
Abstract
To identify risk factors of admission deep vein thrombosis (DVT) in patients with traumatic fractures. Medical records of 1596 patients with traumatic fractures were reviewed. According to the ultrasound reports of the lower extremity veins, patients were assigned to the DVT or non-DVT group. Univariate and multivariate logistic regression analyses were used to identify the independent risk factors of DVT, and the receiver operating characteristic (ROC) curve was used to analyze the predictive value of the D-dimer level for DVT. DVT admission incidence was 20.67%. Statistically significant differences were revealed between the 2 groups in terms of age, sex, fracture site, presence of hypertension, coronary heart disease, stroke, smoking status, time from injury to admission, and levels of fasting blood glucose, hemoglobin, fibrinogen, D-dimer, and hematocrit. Multivariate analysis results showed that age above 50 years, female, above-knee fracture, cigarette smoking, injury-to-admission delay beyond 48 h, low hemoglobin levels, high fasting blood glucose levels, and high D-dimer levels were independent risk factors for admission DVT. ROC analysis showed that the D-dimer level was effective for the prediction of admission DVT in patients with peri-knee and below-knee fractures (area under the curve [AUC] = 0.7296, cutoff point = 1.21 mg/L). An age over 50 years, female, above-knee fracture, smoking, injury-to-admission delay beyond 48 h, decreased hemoglobin level, and increased fasting blood glucose and D-dimer levels were found to be potential independent risk factors for admission DVT. In patients with peri-knee and below-knee fractures, the plasma D-dimer level was effective in predicting admission DVT.
Introduction
Deep vein thrombosis (DVT) is a common complication in trauma patients. The incidence of DVT after trauma was reported to be approximately 9.1% to 61.0%.1–3 Pulmonary embolism (PE), a serious complication in trauma patients, can cause significant mortality and can occur within 72 h after injury. 4 Research reported that the incidence of early posttraumatic PE could be up to 10% to 42%, and fatality from PE was close to 50%. 5 It is well known that DVT is the main risk factor for PE. 6 Therefore, early prediction and intervention of DVT in high-risk patients with traumatic fractures have considerable clinical significance. Previous studies have mostly focused on preoperative DVT, while less attention has been paid to DVT that might have occurred at admission.7–9 Thus, it is necessary to conduct research to identify the risk factors of admission DVT in patients with traumatic fractures. In addition, most of these studies have focused on fractures at a certain site; however, the incidence of DVT was related to the fracture sites.10,11 Emergency physicians encounter patients with various fractures and need to initially screen for DVT risk factors. Therefore, it is also necessary to conduct research that includes fractures at all sites.
Clinically, D-dimer, as an indicator of thrombosis, is used to detect and screen venous thrombosis. 12 However, except for venous thrombosis, elevated levels of D-dimer are also found in patients in whom coagulation and fibrinolysis are co-activated, such as those with recent trauma or surgery and those with severe sepsis. 13 Thus, the predictive value of D-dimer level for admission DVT in patients with traumatic fractures is worth studying.
The aim of this study was to identify the risk factors of admission DVT in patients with traumatic fractures and investigate whether the D-dimer level was effective for the prediction of admission DVT, which will be conducive to the formulation of an early prophylaxis and treatment plan for DVT.
Materials and Methods
This study was approved by our institutional review board. In this retrospective study, the medical records of patients with traumatic fractures who were hospitalized in 3 hospitals between April 2020 and April 2022 were reviewed. The study sample consisted of 1596 patients who met the inclusion and exclusion criteria. Inclusion criteria consisted of the following: (1) patients diagnosed with a traumatic fracture; (2) patients who underwent fasting blood glucose, routine blood tests, and coagulation tests at admission; (3) patients who were examined via whole-leg compression ultrasound to detect DVT at admission. Exclusion criteria comprised the following: (1) patients with an open wound or neurovascular injury; (2) patients with unstable vital signs at admission; (3) patients with combined injuries and multiple fractures; (4) patients with a history of PE or DVT; (5) patients with tumors or who were pregnant; (6) patients who underwent long-term anticoagulation; and (7) patients with incomplete clinical data. The selection process is illustrated in Figure 1.

Process of selecting the study subjects.
