
Abstract
A new scoring system termed sepsis-induced coagulopathy (SIC) has been proposed to diagnose early sepsis-induced disseminated intravascular coagulation (DIC). This study performed DIC-related analyses in patients with confirmed SIC. Data from the intensive care unit (ICU) departments of the three hospitals between 2020 and 2022 were retrospectively analyzed. Finally, 125 patients with confirmed SIC were enrolled in the study. The diagnostic value of three widely used DIC criteria was assessed in patients with newly diagnosed SIC. In addition, the diagnostic and prognostic value of antithrombin (AT) was analyzed in patients with SIC. The Japanese Association for Acute Medicine DIC criteria (JAAM) exhibited the highest DIC diagnostic rate, while the mortality risk of SIC patients demonstrated a proportional increase with higher International Society on Thrombosis and Haemostasis (ISTH) and Chinese DIC scoring system (CDSS) scores. Low AT activity (<70%) in septic patients upon SIC diagnosis predicted a very high 28-day mortality rate, almost twice as high as in the normal AT activity (≥70%) group. A decreasing tendency in AT activity after clinical interventions was correlated with increased mortality. The area under the ROC curve (AU-ROC) of AT in DIC diagnosis was statistically significant when CDSS and ISTH were used as diagnostic criteria, but not JAAM. Each of the three DIC diagnostic criteria showed diagnostic and prognostic advantages for SIC. AT could be an independent prognostic indicator for SIC but demonstrated a relatively limited DIC diagnostic value. Adding AT to the SIC scoring system may increase its prognostic power.
Keywords
Introduction
Disseminated intravascular coagulation (DIC) is thought to be an abbreviation for death is coming.1,2 DIC induced by sepsis is particularly threatening as severe coagulation disorders are often associated with severe multiple organ failure.3,4 Unlike DIC induced by acute promyelocytic leukemia (APL) or pathological obstetrics, treatment of the primary disease can achieve remarkable remission of DIC. 5 Delayed diagnosis and intervention can be highly detrimental to DIC patients; however, the absence of established standard treatment for sepsis-induced DIC may lead to confusion in clinical practice, especially with regard to anticoagulant application. Recently the International Society on Thrombosis and Haemostasis (ISTH) has proposed a new category termed sepsis-induced coagulopathy (SIC) to facilitate prompt diagnosis of DIC in critically ill septic patients.6,7 The usefulness of the SIC criteria has been validated in previous studies.8,9 The SIC criteria enable the early identification of coagulation disorders in sepsis patients and guide the optimal timing for the administration of anticoagulants. 10 To date, no gold standard for DIC diagnosis has been established. A good DIC criterion should be capable of early diagnosis and predicting prognosis. Therefore, our study aimed to compare the diagnostic accuracy and predictive value for mortality between three different DIC criteria among SIC patients, including the ISTH overt DIC criteria (ISTH) 11 commonly used internationally, the Japanese Association for Acute Medicine (JAAM) 12 DIC criteria widely used in Japan, and the Chinese DIC scoring system (CDSS) 13 commonly used in China.
Modern medicine has revealed the pathophysiology of septic DIC. New laboratory parameters independent of conventional coagulation tests, such as plasminogen activator inhibitor-1(PAI-1), have attracted widespread attention and have been evaluated in some medical centers. 14 However, most of them are costly and are not routinely performed in most Chinese hospitals. Antithrombin (AT) is one of the most important physiological anticoagulants, which inhibits intrinsic (factor XIa), extrinsic (factor VIIa), and common coagulation pathways (factor Xa, thrombin). 15 In addition, AT is routinely tested in most Chinese hospitals; therefore, it is a suitable candidate for establishing treatment guidelines. A reduction in antithrombin levels is associated with disease severity in sepsis-induced DIC.16,17 Therefore, this study also assessed the diagnostic and prognostic value of AT in SIC patients.
