
Abstract
Hepatocellular carcinoma (HCC) is associated with higher mortality as a result of poor prognosis and unavailability of effective treatment options. This study retrospectively analyzed the clinical value of platelet-to-lymphocyte ratio (PLR) to aid in differentiating early hepatocellular carcinoma from liver cirrhosis patients. Three hundred and nine (309) patients including 155 patients with hepatocellular carcinoma (HCC) and 154 patients with liver cirrhosis were enrolled in this study. General clinical characteristics and blood parameters of each patient were collected, calculated, and retrospectively analyzed. Mann–Whitney U test was calculated to compare the two groups. Receiver operating characteristics (ROC) curve was performed to investigate the diagnostic potential of PLR in the prediction of HCC at a cut-off with high accuracy (area under the curve [AUC]) > 0.80. Hemoglobin (HB) concentration, red blood cell (RBC) count, neutrophil (NEU) count, platelet count, platelet-to-lymphocyte ratio (PLR), and neutrophil-to-lymphocyte ratio (NLR) were significantly higher in the HCC patients than in the liver cirrhosis patients (p < 0.05). ROC curve analysis showed that the AUC, optimal cut-off value, sensitivity, and specificity of PLR to predict HCC patients were 0.912, 98.7, 81.2%, and 80.6% respectively. The results suggest that PLR is a potential biomarker that can be used to predict early HCC.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is the fifth most prevalent malignancy associated with high mortality and morbidity rates1,2 and accounts for approximately 90% of liver cancer prevalence. 3 HCC is the fifth most frequently reported malignancy in males, and the ninth most frequently reported malignancy in females. It is characterized by a high mortality rate, which is primarily attributable to the poor prognosis and indication of ineffective treatment protocols. 4 The worldwide incidence of HCC varies from region to region, notably because of the multifactorial risk factors. Exposure to aflatoxin B1 and hepatitis B among the sub-Saharan African and Asian populations increases the incidence of HCC in patients with hepatitis B in approximately 80% of the cases, with an increase in viral load and severity of the liver disease. In contrast, the associated risk factors among European and United States populations are uncontrolled alcohol abuse and hepatitis C. 5
Despite numerous global techniques, advancements, and innovations in modern surgical procedures and perioperative management of HCC cases, the prognosis for this cancer remains dismal.6,7
Inflammation plays a crucial role in the development and pathogenesis of cancer, as well as in its progression and metastasis.8–11 Serum ferritin (SF), neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), and platelet-to-lymphocyte ratio (PLR) are well-known and established markers of inflammation that have been identified and reported in numerous studies in various cancers.6–8,12,13 Other studies have shown that platelets play a role in inflammation. By increasing platelet levels, the promotion of neoangiogenesis and the production of adhesion molecules contribute to cancer progression and an increase in early metastasis. In contrast, lymphocytes inhibit malignant progression through tumoral infiltration. For this reason, patients with advanced forms of cancer present with low lymphocyte counts. 6 Malignant diseases are characterized with increased burden of inflammation. 14 PLR is also associated with malignancy 15 and inflammatory conditions such as irritable bowel disease, 16 and other gastrointestinal conditions, 17 thyroiditis, 18 and other thyroid conditions, 19 diabetes mellitus, 20 and COVID-19 infection. 21 NLR also reflects the inflammatory burden in inflammatory bowel disease, 22 diabetes mellitus, 23 thyroiditis, 24 and SARS Cov2 infection. 25 All of these conditions are associated with inflammation as hepatocellular carcinoma is 26
The platelet-to-lymphocyte ratio (PLR) is a widely used biomarker for evaluating inflammatory and immune responses and is generally reported as a prognostic factor in malignancies. In addition, higher values of PLR are associated with unfavorable clinical features in patients with HCC. 27 Few reports on the PLR are used to predict HCC in liver cirrhosis patients. According to a recent report, PLR is a good indicator of mortality and relapse-free survival in HCC transplant patients. 28 Another report demonstrated the usefulness of PLR for predicting mortality in Black African patients with HCC at an advanced stage. 29 Therefore, in this study we explore the diagnostic value of PLR in the prediction of early HCC.
