
Abstract
To investigate the relationship between antithrombin (AT) activity level and prognosis in patients requiring intensive care. Patients whose AT activity was measured within 24 h of intensive care unit (ICU) admission were enrolled for analysis. The primary endpoint was mortality at discharge. Prognostic accuracy was examined using receiver operating characteristic (ROC) curves and cox hazard regression analysis. Patients were divided into 6 groups based on predicted mortality, and a χ2 independence test was performed on the prognostic value of AT activity for each predicted mortality; P < .05 was considered significant. A total of 281 cases were analyzed. AT activity was associated with mortality at discharge (AT% [interquartile range, IQR]): survivor group, 69 (56-86) versus nonsurvivor group, 56 (44-73), P = .0003). We found an increasing risk for mortality in both the lowest level of AT activity (<50%; hazard ratio [HR] 2.43, 95% confidence interval [CI] 1.20-4.89, P = .01) and the middle-low level of AT activity (≥ 50% and < 70%; HR 2.06, 95% CI 1.06-4.02, P = .03), compared with the normal AT activity level (≥ 70%). ROC curve analysis showed that the prediction accuracy of AT was an area under the curve (AUC) of 0.66 (cutoff 58%, sensitivity 61.4%, specificity 68.2%, P = .0003). AT activity was significantly prognostic in the group with 20% to 50% predicted mortality (AUC 0.74, sensitivity: 24.0%-55.5%, specificity: 83.3%-93.0%). An early decrease in AT activity level in ICU patients may be a predictor of mortality at discharge.
Background
Antithrombin (AT), an anticoagulation inhibitory factor synthesized in the liver, binds 1:1 to thrombin and factor XA and inhibits their coagulation activity. AT activity is recognized as an important blood test for the diagnosis of disseminated intravascular coagulation (DIC) syndrome and as an indicator of AT administration. 1 In DIC, AT activity decreases based on decreased synthesis, 2 increased loss, 3 and drug-induced 4 factors, in addition to increased consumption. Decreased AT activity has been reported to be associated with disease severity and prognosis, suggesting that it is a useful prognostic marker even in the absence of DIC.5–7
Patients admitted to intensive care units (ICUs) are known to have higher severity and mortality rates than those admitted to general wards. 8 Although recent updates to scoring systems using big data and machine learning techniques have improved the predictive accuracy of case groups with complex patient backgrounds, 9 the amount, type, and time course of data used daily in the ICU environment changes rapidly. This makes the routine use of highly accurate prognostic scores are not easy. 10 Simple prognostic methods using single markers or indices have been reported, but their accuracy is not high, which is problematic.11–13
Against this background, this study examines the potential of AT activity level as a predictor of prognosis in patients admitted to ICUs. Since there have been no studies that have examined the application of AT activity values to all patients admitted to the ICU, the hypothesis of this study is that AT activity values at ICU admission may be used in a simple and timely manner to predict prognosis. The purpose of this study is to analyze the prognostic accuracy of AT activity values and compare it with existing prognostic scores. It is hoped that the results will provide a new method to support decision making regarding treatment strategies and resource allocation for ICU patients. It also aims to improve the quality of care through common understanding and communication with medical staff, patients themselves, and their families.14,15
Methods
Study Design
This was a 2-center retrospective cohort study with extended follow up from ICU admission to discharge, conducted at Yamagata University Hospital and Nihonkai General Hospital. Ethics committee approval was obtained from all institutions (approval numbers, Yamagata University Hospital: 2020-312; Nihonkai General Hospital: 2020-29), and all methods were performed in accordance with the guidelines of the Declaration of Helsinki. The need for informed consent was obtained by the opt-out method, and the lead author is responsible for the completeness of the study data and the accuracy of data analysis.
The inclusion criteria were all patients admitted to the ICU of the target facility from January 2018 to December 2019. Patients whose AT activity was measured within 24 h of ICU admission were included in the statistical analysis. Exclusion criteria were death within 24 h of ICU admission at age 18 years or younger, use of AT preparations prior to measurement, pregnancy, congenital AT deficiency, human immunodeficiency virus infection or acquired immunodeficiency syndrome. 16 There was no upper age limit.
