound results. The prevalence of DVT was determined and risk factors of DVT were identified. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic value of different factors. The prevalence of DVT at admission was 21.71%(38/175), including one (2.63%) with central DVT, thirty-two (84.21%) with peripheral DVT and five (13.16%) with mixed DVT. The multivariate analysis revealed that decreased lower extremity muscle strength, time from injury to admission, and D-dimer were risk factors for DVT at admission. The diagnostic value of D-dimer was the highest among these risk factors. In conclusion, in patients with acute SCI complicated with cervical fractures, the risk of DVT at admission is very high. Decreased lower extremity muscle strength, time from injury to admission, and D-dimer are risk factors for DVT. Moreover, D-dimer has the highest diagnostic value among these risk factors.
Introduction
Cervical fracture with acute spinal cord injury (SCI) is usually caused by trauma, especially high energy injury, which can lead to a variety of adverse outcomes, including physical, psychological, economic and social impairments that affect not only the patient but also their family. 1 Patients with acute SCI are at high risk for venous thromboembolism (VTE), which significantly increases their morbidity and mortality.2–4 VTE, which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), develops in 12%−64% of individuals with acute SCI and has a mortality rate of 9.7%.5,6 PE is the third leading cause of death in SCI patients, with an estimated incidence of fatal PE as high as 5%, which has drawn people's great attention. 7 However, DVT is often ignored by people because of its insidious onset and insignificant symptoms.
DVT usually occurs in the veins of the lower extremities, which can lead to chronic pain, varicose veins, post-venous thrombosis syndrome, and even PE.8,9 According to the eighth edition of the American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, patients with acute SCI have the highest risk for DVT. 10 It is reported that the incidence of DVT in patients with SCI ranged from 5% to 26%.11,12 Some studies demonstrated that the overall incidence of symptomatic or asymptomatic DVT in un-anticoagulated SCI patients ranges from 50% to 100%, with the highest incidence in the acute phase after injury.13–15 To the best of our knowledge, these studies mainly discussed the incidence of DVT in patients with cervical SCI before, after, or during the perioperative period, and the incidence of DVT at admission has not been reported.
Many studies have investigated associated risk factors of DVT for patients with cervical SCI.16–19 However, the reliability of the data is limited by differences in population size, duration of follow-up, and diagnostic methods used. A review and meta-analysis showed that middle- and old-age, male sex, complete paralysis, personal/family history of venous thrombosis, lack of compression therapy, presence of lower limb/pelvic fracture and diabetes were risk factors of VTE for patients with SCI. 16 Gariani et al 17 found that VTE associated with diabetes mainly resulted from confounders rather than an intrinsic effect of diabetes on venous thrombotic risk. Therefore, there is uncertainty about the risk factors for SCI-related DVT.
Based on the above mentions, the purpose of this study was to determine the prevalence of DVT in patients with acute SCI complicated with cervical fractures at admission, and to investigate risk factors for DVT. Specifically, we examined the diagnostic value of different factors.
Materials and Methods
Patients
We retrospectively collected electronic medical record data of 198 consecutive patients with acute SCI complicated with cervical fractures who had been admitted at Baoding No.1 Central Hospital between January 2018 and December 2021. Our hospital was the largest trauma center in the region. Our study was approved by the Ethics Committee of Baoding No.1 Central Hospital. Informed consent for our study was obtained from all patients. The study inclusion criteria were as follows: (1) acute SCI patients complicated with cervical fractures admitted to our hospital within 1 week of injury; (2) caused by trauma; (3) complete medical records.The exclusion criteria were as follows: (1) combined with multiple organ injury; (2) chronic SCI patients (>1 week); (3) anticoagulation before injury; (4) abnormality of the coagulation system; (5) a history of previous VTE; (6) presence of other sites of fractures. Overall, 23 patients were excluded from this study. Case data collection was performed by two professionally trained clinicians. Finally, a total of 175 acute SCI patients with cervical fractures were included in this study. After admission, all the patients underwent neurological investigation immediately with the Manual Muscle Test (MMT) by two senior spine surgeons and if their findings differed, they came to a conclusion after mutual consultation. The lower extremity muscle strength was calculated by adding the muscle scores of key muscle groups of lower limbs and then taking the average score, in accordance with the guideline of the American Spinal Injury Association (ASIA). 20 All the patients underwent venous ultrasound examination of the lower limbs on the day of admission or the morning of the next day. The diagnosis of DVT was made by two experienced ultrasonologists. Re-examination of ultrasonography occurred when there were different opinions.