Materials and Methods
Three hundred nine patients admitted to the Jingzhou Central Hospital, Hubei province, between January 2021 and December 2022 were enrolled in this study. One hundred and fifty-five patients were in the HCC group, and one hundred and fifty-four were patients with liver cirrhosis. The inclusion criteria for the HCC group were as follows: (a) HCC diagnosis confirmed by ultrasound recognition of nodules >10 mm in the liver, liver function test followed by diagnostic dynamic computed tomography (CT) and Magnified resonance imaging (MRI) following the guidelines of the American Association for the Study of Liver Diseases, 30 liver cirrhosis (LC) group with (1) imaging of cirrhosis or portal hypertension, such as splenomegaly, portal vein 1.3 cm, (2) meeting two or more of the (a) Platelet (PLT) < 100 × 10*9/L; (b) Serum albumin (ALB) < 35 g/L excluding malnutrition or kidney disease, and (3) aspartate aminotransferase (AST)/PLT ratio index (APRI) > 2 according to the Chinese guidelines on the management of liver cirrhosis. 31 Patients treated with surgery or all patients who took antitumor drugs before plasma collection, patients on anticoagulants or had a blood transfusion within one month of the initiation of this study, and patients with all other forms of malignancies were exempted from the study. Blood samples of the study patients were taken into EDTA-K2 anticoagulant tubes. Sysmex XN3000 was used to measure hemoglobin (HB), red blood cell (RBC) count, lymphocytes (LYM), platelets (PLT), and neutrophils (NEU). Additionally, derived hematological profiles such as PLR were calculated by dividing the absolute number of platelets by the total number of lymphocytes and NLR by the whole number of neutrophils by the unlimited number of lymphocytes.
The data was analyzed using version 26 of IBM SPSS Statistics. The Kolmogorov-Smirnov test was used to determine the normality of distribution and Continuous variables were expressed as mean ± standard deviation, and their statistical difference was estimated using the Mann-Whitney U test. The frequency (%) of the categorical variables was used to represent them, and the chi-square test was used. The receiving operating characteristics (ROC) curve and the area under the curve (AUC) were calculated for each parameter. The predictive value of PLR for prediction of HCC was determined, with an AUC of more than 0.80 being a solid indicator. A P value of 0.05 was regarded as statistically significant.
Results
General Clinical Data of Patients
As shown in Table 1, the general clinical data of the 309 study participants admitted to Jingzhou Central Hospital from January 2021 to December 2022 were enrolled in this retrospective analysis. The mean age of HCC patients was 55.70 ± 10.77 years, and that of patients with liver cirrhosis was 58.17 ± 12.88 years Table 2. Age was statistically different between the patients with hepatocellular carcinoma and liver cirrhosis (P < 0.05). There was no statistical difference in gender between the HCC patients and the patients with liver cirrhosis (p = 0.260).
Demographic Data of Study Participants.
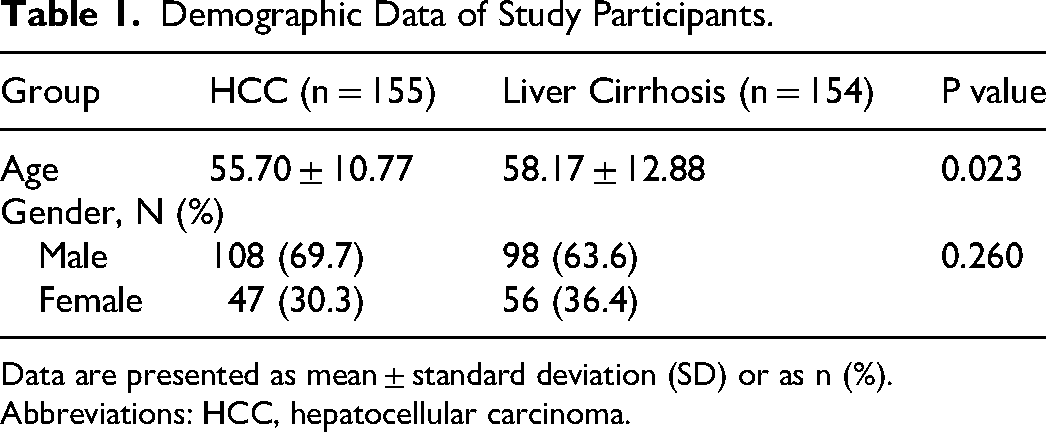
Data are presented as mean ± standard deviation (SD) or as n (%).
Abbreviations: HCC, hepatocellular carcinoma.
Hematological profiles of HCC and Liver cirrhosis patients.