Patients and Methods
Patients in the Study
This three-center retrospective study collected data from Intensive Care Unit (ICU) inpatients diagnosed with sepsis in West China Hospital, Sichuan Provincial People's Hospital, and Ninth People's Hospital of Shanghai Jiao Tong University between May 2020 and October 2022. The longest follow-up time was two months after discharge from the ICU. Clinical and laboratory data were collected from patients with sepsis who had confirmed SIC (SIC score ≥4) for further analysis. The three centers used only low-molecular-weight heparin (LMWH) for anticoagulant therapy. None of the patients was treated with antithrombin.
The exclusion criteria were: patients less than 14 years of age; severe underlying liver lesions (Child-Pugh B or above); patients receiving long-term anticoagulation treatment before confirmed SIC; hospitalization time in ICU less than 24 h; chronic hemorrhagic diseases such as hemophilia, idiopathic thrombocytopenic purpura, thrombotic thrombocytopenic purpura, and antiphospholipid syndrome.
Ultimately, 125 patients met the inclusion criteria and were included in the study.
All patients and donors provided written informed consent for data collection before recruitment. The present study was approved by the Ethics Committees of West China Hospital, Sichuan Provincial People's Hospital, and Ninth People's Hospital of Shanghai Jiao Tong University. The study was conducted in accordance with the provisions of the Declaration of Helsinki and local laws.
Diagnostic Criteria and Laboratory Measurements
Three different DIC scoring algorithms were used: the International Society of Thrombosis and Hemostasis criteria (ISTH; DIC diagnosis score ≥ 5), the Japanese Association for Acute Medicine DIC criteria (JAAM; DIC diagnosis score ≥ 4), and the new Chinese DIC scoring system (CDSS; DIC diagnosis score ≥7). The Modified Sequential Organ Failure Assessment (SOFA) score is an important part of the SIC scoring algorithm, which is determined by the sum of four items (respiratory SOFA, cardiovascular SOFA, hepatic SOFA, and renal SOFA). (Table 1)
DIC and SIC Scoring Algorithms.
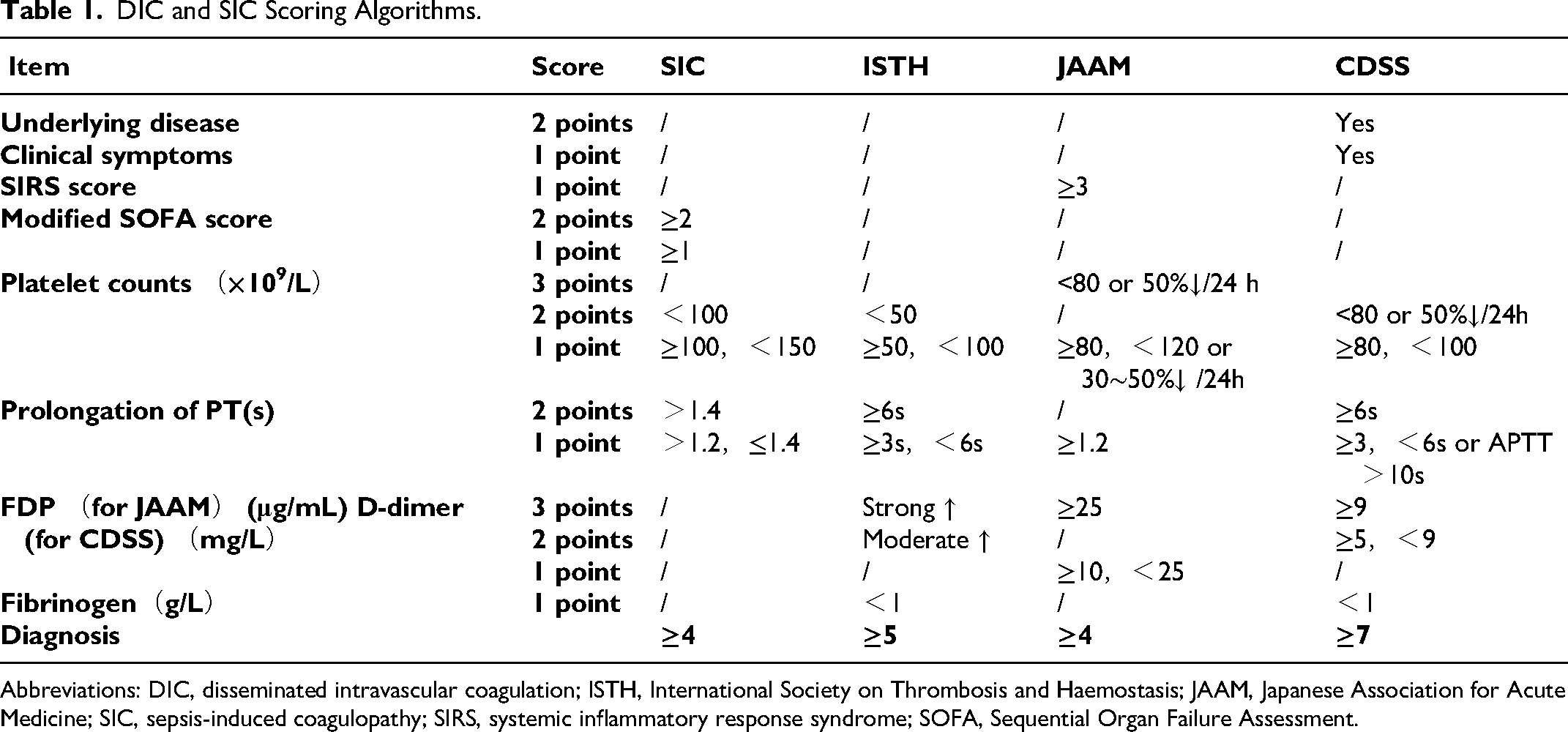
Abbreviations: DIC, disseminated intravascular coagulation; ISTH, International Society on Thrombosis and Haemostasis; JAAM, Japanese Association for Acute Medicine; SIC, sepsis-induced coagulopathy; SIRS, systemic inflammatory response syndrome; SOFA, Sequential Organ Failure Assessment.