Data Collection
Patient data were retrieved using electronic medical records, including age, sex, height, weight, fracture site, complications (including hypertension, diabetes, coronary heart disease, and stroke), smoking status, time from injury to admission, serum markers at admission (including fasting blood glucose, hemoglobin, hematocrit, platelets, fibrinogen, and D-dimer), and an ultrasound report of the lower extremity veins at admission. Fracture sites were categorized as ankle–foot fractures (including ankle joint and foot fractures), tibia–fibula fractures, peri-knee fractures (including femoral condyle, patellar, and tibial plateau fractures), femoral shaft fractures, peri-hip fractures (including femoral neck, femoral intertrochanteric, and acetabular fractures), and pelvic fractures. According to the ultrasound reports, the patients were divided into the DVT or non-DVT group.
Statistical Analysis
All data were analyzed using SPSS® for Windows (version 18; SPSS Inc., Chicago, IL, USA). The measurement data of clinical indices were expressed as mean ± standard deviation (SD) and analyzed using independent samples t-tests. Count data were expressed as numbers (percentages) and analyzed using the chi-square test. Factors with a P < .05 in the univariate analysis were selected for logistic multivariate regression analysis. The receiver operating characteristic (ROC) curve was used to assess the predictive value of the D-dimer level for admission DVT. The cutoff points were selected according to the maximum Youden index. Sensitivity and specificity for DVT diagnosis were also measured. Statistical significance was set at P < .05.
Results
Patient Demographic and Clinical Characteristics
A total of 1596 patients were enrolled, including 726 (45.49%) women and 870 (54.51%) men, with an average age of 57.16 years (SD, 18.41; range, 16-96; median, 51.0) and an average body mass index (BMI) of 23.43 kg/m2 (SD, 3.59; range, 14.17-39.52). Of the 1596 patients, 348 had ankle–foot fractures, 232 had tibia–fibula fractures, 308 had peri-knee fractures, 167 had femoral shaft fractures, 311 had peri-hip fractures, and 230 had pelvic fractures.
Incidence of DVT
The incidence of admission DVT in patients with traumatic fractures was 20.67% (330 of 1596), and proximal DVT was detected in 59 (3.68%) patients. The incidence rates of admission DVT were 14.36% (50 of 348), 12.06% (28 of 232), 14.28% (44 of 308), 32.33% (54 of 167), 27.65% (86 of 311), and 29.56% (68 of 230) in patients with ankle–foot, tibia–fibula, peri-knee, femoral shaft, peri-hip, and pelvic fractures, respectively. Proximal DVT was detected in 0.00% (0 of 348) of patients with ankle–foot fractures, 0.00% (0 of 232) with tibia–fibula fractures, 1.94% (6 of 308) with peri-knee fractures, 9.58% (16 of 167) with femoral shaft fractures, 5.78% (18 of 311) with peri-hip fractures, and 8.26% (19 of 230) with pelvic fractures. Of all the DVT cases. symptomatic DVT was found in 29 patients (8.78%). Three patients (2 with peri-hip fractures and 1 with a pelvic fracture) with proximal DVT developed dyspnoea, tachypnoea, and chest pain, and were diagnosed with PE by computed tomography pulmonary angiogram (CTPA) within 24 h after admission.
Of the 1596 patients, 75 (4.69%) had DVT in both lower extremities; 6 (0.86%) had ankle–foot fractures, 3 (1.29%) had tibia–fibula fractures, 3 (0.97%) had peri-knee fractures, 9 (5.38%) had femoral shaft fractures, 30 (9.64%) had peri-hip fractures, and 27 (11.73%) had pelvic fractures.
Univariate Analysis of Risk Factors
The results of the univariate analysis are provided in Table 1. Based on age, the patients were divided into 4 groups: age ≤ 25 years, 26 years ≤ age ≤ 50 years, 51 years ≤ age ≤ 75 years, and age ≥ 76 years; the incidence rates of DVT were 6.45%, 10.35%, 29.72%, and 33.83%, respectively (P < .001). Women had a higher incidence of DVT (25.89% vs 16.32%, P < .001). There was a statistically significant difference between the fracture sites of patients with and without DVT (P < .001).