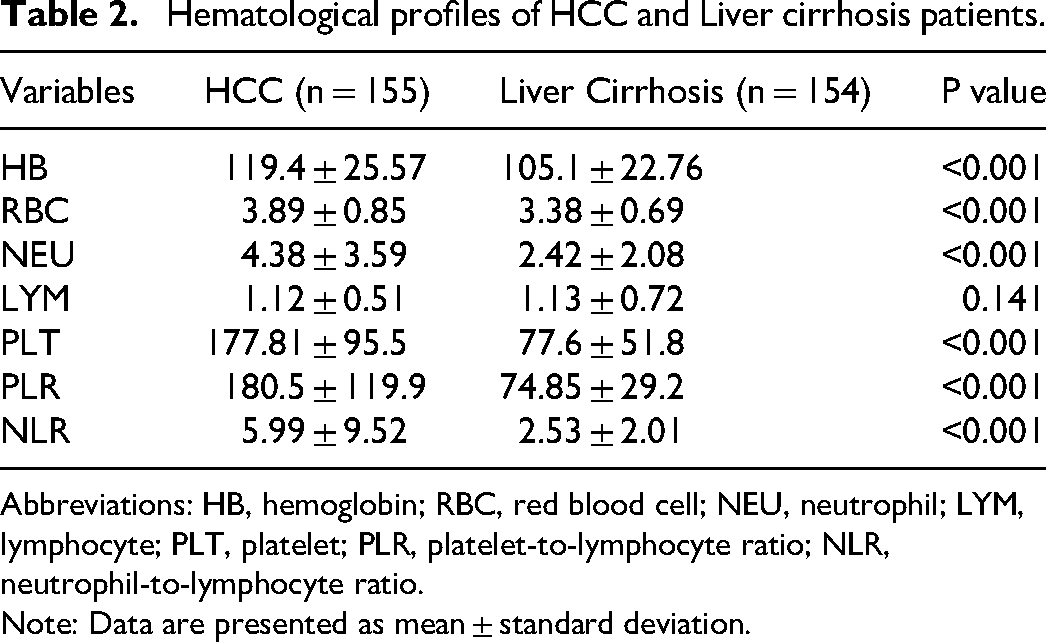
Abbreviations: HB, hemoglobin; RBC, red blood cell; NEU, neutrophil; LYM, lymphocyte; PLT, platelet; PLR, platelet-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio.
Note: Data are presented as mean ± standard deviation.
Hematological and Derived Hematological Profiles of Study Patients
Hematological and derived hematological profiles of the two study patients were analyzed. A comparison of the hematological profiles showed that HB, RBC, NEU, PLT, PLR, and NLR parameters were markedly elevated in the HCC patients (P < 0.05). Conversely, LYM was slightly decreased in the HCC patients, but there was no statistical difference between the two groups (P > 0.05).
Diagnostic Accuracy of Hematological Profiles in Predicting Hepatocellular Carcinoma Patients
The receiver-operating characteristic (ROC) curve was further used in the analysis of the hematological profiles of the patients in the prediction of hepatocellular carcinoma, and the AUC was calculated for each parameter as shown in Figure 1 and Table 3. The findings revealed that the AUC values for NEU, PLT, NLR, and PLR were 0.749, 0.867, 0.666, and 0.912, respectively, which could significantly predict HCC with high accuracies. At a cut-off of 98.7, PLR could predict HCC with a sensitivity of 81.2% and specificity of 80.6% (95% confidence interval (CI) (0.883–0.941), p < 0.001), as shown in Table 3. At a cut-off of 115 (109/L), PLT was 80.5% sensitive and 76.1 specific in predicting HCC, although NLR (AUC = 0.666, p < 0.001) and NEU (AUC = 0.749, p < 0.001) could significantly predict HCC, they had a weak performance. Although NLR had lower specificity and sensitivity, the sensitivity and specificity of PLR were still conducive in predicting hepatocellular carcinoma patients. Therefore, PLR was considered an optimal parameter for the prediction of HCC.