The clinical and laboratory data of patients with sepsis satisfying the SIC criteria (score ≥ 4) were recorded for further analyses. Meanwhile, DIC scores were calculated at the time of SIC diagnosis.
Routine blood examinations, including white blood cell counts (WBC), hemoglobin content (HB), and platelet count (PLT), were determined using an XN-20A1 analyzer (Sysmex). Coagulation indicators, including D-dimer, fibrin/fibrinogen degradation products (FDP), prothrombin time (PT), activated partial thromboplastin time (APTT), antithrombin (AT), and fibrinogen (FIG), were tested using a Sysmex CS-5100 analyzer (Sysmex).
Statistical Analysis
The chi-square test was applied to compare the diagnostic efficacy of the three different DIC scoring algorithms for SIC patients.
Moreover, univariate and multivariate analyses were conducted to explore the relationship between clinical/laboratory indicators and prognosis. For univariate analysis, continuous variables with normal distribution were expressed as mean ± standard deviation (mean ± S.D), and variables with skewed distribution were expressed as median and interquartile range. The independent-sample T-test/ unpaired Wilcoxon signed-rank test (for continuous variables) and the chi-square test (for categorical variables) were used to compare the differences between the survival and non-survival groups. Stepwise logistic regression models with forward elimination were generated for the multivariate analysis. The results were reported as odds ratios (ORs) and 95% confidence intervals (CIs) in the forest plots.
Kaplan-Meier analysis was used to estimate the odds ratio (OR, 95%CI) of mortality between the normal and low AT groups. The differences were examined using the log-rank test. As AT was not included in the above-mentioned scoring algorithms, the cutoff value of AT activity was determined according to the Japanese Society on Thrombosis and Hemostasis (JSTH) DIC diagnostic criteria, 18 which is 70%.
Most deaths showed remarkably decreased AT activity after the clinical interventions. In these cases, AT activities were separately recorded at the end of the events (before and on the day of death or the day of ICU discharge) and were labeled as AT-ending. AT activities recorded at the time of confirmed SIC were labeled as AT-diagnosis. The paired-sample T-Test was used for comparisons between the non-survival and survival groups.