Demographic Characteristics and Risk Factors Associated With Admission DVT.

Abbreviations: DVT, deep vein thrombosis; BMI, body mass index.
Coronary heart disease includes chronic myocardial ischemia, ST segment changes without clinical symptoms, and delayed myocardial infarction in electrocardiograms. b Stroke includes fresh and delayed cerebral ischemia and hemorrhage in computed tomography or magnetic resonance imaging.
Regarding comorbidities, patients with DVT had a higher prevalence of hypertension (23.03% vs 11.69%, P < .001), coronary heart disease (20.00% vs 15.48%, P = .048), and stroke (23.03% vs 13.42%, P = .048) than those without DVT. In addition, the incidence of cigarette smoking was higher in patients with DVT (11.51% vs 8.05%, P = .048) than in patients without DVT.
The average time from injury to admission was 25.04 h (SD, 20.46; range, 1.00-72.00; median, 24.00). Based on the time from injury to admission, the patients were divided into 3 groups: time from injury to admission ≤ 24 h, 24 h < time from injury to admission ≤ 48 h, and time from injury to admission >48 h; the incidence rates of DVT were 16.50%, 11.73%, and 62.80%, respectively (P < .05).
Patients with DVT had a lower hematocrit level (38.04 ± 5.45% vs 39.18 ± 5.85%, P = .001) and hemoglobin level (117.79 ± 17.59 g/L vs 127.31 ± 22.59 g/L, P < .001), and a higher fasting blood glucose level (7.16 ± 2.92 mmol/L vs 6.31 ± 2.16 mmol/L, P < .001), fibrinogen level (3.83 ± 1.28 g/L vs 3.42 ± 1.15 g/L, P < .001), and D-dimer level (3.64 ± 3.82 mg/L vs 2.40 ± 3.86 mg/L, P < .001) than patients without DVT.
No statistically significant differences were found in BMI, diabetes, or platelet levels between patients with and without DVT (P > .05).
Multivariate Analysis of Risk Factors
The results of the multivariate analysis are provided in Table 2; they showed that an age above 50 years (age: 51-75, odds ratio [OR] = 6.260, 95% confidence interval [CI] 2.565-15.279, P < .001; age: ≥ 76, OR = 5.50, 95% CI 2.098-14.421, P = .001), female sex (OR = 1.434, 95% CI 1.023-2.010, P = .037), above-knee fracture (femoral shaft fractures: OR = 2.242, 95% CI 1.343-3.742, P = .002; peri-hip fractures: OR = 1.491, 95% CI 1.106-1.913, P = .036; pelvic fractures: OR = 1.796, 95% CI 1.114-2.896, P = .016), cigarette smoking (OR = 2.345, 95% CI 1.442-3.815, P = .001), and injury-to-admission delay beyond 48 h (OR = 9.195, 95% CI 6.119-13.817, P < .001) were independent risk factors for admission DVT.
Multivariate Logistic Regression Analysis for Risk Factors Associated With Admission DVT.

Abbreviation: DVT, deep vein thrombosis.
A higher hemoglobin level (OR = .989, 95% CI 0.983-0.996, P = .002) decreased the risk of admission DVT, while high fasting blood glucose levels (OR = 1.052, 95% CI 1.0185-1.087, P = .002) and high D-dimer levels (OR = 1.136, 95% CI 1.062-1.214, P < .001) were independent risk factors for admission DVT.
ROC Curve Analysis for D-dimer Value
Based on the fracture site, the patients were divided into 2 groups: patients with peri-knee and below-knee fractures (including ankle–foot and tibia–fibula fractures) and patients with above-knee fractures (including femoral shaft, peri-hip, and pelvic fractures). ROC analysis showed that the D-dimer level was effective for the prediction of admission DVT in patients with peri-knee and below-knee fractures, with an area under the curve (AUC) of 0.7296 and a cutoff point of 1.21 mg/L (sensitivity of 0.861 and specificity of 0.678) (Figure 2). In patients with above-knee fractures, the D-dimer level had a low value in predicting admission DVT, with an AUC of 0.614 and a cutoff point of 2.09 mg/L (sensitivity of 0.704 and specificity of 0.596) (Figure 3).