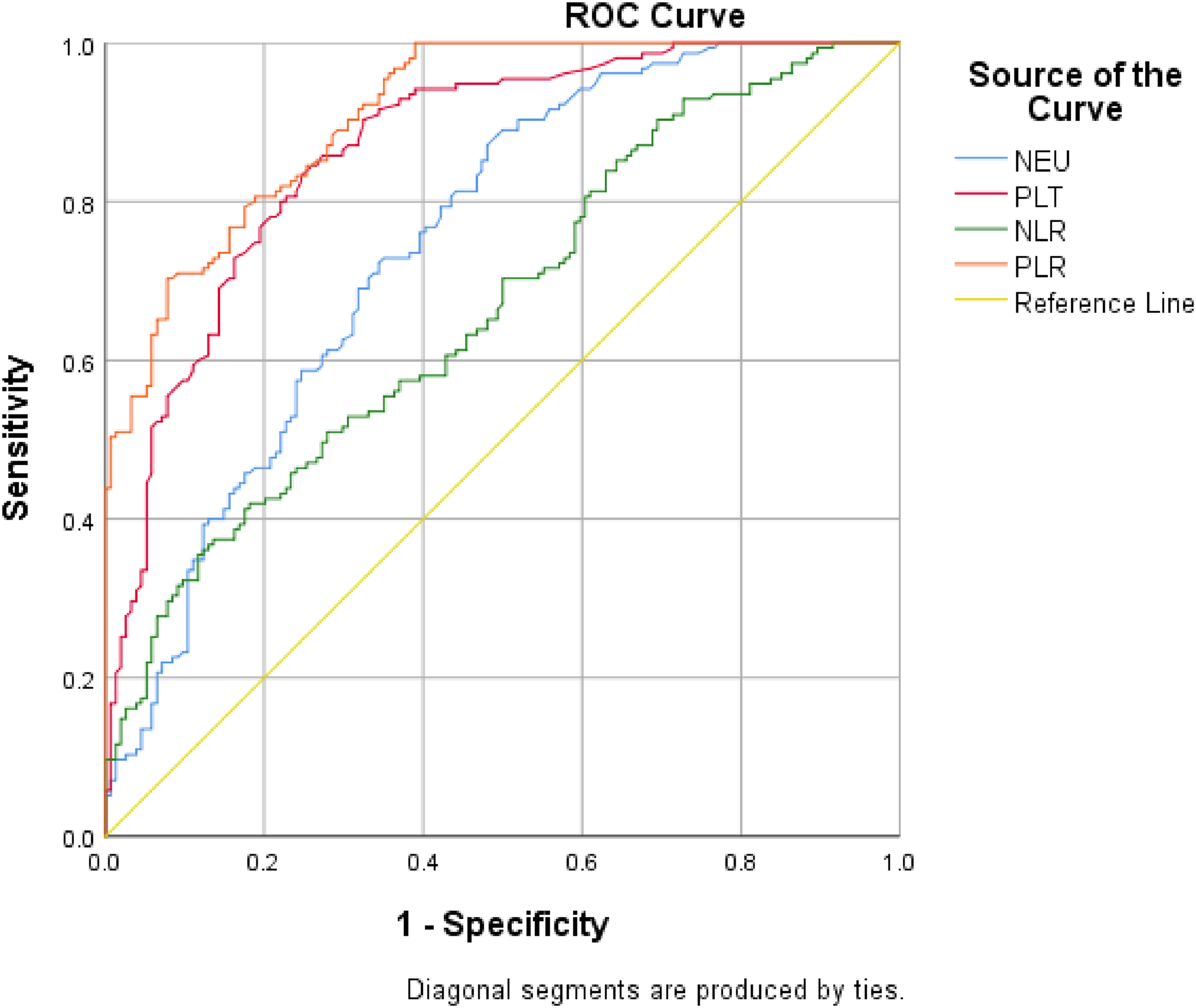
Receiver operating curve of hematological parameters in predicting hepatocellular carcinoma.
Diagnostic Accuracy of Hematological Profiles in Predicting HCC.

Abbreviation: AUC, area under the curve.
Discussion
Hepatocellular carcinoma is one of the cancers with high mortality and morbidity, and it is considered a significant threat to human health. Recently, several advanced techniques and methods, such as chemotherapy, immunotherapy, liver transplantation, surgical resection, and radiography, have been adopted to treat and manage liver cancer patients. Surgical resection and liver transplantation have been reserved for patients with early-stage liver cancer, while the other treatment options are only adopted as rescue measures in advanced cancer patients. 12 HCC is a known cancer arising out of inflammation, and approximately 80% of all cases are attributable to either hepatitis B (HBV) or hepatitis C (HCV) infections. 6 It is essential, therefore, to identify novel non-invasive biomarkers that can be used to predict HCC.