Diagnosis of DVT
Ultrasound examination was conducted to diagnose DVT. All veins of the lower limbs were examined, including the external iliac vein, femoral vein, popliteal vein, posterior tibial vein, fibular vein, and intermuscular vein, up to the top of the Achilles tendon. All examinations were performed with the same ultrasound equipment (Philips Medical Healthcare, Armstrong, Netherlands) by the qualified radiologists. The transverse imaging plane was used to assess the compressibility of each vein and the presence of intraluminal echoes and color doppler was detected blood flow. Direct signs of thrombosis were characterized by vascular dilatation, incompressibility, low intraluminal echo, and absence of continuous doppler flow signal (Figure 1). According to venous ultrasound results, all the patients were divided into DVT group and non-DVT group. DVT was classified into three types: central DVT (in the popliteal vein or proximally), peripheral DVT (localized distal to the popliteal vein) and mixed DVT (both central and peripheral thrombosis).

Representative Doppler ultrasound images showing vascular dilatation, incompressibility, low intraluminal echo, and absence of continuous doppler flow signal
Data Collection
Demographic and clinical data were collected, including age, gender, height, weight, body mass index (BMI), comorbidities (including hypertension, diabetes and coronary heart disease), lower extremity muscle strength, cervical stenosis (including cervical spondylosis, cervical disc herniation and ossification of posterior longitudinal ligament), time from injury to admission, causes (including traffic accident, high fall, injury caused by heavy object, and fall at ground level), fibrinogen (FIB), prothrombin time (PT), thrombin time (TT), activated partial thromboplastin time (APTT), D-dimer, blood platelet (PLT) and red blood cell distribution width (RDW). D-dimer levels were assayed by photometric immunoassay method (Sysmex Chemical Medicine, Kobe, Japan) within two hours after collection from veins in the forearm.
Statistical Analysis
Statistical analysis was performed using SPSS (Version 22.0, IBM SPSS Inc., Chicago, IL, USA). The baseline characteristics were expressed as mean ± standard derivation (SD), ratio or median with interquartile range (IQR) accordingly. Continuous variables which complied with the normal distribution were compared with independent t test. Non-normally distributed continuous variables were analyzed by Mann-Whitney U test. Categorical variables were compared using the chi-square test. The variables showing P < .05 were selected into the multivariate logistic analysis which explored the risk factors of admission DVT. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic value of different factors. Values for P < .05 were defined as statistically significant.
Results
Prevalence and Distribution of Admission DVT
In 175 patients with acute SCI complicated with cervical fractures, the overall prevalence of DVT at admission was 21.71% (38/175). Of these patients, one (2.63%) had central DVT, thirty-two (84.21%) had peripheral DVT and five (13.16%) had mixed DVT. Three patients with peripheral DVT subsequently developed mixed DVT, and no patients developed symptomatic PE in the study. The specific thrombosis distribution was as follows: femoral vein thrombosis in 4 cases, popliteal vein thrombosis in 3 cases, posterior tibial vein thrombosis in 4 cases, fibular vein thrombosis in 3 cases and intermuscular vein thrombosis in 30 cases.
Univariate Analysis of Admission DVT
As shown in Table 1, the average age in the DVT group was 58.7 ± 11.9 whereas that in the non-DVT group was 52.6 ± 13.5. It showed that patients with DVT were older than those without DVT (P = .012). There was a significant difference in lower extremity muscle strength between the two groups (P < .001). Compared with the non-DVT group, more patients in the DVT group had cervical stenosis (P < .001). Time from injury to admission was significantly different between the two groups:1.83 ± 0.78 days versus 0.98 ± 0.46 days, respectively (P < .001). No significant differences were observed in gender, BMI, causes, diabetes, hypertension and coronary heart disease between the two groups (all P > .05).
Demographic Data of Patients between the Two Groups

Values are presented as mean ± standard deviation or number (%).
t Value or χ2 Value.
Manual muscle test score (0-5).