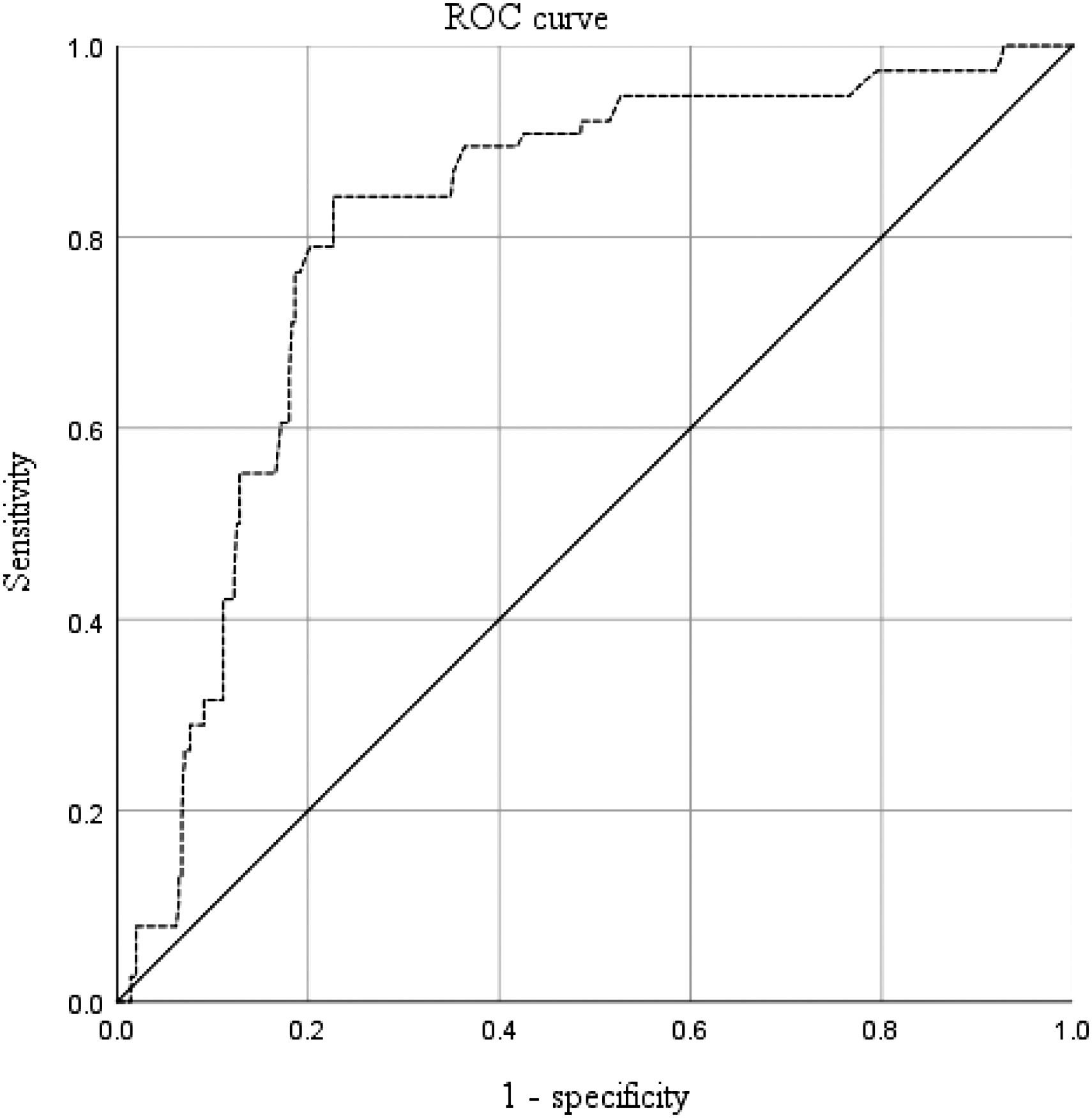
The predictive value of D-dimer level for admission deep vein thrombosis (DVT) in patients with peri-knee and below-knee fractures.