AT activity was measured using ACL TOP 750 CTS (Instrumentation Laboratory, Bedford, MA, USA) or CP3000 (Sekisui Medical Company, Tokyo, Japan). The normal values of AT activity provided by the manufacturers were 83% to 128% for ACL TOP 750 CTS and 80% to 130% for CP3000. The same instrument was used for other coagulation markers, including FDP. Arterial blood is used in cases in which observation arterial manometry is being performed, and venous blood is used in all other cases. Specimens are stored in test tubes containing 3.2% sodium citrate, and plasma components are extracted by centrifugation at 1500 rpm for 15 min and measured with the above measuring instrument. These series of measurements are performed quickly after blood collection and specimens are processed at room temperature. Measurements are based on the guidelines of the Clinical Laboratory Standards Institute. 17
The primary endpoint was mortality at discharge, and secondary endpoints were mortality at 7 and 28 days. The study complies with the guidelines for diagnostic and prognostic research (STARD and TRIPOD), but does not comply with the part of the study that separates train set, test set, and verification set.
Statistics
Continuous variables were evaluated for normality of distribution using the Kolmogorov-Smirnov test. Categorical data are presented as frequencies and percentages. Comparisons between 2 groups were made with the Mann-Whitney U test or Student's t-test for continuous variables; comparisons between 3 groups were made with the analysis of variance (ANOVA) test or Kruskal-Wallis test. Categorical variables were tested for χ2 independence, and Fisher's exact test was adapted when there were 2 or more cells with an expected value <5. Diagnostic accuracy was assessed using the area under the curve (AUC) of the receiver operating characteristic curve (ROC); the optimal cutoff value for the ROC curve was calculated using the Youden index.
We assessed the prognostic utility of AT activity levels using Cox proportional hazards regression models. Two distinct analyses were conducted: one examined the hazard ratio for each 1% increase in AT activity levels, and the other stratified patients into 3 groups based on their AT activity levels for a more granular understanding of the risk. Patients were divided into 3 groups [group H (AT activity: ≥70%), group M (AT activity: ≥50% and <70%), and group L (AT activity: < 50%)]. 18 Results are presented with hazard ratios, 95% confidence intervals, and P values. Model counts for each variable were also listed. Schoenfeld residuals test was used to verify the assumptions. The Schoenfeld residuals for each variable were plotted over time to confirm that they were independent of time. For multicollinearity, the variance expansion factor (VIF) was calculated and a VIF >10 was considered to be collinear. Model evaluation was performed using the concordance index, log likelihood, partial log likelihood, partial Akaike information criterion, and log likelihood ratio test. Additional adjustment variables were age, body mass index, organ failure assessment (SOFA) score, and presence of surgery. The number of independent variables was set so that the number of independent variables was less than the number of the lesser outcome divided by 10, with death in hospital as the primary endpoint. In our pilot study, sample size calculations based on AT activity values in the surviving and nonsurviving groups were 10 cases for survival group and 10 cases for nonsurvival group each for a 50% mortality rate and 19 cases for survival cases and 4 cases for nonsurvival cases for an 18% mortality rate. These numbers were found to be less than the former.
For preprocessing, missing data were compared with 3 groups divided by AT activity values (AT activity <50, ≥50 and <70, ≥70) and the distribution of missing data with the χ2 test; if there was no association between AT activity values and the distribution of missing values, the analysis was performed without excluding missing values in multivariate analysis. After confirming that no differences were observed between the counties, multiple assignment methods were used to supplement the data. The multiple assignment method using Bayesian theory was used to supplement the results. 19 Categorical variables were made into dummy variables of 0 and 1.
As a sensitivities analysis, analyses on a subset of the data were performed as follows. A random sample was selected from the overall dataset and the same analysis was performed on that subset. This was repeated a total of 5 times to ensure that the results were consistent.
All reported P values were 2-sided, with a P value of <.05 indicating a statistically significant difference. Statistical analysis was performed using Python (Python Software Foundation).
Results
There were 1984 patients admitted to the intensive care unit during the study period. Out of these, a total of 281 patients were included in the study, focusing on those who had their AT activity levels measured and met the inclusion criteria (Figure 1). Most of the patients were male (60.4%) and the age of eligible cases were 69 (58-77) years. The reasons for admission were postoperative cases (55.2%) and emergency admission (74.4%) (Table 1). Additional demographic details for each hospital are provided in Supplemental Table 1.

Study flow diagram of the patient selection process.