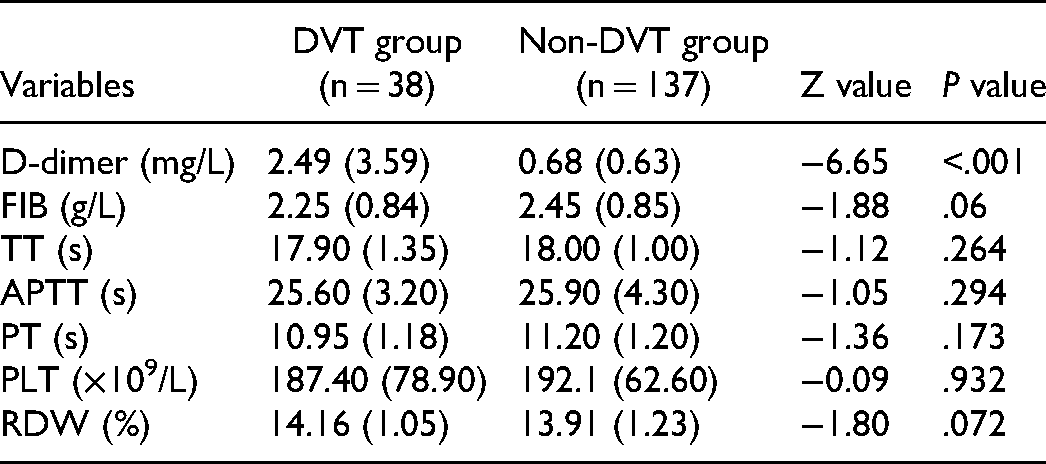
The DVT group had a significantly higher level of D-dimer than the non-DVT group (2.49 mg/L (IQR = 3.59) versus 0.68 mg/L (IQR = 0.63); P < .001).However, there were no significant differences between the two groups in FIB, TT, APTT, RDW and PLT (all P > .05) (Table 2).
Laboratory Results of Patients between the Two Groups
Multivariate Analysis of Admission DVT
Logistic regression analysis was conducted to explore risk factors by entering age, lower extremity muscle strength, time from injury to admission, cervical stenosis and D-dimer. As shown in Table 3, the results showed that lower extremity muscle strength (OR,5.080;95%CI:1.560-16.545; P = .007), time from injury to admission (OR,9.013;95%CI:3.746-21.683; P < .001) and D-dimer (OR,1.849;95%CI:1.361-2.512; P < .001) were risk factors for admission DVT.
Multivariable Analysis of the Risk Factors for DVT at Admission

ROC Analysis of Different Risk Factors
The ROC curves of the four risk factors were shown in Figure 2. The value of AUC (area under the ROC curves) usually indicates the diagnostic value of the risk factors.The diagnostic value of D-dimer (AUC value = 0.853) was the highest one among these factors.The AUC value of lower extremity muscle strength and time from injury to admission was 0.697 and 0.843, respectively (Table 4). The diagnostic cut-off value was determined by the Youden index, which was less than 3 score in lower extremity muscle strength, more than 1.4 days in time from injury to admission and 1.02 mg/L in D-dimer, respectively.

The ROC curves of different risk factors
The ROC Results of Different Factors

The cut-off points of scores were determined by the Youden index.
Discussion
The results of this retrospective study confirmed a high risk of DVT at admission (21.71%) for acute SCI complicated with cervical fractures. Decreased lower extremity muscle strength, time from injury to admission, and D-dimer were risk factors for DVT. We also found D-dimer has the highest diagnostic value among these three factors.
Acute cervical SCI is usually complicated with cervical fracture, which can lead to serious complications for patients. 21 DVT and PE are common and devastating complications after acute SCI. It is known that the formation of DVT is mainly due to the classical three factors known as Virchow's triad: endothelial dysfunction, hypercoagulability and venous stasis. 22 Two factors lead to the occurrence of VTE in SCI patients: one is that prolonged bed rest and motor impairment both lead to decreased lower extremity activities, resulting in circulatory stagnation; the other is that the pain and clinical symptoms of SCI patients are reduced. 6 The prevalence of DVT after acute SCI has been discussed by many researches, which mainly concentrate upon perioperative or postoperative period.2,4,12–14 To our knowledge, this is the first retrospective study to evaluate the admission prevalence and risk factors of DVT in patients with acute SCI complicated with cervical fractures.
A number of previous studies have reported the incidence of DVT in SCI patients, which was of a broad spectrum (range: 2%-100%).12–14,19,23,24 We thought the variation of DVT incidence depended on the surveillance methods, time after injury and DVT prophylaxis. A systematic review indicated that the risk for DVT was greatest during the first two weeks after injury. 5 One previous study of 148 patients by Lowery et al 25 found the prevalence of VTE in patients with acute SCI who were in an urban inner city was 19.59%. Jones et al, 14 in their retrospective study, found the prevalence of VTE was 5.4% in 16 240 adults and children after SCI. To our knowledge, this is the largest study of VTE after cervical SCI to date. Sugimoto et al 24 demonstrated the incidence of DVT in cervical SCI patients caused by trauma was 21% surveilled by doppler ultrasonography. A recent study investigated the incidence of VTE after acute cervical SCI in patients with ossification of the posterior longitudinal ligament (OPLL), and they found the incidence of VTE in the OPLL group was as high as 50%. 6 In the current study, the prevalence of DVT with cervical fractures was 21.71% at admission, which was consistent with previous research.