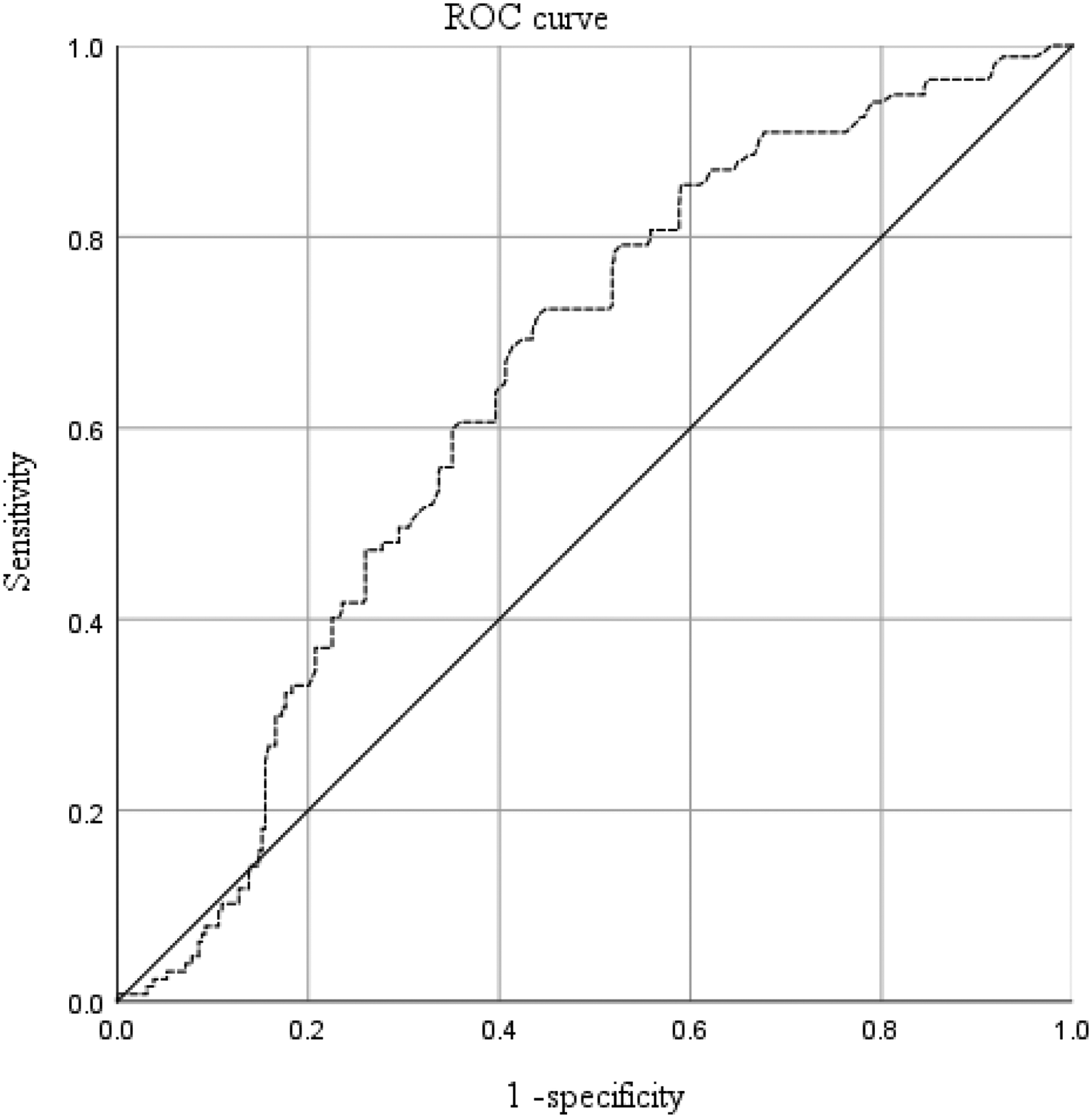
The predictive value of D-dimer level for admission deep vein thrombosis (DVT) in patients with above-knee fractures.