This study retrospectively analyzed the hematological and derived hematological parameters of 155 patients with hepatocellular carcinoma and 154 patients with liver cirrhosis. The AUC of the hematological and derived hematological parameters were calculated to aid in early predicting patients with hepatocellular carcinoma. The AUC of platelet-to-lymphocyte ratio was significantly higher than that of NLR, PLT, NEU, and LYM. The sensitivity (81.2%) and specificity (80.6%) of PLR were also higher than that of NLR, PLT, NEU, and LYM, which is an indication that PLR is a better marker for the prediction of early hepatocellular carcinoma. As shown in Table 3, the cut-off value of PLR is 98.7, which means when PLR < 98.7, patients are more likely to develop early HCC. A recent study suggested that PLR is a viable predictor of tumor response for hepatocellular carcinoma. 32 Other studies have demonstrated platelets’ role in facilitating tumor cell escape from the immune system. Platelet levels are known to promote proliferation in normal liver tissues and HCC; therefore, HCC patients with high platelet levels are at an increased risk of extrahepatic metastasis. 33 There is a cross-link between inflammation and tumor progression.34,35 Increased percentage of platelets secretes high levels of vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF), which are major players in angiogenesis, cell proliferation, and tumor metastasis.36–38 Platelets also provide support in tumor cell evasion of the immune system and Nieswandt et al showed platelets may protect tumor cells from lysis mediated by natural killer cells in metastasis facilitation. 39 Lymphocytes play a pivotal role in the defense mechanism of the microenvironment of HCC. Lymphocytes play a role in cell-mediated anti-tumor immune response.40–42 The lymphocyte levels are relatively low in patients with high PLR, as demonstrated in this study; however, other studies have reported that increased lymphocyte proliferation in tumors is associated with better prognosis. 43 High levels of tumor-infiltrating lymphocytes are associated with lower recurrence rate and better prognosis in HCC patients. 44 This suggests the combined effect of platelets and lymphocytes in PLR may be of predictive value in HCC patients.
Previous study has shown that PLR is a valuable biomarker in predicting outcomes in patients with HCC who underwent liver resection. 45 In addition to the traditional diagnostic techniques for HCC, many potential biomarkers have been investigated. Non-coding RNAs such as microRNAs (miRNAs) and contrast-enhanced ultrasound (CEUS) have been extensively studied as new diagnostic biomarkers. A meta-analysis evaluating the diagnostic performance of contrast-enhanced ultrasound (CEUS) in distinguishing HCC and intrahepatic cholangiocarcinoma (ICC) demonstrated that CEUS possessed high specificity and sensitivity in differentiating these two diseases. 46 MicroRNAs are potential non-invasive biomarkers as they are highly stable and can circulate freely in the blood and the saliva. A study report by Ratnasari et al showed that miRNA 29c-3p might be a potential biomarker as a tumor biomarker and a predictive factor of clinical progression and survival. 47 PLR could provide useful diagnostic value in predicting between patients with HCC and patients with liver cirrhosis. However, further prospective studies are required to confirm its usefulness in this population.
This study has a few limitations. Firstly, this is a single-center study involving a smaller number of cases. Considering the relatively minor patient population, more clinical cases are needed to confirm our findings in a future study. In addition, this was a cross-sectional rather than longitudinal design, and such methods cannot guarantee a causal relationship. Lastly, we did not analyze the prognosis of the enrolled cases. To sum up, to solve these limitations, large-sample, multi-center, and systematic prospective studies are the focus of our future study.
Conclusion
In summary, this retrospective study revealed that PLR is a better marker for predicting HCC patients from liver cirrhosis patients. This routine clinical test, PLR is easy to obtain and as such, this measurement should be considered as a biomarker in the clinical measurement of HCC. The ROC curve of these parameters analyzes further that PLR was the best predictor of HCC, with optimal specificity of 80.6%, improving the reasonable allocation of medical resources to reduce patient mortality for clinicians.
Footnotes
Acknowledgements
Wethank the staff of the Department of Laboratory Medicine, Jingzhou Central Hospital who assisted us throughout the course of the study.
Author Contributions
Abdul Fatawu Mohammed and Xu Chen were involved in manuscript drafting, and were responsible for data collection and data analysis; Chengbin Li was responsible for the research design and critical revision of the manuscript.
Data Availability
The data supporting the findings of this study are available upon request from the corresponding author. The data were not publicly available because of privacy or ethical considerations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.