Characteristics of the Study Population.

Data are presented as the count (%), median [IQRs] or mean [SD].
The medical background and test findings of all participants, separated into survivors and nonsurvivors, are listed.
Abbreviations: Alb, albumin; APACHE, Acute Physiology and Chronic Health Evaluation; AT, antithrombin activity; BMI, body mass index; CRP, C-reactive protein; DIC, disseminated intravascular coagulation; FDP, fibrin/fibrinogen degradation products; FIO2, fraction of inspiratory oxygen; Ht, hematocrit; IQR, interquartile range; PaO2, partial pressure of arterial oxygen; Plt, platelet count; PT-INR, prothrombin time-international normalized ratio; SD, standard deviation; SOFA, Sequential Organ Failure Assessment; WBC, white blood cell.
Univariate analysis showed significant differences in AT activity levels between survivor and nonsurvivor groups for mortality after 28 days and at discharge (Table 1). The Acute Physiology And Chronic Health Evaluation II (APACHE II) score was calculated from data within 24 h of admission, and the predicted mortality rate was calculated from the APACHE II score. Age and sex did not differ between the 2 groups. FDP was the most common missing data (13.4%). The other missing data were included in a 3-group test based on AT activity values. Because of the low association between missing data and AT activity, cases with missing data were also included.
ROC curve analysis showed that the AT activity level had a prognostic value of AUC 0.66 (cutoff: 58%, sensitivity: 61.4%, specificity: 68.2%) (Figure 2). This was statistically as accurate as the APACHE II and SOFA scores (APACHE II score P = .68, SOFA score P = .18).

The ROC curves predicting inpatient mortality. The ROC curves reveal sensitivity/specificity relationships based on AT activity (A), APACHE II score (B), SOFA score (C), and acute DIC score (D), respectively. The cutoff value and P value for AT activity (A) was 58% and P = .0003, for APACHE II score (B) was 19 and P ≤ .0001, for SOFA score (C) was 8 and P ≤ .0001, for acute DIC score (D) was 2.5 and P = .0002. Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; AT, antithrombin; AUC, area under the curve; 95% CI, 95% confidence interval; DIC, disseminated intravascular coagulation; ROC, receiver operating characteristic; SOFA, sequential organ failure assessment.
The subjects were divided into 3 groups according to the AT activity values [group H (AT activity: ≥70%), group M (AT activity: ≥50% and <70%), group L (AT activity: <50%)] (Figure 3 and Supplemental Table 2). The severity of patients differed between the groups. The SOFA score increased with decreasing AT activity values among the 3 groups (Figure 3B). Furthermore, Dunn's multiple comparison test showed that group L had a significantly higher SOFA score than group H (P = .0063). Survival rates differed significantly between groups L, M, and H (Figure 3C). By Bonferroni correction, group H had significantly higher survival rates than group L (log-rank test P = .0069, Gehan-Breslow-Wilcoxon test P = .011). The findings for group M's SOFA score and survival were better than those for group L and worse than those for group H, but they were not statistically different from one another.

Distribution of AT activity levels in relation to the SOFA score and prognosis in participants. (A) Box-and-scatterplots according to their AT activity values, the subjects were split into 3 groups (groups L, M, and H). (B) The SOFA values for the 3 groups were different, with group L scoring higher than group H. (C) Kaplain-Meier curves reveal that the survival rates of the 3 groups varied, with group H showing a greater survival rate than group L. Abbreviations: AT, antithrombin; SOFA, sequential organ failure assessment.
In multivariable-adjusted Cox-proportional hazards regression models, the risk of death is 2.43 times higher in patients with group L (≤50%) and 2.06 times higher in those with group L (≥50% and <70%) (Table 2). Another multivariate analysis, which examined each disease separately, showed that there was a significant hazard risk for different levels of AT activity (Supplemental Tables 3 and 4). The analysis revealed that the L group had a higher hazard ratio compared to the H group, and a similar trend was observed in the M group. After statistical adjustment, significant differences emerged in the non-DIC and nonsurgery categories. Additionally, ROC curve analysis for the most common diseases yielded AUC values ranging from 0.520 to 0.721 (refer to Supplemental Table 5). Specifically, in cases of sepsis with DIC, the AUC was 0.72, with a cutoff value of 53.5%, a sensitivity of 60.0%, and a specificity of 73.7%.