Discussion
Incidence of DVT
The incidence of DVT at admission in patients with traumatic fractures was 20.67%, and the respective incidence rates of DVT at admission were 14.36%, 12.06%, 14.28%, 32.33%, 27.65%, and 29.56% in patients with ankle–foot, tibia–fibula, peri-knee, femoral shaft, peri-hip, and pelvic fractures, which were lower than the preoperative incidence rates of DVT reported in previous studies.10,11 In such cases, the incidence rate of preoperative DVT was 35.0%, and in patients with ankle–foot, peri-knee, peri-hip, and pelvic fractures, the preoperative incidence rates of DVT were 23.6%, 42.0%, 36.8%, and 35%, respectively. This indicates that a certain proportion of patients with traumatic fractures develop DVT during the period from admission to surgery, and the long waiting time from admission to surgery may be a factor leading to the high incidence of preoperative DVT in patients with traumatic fractures. Therefore, surgery should be scheduled as soon as possible (if allowed) for patients with traumatic fractures. In addition, this study found that a proportion of patients had DVT in both lower extremities, especially those with the femoral shaft, peri-hip, and pelvic fractures. Therefore, for patients with above-knee fractures, attention should be paid to the formation of thrombosis in both lower limbs.
Risk Factors of Admission DVT
Study results on the effects of age on DVT are inconsistent. A study by Xia et al 14 demonstrated that there was no significant relationship between age and DVT in elderly patients with traumatic fractures. Even in studies that confirmed age as an independent risk factor for DVT, there was disagreement about the specific cutoff value for age. Chang et al 15 demonstrated that age above 60 years was an independently associated factor for DVT. Kim et al 16 reported a significant increase in the incidence of DVT in patients with pelvic and acetabular fractures over 50 years of age. In a study by Montgomery et al, 17 it was reported that patients above 30 years of age had a higher risk of developing DVT. By comparing these studies, we found that much of this discrepancy is related to the patient demographic. Xia et al reported that the study population consisted of elderly patients, while Montgomery et al reported that the study population consisted of adult patients. In the present study, elderly and adult patients with traumatic fractures were included, with an average age of 57.16 years (SD, 18.41; range, 16-96; median, 51.0), and we found that a traumatic fracture at age > 50 years was an independent risk factor for admission DVT. Furthermore, this study showed that the female sex was an independent risk factor for the development of admission DVT. This may be related to the higher level of platelet activity in women than in men. 18 In addition, some studies found that DVT was significantly associated with common iliac vein obstruction, and there were more females than males with the common iliac vein (CIV) compression of 70% or more.19,20
An above-knee fracture was also found to be an independent risk factor for DVT at admission in our study. There are 2 possible reasons for this result: firstly, femoral neck and femoral intertrochanteric fractures were more common in patients with advanced age, which contributed to the high occurrence of DVT21,22; secondly, femoral shaft, acetabular, and pelvic fractures are mostly caused by violence, which can cause relatively severe vascular endothelial damage. 23 In addition, our study demonstrated that proximal thrombosis, as an independent risk factor for PE, 24 had a higher incidence in patients with above-knee fractures. Therefore, in patients with traumatic fractures, special attention should be paid to those with above-knee fractures, and early prophylaxis and treatment plans should be formulated to prevent clot extension and acute PE.
Univariate analysis showed that there were significant differences in the incidence of DVT at admission between patients with and those without hypertension, coronary heart disease, and stroke. However, logistic multivariate analysis showed that hypertension, coronary heart disease, and stroke were not independent risk factors for DVT at admission in patients with traumatic fractures. It is speculated that this may be related to the increased prevalence of hypertension, coronary heart disease, and stroke with age.
Most studies have found diabetes to be an independent risk factor for DVT.15,25 There are 2 main theories to explain this result: first, patients with diabetes need to regulate blood glucose before surgery, which increases the preoperative preparation time and risk of DVT 26 ; second, the body is under stress after a fracture, and the blood glucose of patients with diabetes undergoes extensive changes, which leads to the release of a large number of cytokines and activation of the coagulation system in the body, resulting in increased platelet activation. 27 In this study, a significant difference was not found in the incidence of admission DVT between patients with and those without diabetes, but it was observed that higher glucose levels increased the risk of DVT. Based on the above, we hypothesized that diabetes itself is not a risk factor for DVT, whereas increased preoperative preparation time and large blood glucose fluctuations are risk factors for admission to DVT. Therefore, it is necessary to control blood glucose levels over time and effectively in these patients with diabetes and poor blood glucose control at admission.