In this study, we found that time from injury to admission, lower extremity muscle strength and D-dimer were risk factors for DVT at admission. Older age was often considered one of the risk factors for DVT after SCI.13,19,26 Giorgi Pierfranceschi et al 26 reported that age over 45 years was a risk factor of VTE in patients with SCI. In our study, the mean age of the DVT group was 58.71 ± 11.91 years old, and that of the non-DVT group was 52.58 ± 13.46 years old, with statistically significant differences. But the multivariate analysis didn't demonstrate age was a risk factor for DVT, which was consistent with the research by Wei et al. 16 This may be due to the small sample size and the older age (mean age >45 years) of patients with SCI complicated with cervical fracture. BMI, causes of injury, and gender were not risk factors for DVT at admission, which was consistent with some previous studies.25,27 Our study also found that hypertension, diabetes and coronary heart disease were not associated with DVT, which may be due to the low number of these events. We found that cervical stenosis was closely associated with DVT, but was not a risk factor for DVT. Similar to our results, Ichikawa et al 6 found that SCI patients with OPLL had a high incidence of DVT. They speculated that this may be related to endothelial dysfunction, so this needs further research to confirm.
In our study, the multivariate analysis demonstrated that lower extremity muscle strength <3 was a risk factor for DVT at admission. We also revealed that compared with lower extremity muscle strength ≥3, decreased lower extremity muscle strength led to a 5-fold increase in the risk of DVT. The venous blood of the lower extremities can return to the heart mainly rely on the function of the muscle pump. Paralysis of the lower extremities can weaken the muscle pump function, reduce blood flow, and promote the formation of DVT. One previous retrospective study showed that paraplegia was independently associated with the occurrence of VTE. 26 Another study of 222 patients by Clements et al 27 found statistically significant association between VTE and completeness of motor paralysis. Therefore, for patients with impaired muscle strength of lower extremities, early thromboembolism prevention is necessary.
Previous studies demonstrated that delayed admission to hospital was considered a risk factor for DVT in patients with fractures.28,29 Clements et al, 30 in their study between 2010 and 2013, found that there was a statistically significant association between DVT and time from injury to admission for SCI patients. In their study, the mean time from injury to admission in the DVT group was 3.5 days whereas that in the non-DVT group was 1.0 days. In our study, although the time from injury to admission was short, we still found it was a risk factor for DVT. We also found that time from injury to admission greater than 1.4 days had the greatest diagnostic efficacy (sensitivity 68.42%, specificity 90.51%). The possible reasons were that delayed admission could lead to the failure of timely application of measures to prevent DVT, and with the development of time, patients’ increased fluid loss, prolonged bed time and long-term blood stasis may increase the occurrence of DVT in lower extremity.
We did find an association between D-dimer level and risk of DVT at admission. One research discovered that for patients with SCI during rehabilitation, only high D-dimer upon admission was associated with risk of VTE. 31 Masuda et al 32 showed that the cut-off level of D-dimer was 16 µg/dL on day 14 after injury in patients with SCI and demonstrated that the sensitivity and specificity were 77.3% and 69.2%, respectively. In the current study, we determined that the optimal cut-off point of D-dimer was 1.02 mg/L, because of a good balance between sensitivity and specificity (sensitivity 84.21%, specificity 78.10%). The diagnostic value of D-dimer (AUC value = 0.853) was the highest one among these factors. Therefore, for patients with D-dimer greater than 1.02 mg/L at admission, venous ultrasound examination of lower extremity should be performed as soon as possible, and preventive measures should be taken early.
There were some limitations in our study. First, this was a retrospective study, which inherently leads to observer bias and selection bias. Second, the study was carried out at a single hospital, and the sample size was small, so some important variables may not have been included in the study. Third, ultrasound examination has the potential problem of biased results due to its dependence on the clinical skills of investigators.
Conclusions
In patients with acute SCI complicated with cervical fractures, the risk of DVT at admission is very high. Decreased lower extremity muscle strength, time from injury to admission, and D-dimer are risk factors for DVT. Moreover, D-dimer has the highest diagnostic value among these risk factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Ethics Committee of Baoding No.1 Central Hospital approved this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Baoding City Science and Technology and Intellectual Property Bureau (grant number 2041ZF100).