Cox Proportional Hazard Analysis to Distinguish Mortality at Discharge.
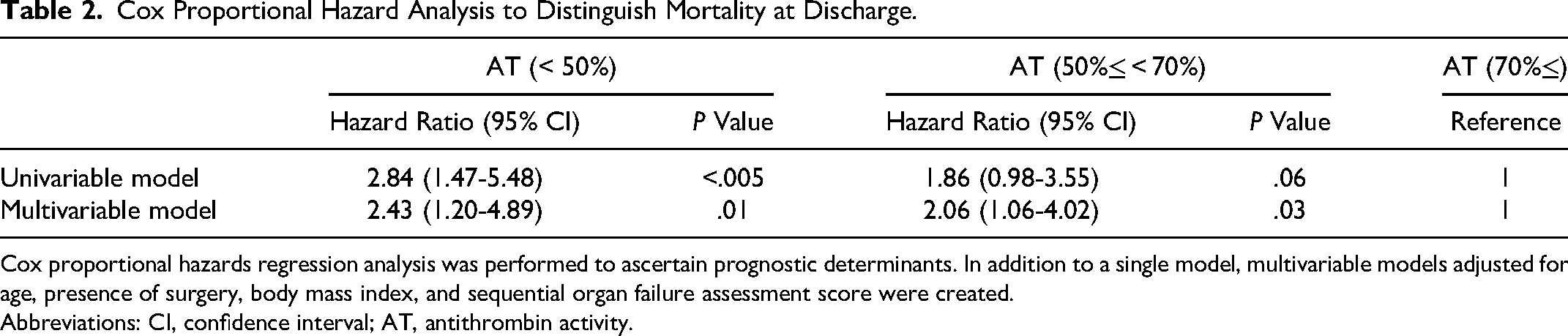
Cox proportional hazards regression analysis was performed to ascertain prognostic determinants. In addition to a single model, multivariable models adjusted for age, presence of surgery, body mass index, and sequential organ failure assessment score were created.
Abbreviations: CI, confidence interval; AT, antithrombin activity.
We stratified patients by predicted mortality and evaluated accuracy (Table 3, Supplemental Figure 1, the number of cases divided by the AT activity value [cutoff value 58%], which forecasts hospitalization mortality obtained from the APACHE II score, stratifies the predicted mortality). The χ2 test with an AT activity cutoff of 58% significantly predicted the outcome in the ≥20% and <50% predicted mortality group (AUC: 0.74, sensitivity: 24%-55.6%, specificity: 83.3%-93.0%).
Accuracy of Prognosis Using Stratified Values of AT Activity for Projected Mortality.

Based on threshold values for AT activity of 58%, for each anticipated mortality stratified using the APACHE II score, hospital mortality was investigated using a chi-square test.
Abbreviations: AT, antithrombin; APACHE, Acute Physiology and Chronic Health Evaluation.
Discussion
In our study, we found that the level of AT activity within 24 h of ICU admission serves as an independent predictor of discharge prognosis, comparable to APACHE II and SOFA scores in ROC curve analysis. The predictive accuracy varies based on the underlying disease and predicted mortality, having higher discriminatory power in cases with predicted mortality ≥20% and <50%.
Contrasting results have been reported in previous studies regarding AT's role in prognosis.
While some past research associated low AT activity with poor prognosis,20–26 others found its predictive value limited6,27–33 Our results align with the former, our subgroup analysis revealed that AT activity demonstrated a prognostic significance in line with previous findings in open cardiac operations and septic conditions,27,28 excluding illnesses with small sample sizes, such as acute pancreatitis and trauma. This observation was made with a demarcation threshold of 50% to 60% AT activity, which is consistent with prior documentation.
There are several reasons why AT activity values are prognostically useful. It may indicate increased consumption or decreased production in severe cases as an indicator of organ damage, and it may produce an anti-inflammatory response through syndecans.
In our study, the SOFA score showed the highest accuracy in the predictive model, emphasizing the grim prognosis in severe cases with multiple organ failures, consistent with prior studies. 34 AT also showed comparable predictive accuracy, as AT is a marker used in DIC diagnostic criteria, it may serve as an organ damage marker. 1 Yet, platelet count alone did not independently predict prognosis, pointing to the potential association of other SOFA score parameters with prognosis and AT activity levels (Supplemental Table 2 and Figure 2). As other coagulation factors, synthesis occurs in the liver and may reflect liver function. 35 As an overall indicator of multiorgan failure, we consider that it may reflect prognosis.