At present, the results of studies on the relationship between time from injury to admission and DVT are inconsistent. An observational study by Zhang et al did not demonstrate a significant relationship between time from injury to admission and DVT, which was not in accordance with the research findings of Fan et al and Wei et al.10,28,29 Fan et al and Wei et al found that a longer time from injury to admission was a vital contributing factor to thrombosis. Our study demonstrated that a time from injury to admission > 48 h was an independent risk factor for DVT. In the studies by Fan et al and Wei et al, the mean number of days between fracture and hospitalization in the DVT group were above 2.10 and 2.49 days, respectively, while in Zhang et al's study, the mean number of days between fracture and hospitalization was 1.70 days (below 48 h). Therefore, it is likely that a cut-off value (48 h) of time from injury to admission exists, above which the risk of DVT increases significantly.
The present study found that a lower hemoglobin level increased the risk of admission to DVT. Anemia as a cause of venous thromboembolism is supported by several studies.30,31 In addition, lower hemoglobin levels might be due to severe trauma, which is an independent risk factor for DVT. 32 D-dimer level is an important indicator of fibrinolytic activity, reflecting the hypercoagulable state and fibrinolytic activity of the body. Our study demonstrated that an increased D-dimer level was an independent risk factor for DVT at admission in patients with traumatic fractures, which is consistent with the results of Zuo and Hu. 33 They found that a D-dimer level > 1.44 mg/L increased the risk of admission DVT in elderly patients with intertrochanteric fractures.
The Predictive Value of D-dimer for DVT
In this study, we found that the plasma D-dimer level at admission was effective for the prediction of DVT in patients with peri-knee and below-knee fractures; however, the D-dimer level had a low value in predicting DVT at admission in patients with above-knee fractures. Age and trauma may have contributed to these differences. Additionally, hip fractures are more common in elderly patients. 21 Lin et al found that the plasma D-dimer level was effective for the prediction of DVT in patients with fractures aged ≤ 60 years and D-dimer level had a low value in predicting DVT in patients with fractures over 60 years of age. 34 Furthermore, according to the abbreviated injury scale (AIS), AIS = 2 in patients with peri-knee and below-knee fractures (except femoral condyle fractures), and AIS = 3 in patients with above-knee fractures (except simple pelvic fractures). 35 Thus, above-knee fractures are more traumatic than peri-knee and below-knee fractures. The D-dimer level increased with the degree of trauma;36 therefore, in patients with above-knee fractures, the change in D-dimer level may be mainly caused by severe trauma, which affects the predictive value of D-dimer for DVT.
Limitations of This Study
This study had several limitations. First, the retrospective design has its inherent limitation of accuracy in data collection. Second, patients with combined injuries and multiple fractures were excluded, limiting broader applications. We will include patients with chest, abdominal, brain, and extremity injuries, as well as multiple fractures, for analysis in the future. Third, dynamic observations of D-dimer levels were lacking in this study; the predictive value of dynamic changes in D-dimer level for DVT is also worthy of further investigation. Fourth, this study only identified the risk factors of admission DVT in patients with traumatic fractures; external validation studies are still lacking.
Conclusions
The incidence of DVT at admission in patients with traumatic fractures was 20.67%. Age above 50 years, female sex, above-knee fracture, smoking, injury-to-admission delay beyond 48 h, decreased hemoglobin level, and increased fasting blood glucose and D-dimer levels were found to be potential risk factors for admission DVT in patients with traumatic fractures. In addition, the plasma D-dimer level was effective in the prediction of admission DVT in patients with peri-knee and below-knee fractures, and the cutoff point was 1.21 mg/L, with a sensitivity of 0.861 and a specificity of 0.678. These epidemiologic data are helpful in the assessment and risk stratification of admission DVT, and in supporting the formulation of an early prophylaxis and treatment plan for DVT.
Footnotes
Authors’ Note
Li Zhang and Xiaobing Liu contributed equally to this work.
Data Availability Statement
All de-identified data supporting the analyses in this study are contained in the tables published in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Key Research and Development Project of Shaanxi Province (no. 2023-YBSF-069) and the Key Research and Development Project of Shaanxi Province (no. 2022SF-149).