Furthermore, the area under the curve of receiver operating characteristic (AU-ROC) was used to evaluate the sensitivity and specificity of AT for DIC diagnosis. The above-mentioned DIC criteria were used as DIC diagnostic standards respectively. The optimal cutoff value of AT for DIC diagnosis was evaluated by the Youden index.
For all reported results, P < 0.05 was considered to denote statistical significance. The aforementioned analyses were performed using SPSS 22.0.
Results
The general information is described in Table 2. In this study, 125 cases of septic ICU inpatients were diagnosed with SIC (SIC scores were above 4 points), exhibiting a mortality of 51.2%. The median age was 67 years, and 68 (54.4%) patients were male. Regarding illness severity, all SIC patients developed organ dysfunction with varying degrees of severity, regardless of the primary disease. 67 patients (53.6%) experienced shock or microcirculatory disorders. A total of 55 patients (44.0%) had new bleeding symptoms independent of the original disease. Gastrointestinal bleeding had the highest frequency (27 patients, 21.6%). The median modified SOFA and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were 6 and 22, respectively. The values for the scoring systems and laboratory indicators are listed in Table 2. LMWH was administered as anticoagulant therapy in 73 patients (58.4%).
The Univariate Analyses of Variables Between Survivor and Non-Survivor Group.
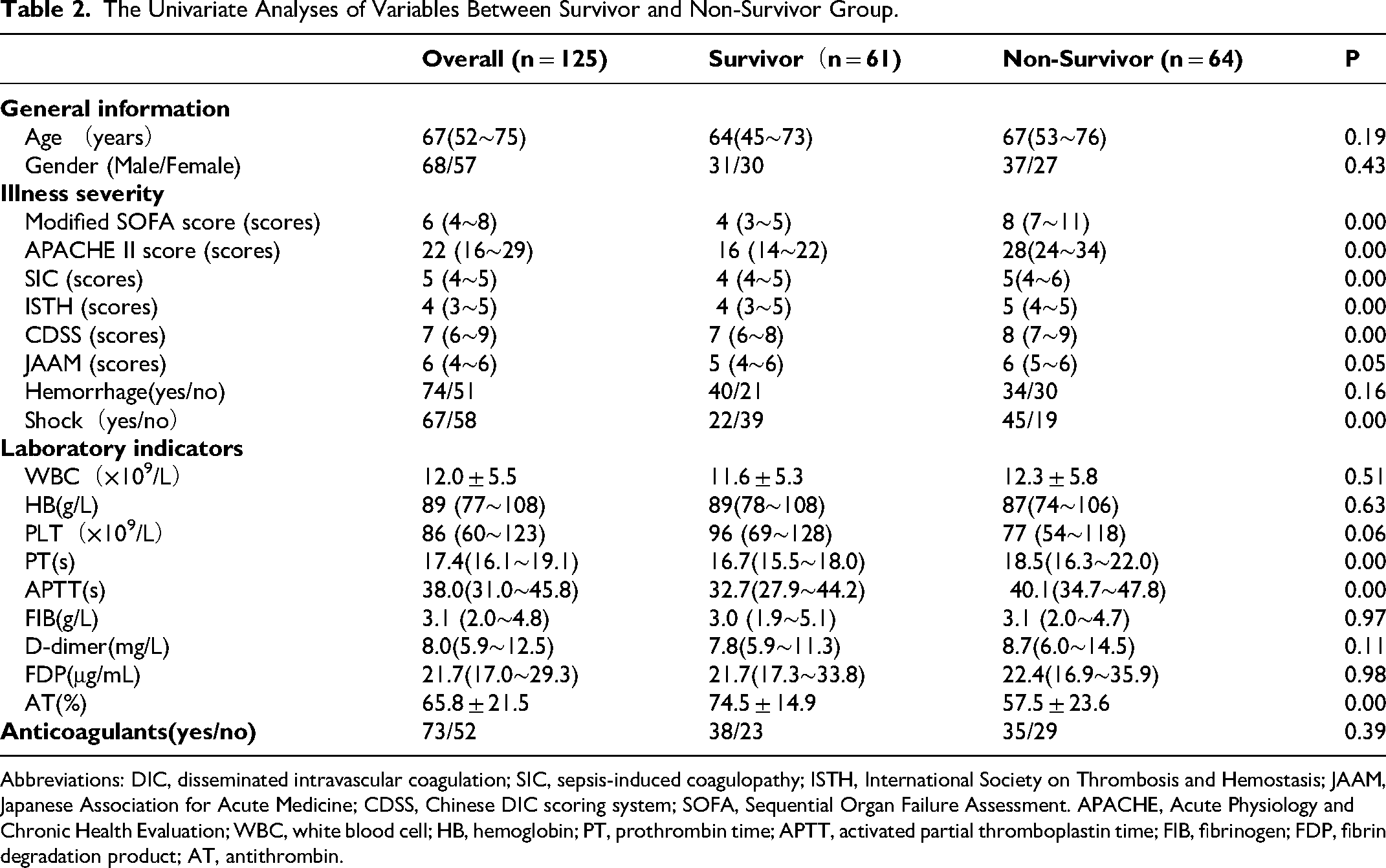