AT is not only an anticoagulant but also binds to syndecans and provides vascular-endothelium protection, 36 myocardial protection,37,38 and renoprotection. 33 Therefore, low AT activity levels may lead to organ damage that progresses over time and a poor prognosis. The anti-inflammatory activity of AT is mediated directly via syndecans and indirectly via the coagulation pathway. 39 Syndecans are transmembrane proteoglycans that play a major role in inflammation by regulating leukocyte extravasation and cytokine function. 40 In addition, syndecan is a major source of cell surface heparan sulfate and regulates inflammatory cell maturation, leukocyte-endothelial interactions, and chemotaxis. 41 The coagulation pathway is also involved in inflammation, and excessive fibrin deposition in the lung is a prominent feature of lung injury. 42
The development of intensive care has led to declining mortality rates.43–45 For our study group, predicted mortality for the entire subject population was 26.2%, with actual mortality rates of 6.0% for 7-day mortality, 13.8% for 28-day mortality and 22.1% for mortality at discharge. This is comparable to the discharge mortality rate of 13.2% to 52.3% for patients admitted to the ICU.10,46–48
However, long-term prognosis, dictated by the late phase transition, remains a challenge. 49 Our analysis showed that the group with predicted mortality of 20% to 50% had significant discriminative power. This suggests that even patients with mild-to-moderate declines in AT activity, below normal, are more likely to be discharged alive. Our study also allowed us to identify the patient group for whom AT is likely to be prognostic. The association between AT activity level and prognosis was found to be low in mild cases and very severe cases.
The reason for the lack of significant difference in AT activity between survivors and nonsurvivors in cases with predicted mortality of 50% or higher, is likely due to the high proportion of severe cases in this group, particularly among those who died within 2 days of admission. The time of lowest AT activity value may vary depending on the pathological condition and time course. 31
Looking at specific diseases, the AUC was lower in patients with DIC, with a ROCAUC of 0.52. However, considering only septic DIC cases, the AUC demonstrated moderate accuracy with a ROCAUC of 0.72. The implications of assessing AT activity levels per predicted mortality may have important implications for AT use. In the KyberSept trial, 50 improved survival was observed in patients treated with AT, excluding patients with predicted mortality of 60% or greater. Another RCT using AT agents found no significant difference in mortality for septic DIC with AT activity levels of 50% to 80%. 51
In sepsis, 4 phenotypes correlating with host response patterns and clinical outcome have been noted. 52 This suggests that AT preparations may be most effective when selectively administered to patients for whom reduced AT activity levels are associated with prognosis. In our study, an AT activity level of approximately 50 in sepsis was a useful cutoff value for prognosis, and prognosis was useful in cases with a predicted mortality rate of 20% to 50%. Therefore, we can infer that the benefit of AT therapy is relatively small in the groups with particularly high or low severity of illness and relatively high AT activity, since the AT activity value has little impact on prognosis.
The strengths of this study include the high variety of the patients, as it examines all admissions from multiple institutions, the sufficient sample size for multivariate analysis and the short 2-year time period covered.
There are 6 limitations of the study: first, because it is a retrospective observational study, the reason for testing AT activity levels may vary from one physician to another; measurement of AT activity levels is likely to be for diseases such as sepsis or macrovascular disease, which can cause abnormalities in the coagulation-fibrinolytic system. It is also possible that protocols for measuring coagulation time and treatment follow up varied from case to case, which may have also influenced the results. Second, while our sample size was statistically robust, it featured a skewed distribution due to the small number of participating facilities and their overwhelming representation of postoperative surgical cases in the ICU. Even though we evaluated the accuracy for both surgical and nonsurgical cases separately, it is essential to interpret our findings within the context of the specific characteristics of these facilities. Third, FDP was the most common missing data (13.4%). We performed a test including other missing data, dividing the patients into 3 groups according to AT activity values. The fourth limitation was the use of fresh frozen plasma (FFP) products: cases of AT agents use were excluded, but FFP products were not excluded from the administration. The more frequent use of FFP during open heart surgery may have led to increase AT activity levels. On the other hand, unfractionated heparin is used intraoperatively during open heart surgery. Unfractionated heparin binds tightly to AT and exerts anticoagulant effects. Fifth, the treatment and medical histories before ICU admission were not recorded. In sepsis, for example, the AT activity level may be modified because blood samples are collected differently in the early stage of the disease, when the inflammatory response has not yet increased, compared to the middle stage, when the inflammatory response is high. In addition, transfusions and invasive procedures in the emergency room or surgical department may result in different AT activity levels. Lastly, the sixth limitation involves the different instruments used to measure AT activity values. However, previous studies have reported minimal discrepancies between the ACL TOP 750 and CP3000 models used in this study, suggesting a negligible effect on the results. 53
Conclusions
In an analysis of cases in which AT activity values were measured within 24 h of ICU admission, AT activity values were an independent prognostic predictor of mortality at discharge. When examined for accuracy, AT activity showed higher specificity and predicted survival at discharge in the group of cases with a predicted mortality of ≥20% and <50%.