Abbreviations: DIC, disseminated intravascular coagulation; SIC, sepsis-induced coagulopathy; ISTH, International Society on Thrombosis and Hemostasis; JAAM, Japanese Association for Acute Medicine; CDSS, Chinese DIC scoring system; SOFA, Sequential Organ Failure Assessment. APACHE, Acute Physiology and Chronic Health Evaluation; WBC, white blood cell; HB, hemoglobin; PT, prothrombin time; APTT, activated partial thromboplastin time; FIB, fibrinogen; FDP, fibrin degradation product; AT, antithrombin.
The three DIC scoring algorithms were compared in patients with SIC. As shown in Figure 1, among the 125 confirmed SIC patients, 54 cases (43.2%) met the ISTH criteria for overt DIC, 92 cases (73.6%) met the CDSS-DIC criteria, and 110 (88.0%) cases met the JAAM-DIC criteria. The paired comparison revealed statistically significant differences (ISTH vs JAAM, P = 0.00; ISTH vs CDSS, P = 0.00; CDSS vs JAAM, P = 0.01). Among the subgroup of 61 survivors, 19 cases (31.1%) met the ISTH criteria for overt DIC, 36 cases (59.0%) met the CDSS-DIC criteria, and 53 (86.9%) cases met the JAAM-DIC criteria. Significant differences were determined by paired comparisons (ISTH vs JAAM, P 0.00; ISTH vs CDSS, P 0.00; CDSS vs JAAM P 0.00). Among the subgroup of 64 non-survivors, 35 cases (54.7%) met the ISTH criteria for overt DIC, 56 cases (87.5%) met the CDSS-DIC criteria, and 57 (89.1%) cases met the JAAM-DIC criteria. Except for the comparison between CDSS and JAAM, significant differences were observed by paired comparison (ISTH vs JAAM, P = 0.00; ISTH vs CDSS, P = 0.00; CDSS vs JAAM P = 0.83).