Supplemental Material
sj-docx-1-cat-10.1177_10760296231218711 - Supplemental material for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study
Supplemental material, sj-docx-1-cat-10.1177_10760296231218711 for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study by Kenya Yarimizu, Masaki Nakane, Yu Onodera, Taro Matsuuchi, Hiroto Suzuki, Masatomo Yoshioka, Masaya Kudo and Kaneyuki Kawamae in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-2-cat-10.1177_10760296231218711 - Supplemental material for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study
Supplemental material, sj-docx-2-cat-10.1177_10760296231218711 for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study by Kenya Yarimizu, Masaki Nakane, Yu Onodera, Taro Matsuuchi, Hiroto Suzuki, Masatomo Yoshioka, Masaya Kudo and Kaneyuki Kawamae in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-3-cat-10.1177_10760296231218711 - Supplemental material for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study
Supplemental material, sj-docx-3-cat-10.1177_10760296231218711 for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study by Kenya Yarimizu, Masaki Nakane, Yu Onodera, Taro Matsuuchi, Hiroto Suzuki, Masatomo Yoshioka, Masaya Kudo and Kaneyuki Kawamae in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-4-cat-10.1177_10760296231218711 - Supplemental material for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study
Supplemental material, sj-docx-4-cat-10.1177_10760296231218711 for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study by Kenya Yarimizu, Masaki Nakane, Yu Onodera, Taro Matsuuchi, Hiroto Suzuki, Masatomo Yoshioka, Masaya Kudo and Kaneyuki Kawamae in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-5-cat-10.1177_10760296231218711 - Supplemental material for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study
Supplemental material, sj-docx-5-cat-10.1177_10760296231218711 for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study by Kenya Yarimizu, Masaki Nakane, Yu Onodera, Taro Matsuuchi, Hiroto Suzuki, Masatomo Yoshioka, Masaya Kudo and Kaneyuki Kawamae in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-jpg-6-cat-10.1177_10760296231218711 - Supplemental material for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study
Supplemental material, sj-jpg-6-cat-10.1177_10760296231218711 for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study by Kenya Yarimizu, Masaki Nakane, Yu Onodera, Taro Matsuuchi, Hiroto Suzuki, Masatomo Yoshioka, Masaya Kudo and Kaneyuki Kawamae in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-jpg-7-cat-10.1177_10760296231218711 - Supplemental material for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study
Supplemental material, sj-jpg-7-cat-10.1177_10760296231218711 for Prognostic Value of Antithrombin Activity Levels in the Early Phase of Intensive Care: A 2-Center Retrospective Cohort Study by Kenya Yarimizu, Masaki Nakane, Yu Onodera, Taro Matsuuchi, Hiroto Suzuki, Masatomo Yoshioka, Masaya Kudo and Kaneyuki Kawamae in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The authors wish to thank research assistants of Department of Anesthesiology, Yamagata University Medical School Hospital, and acknowledge the ICU staff and colleague anesthesiologists. The most important thanks I would like to express is to my family for their emotional support.
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by KY. The first draft of the manuscript was written by KY and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
All methods were carried out in accordance with the guidelines of the Declaration of Helsinki. The need for informed consent was obtained with an opt-out method.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Yamagata University, 2020-312; Nihonkai General Hospital, 2020-29. Ethics committee approval was obtained at our institution.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
List of Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.