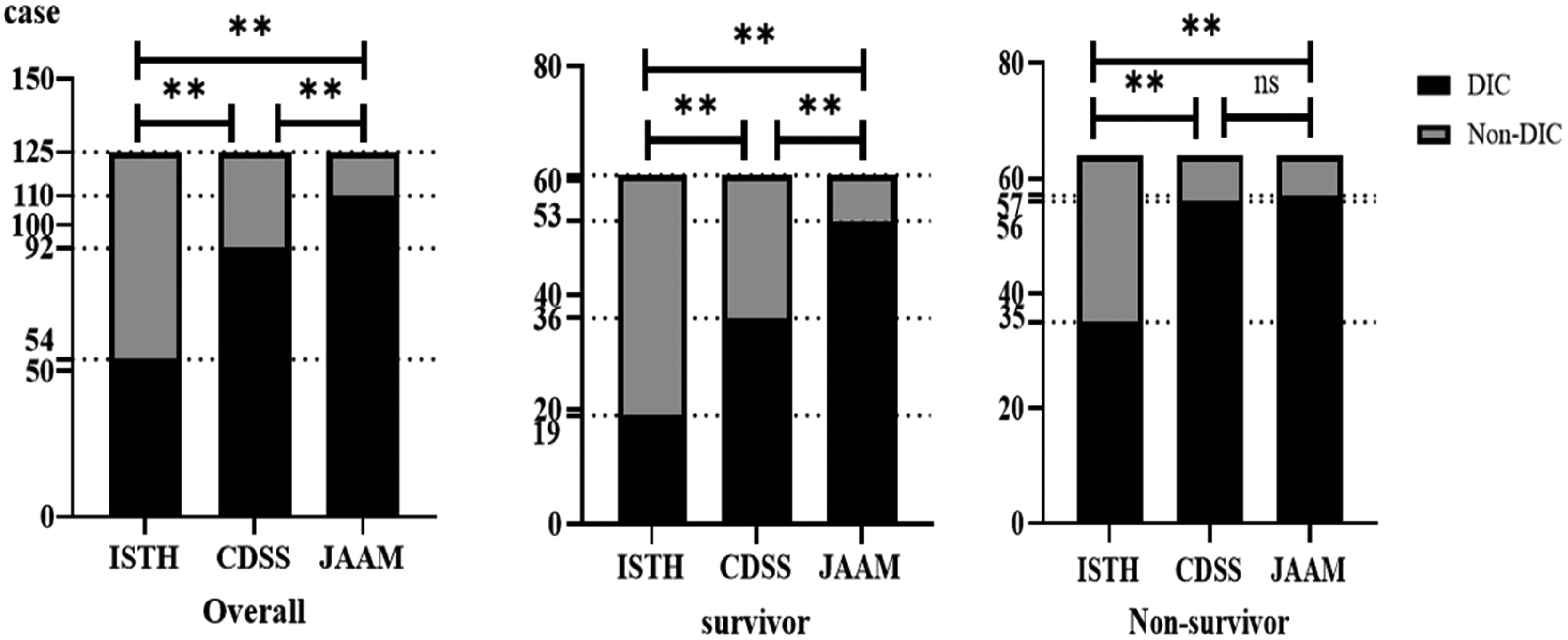
Diagnostic consistency between ISTH/CDSS/JAAM with SIC. Abbreviations: DIC, disseminated intravascular coagulation; SIC, sepsis-induced coagulopathy; ISTH, International Society on Thrombosis and Hemostasis; JAAM, Japanese Association for Acute Medicine; CDSS, Chinese DIC scoring system.
The univariate analyses of prognosis are shown in Table 2. The following indicators showed statistically significant differences between the survival and non-survival groups: modified SOFA score (median 4 vs8, P 0.00), APACHE II score (median 16 vs28, P 0.00); SIC score (median 4 vs5, P 0.00), ISTH score (median 4 vs5, P 0.00), CDSS score (median 7 vs8, P 0.00), clinical manifestations of shock (incidence rate 36.1% vs 70.3%, P 0.02), prolongation of PT (median 16.7 s vs18.5 s, P 0.00), APTT(median 32.7 s vs40.1 s, P 0.00), and AT (mean 74.5% vs57.5%, P 0.00).
Age, sex, clinical manifestations, laboratory indicators, SIC/DIC scores calculated by each scoring system, and anticoagulant therapy were included in the multivariate analysis. As shown in Figure 2, the following indicators might have an impact on mortality: occurrence of shock (OR = 3.40, 95% [ CI]: 1.15–10.09, P = 0.03), ISTH DIC scores (OR 3.57, 95% [CI]: 1.14–11.73, P = 0.03), CDSS DIC scores (OR 3.73, 95% [ CI]: 1.31–10.59, P 0.01), value of PT (s, OR 1.75, 95% [ CI]: 1.19–2.65, P 0.00), and value of AT (%, OR 0.95, 95% [ CI]: 0.92–0.98, P = 0.00).
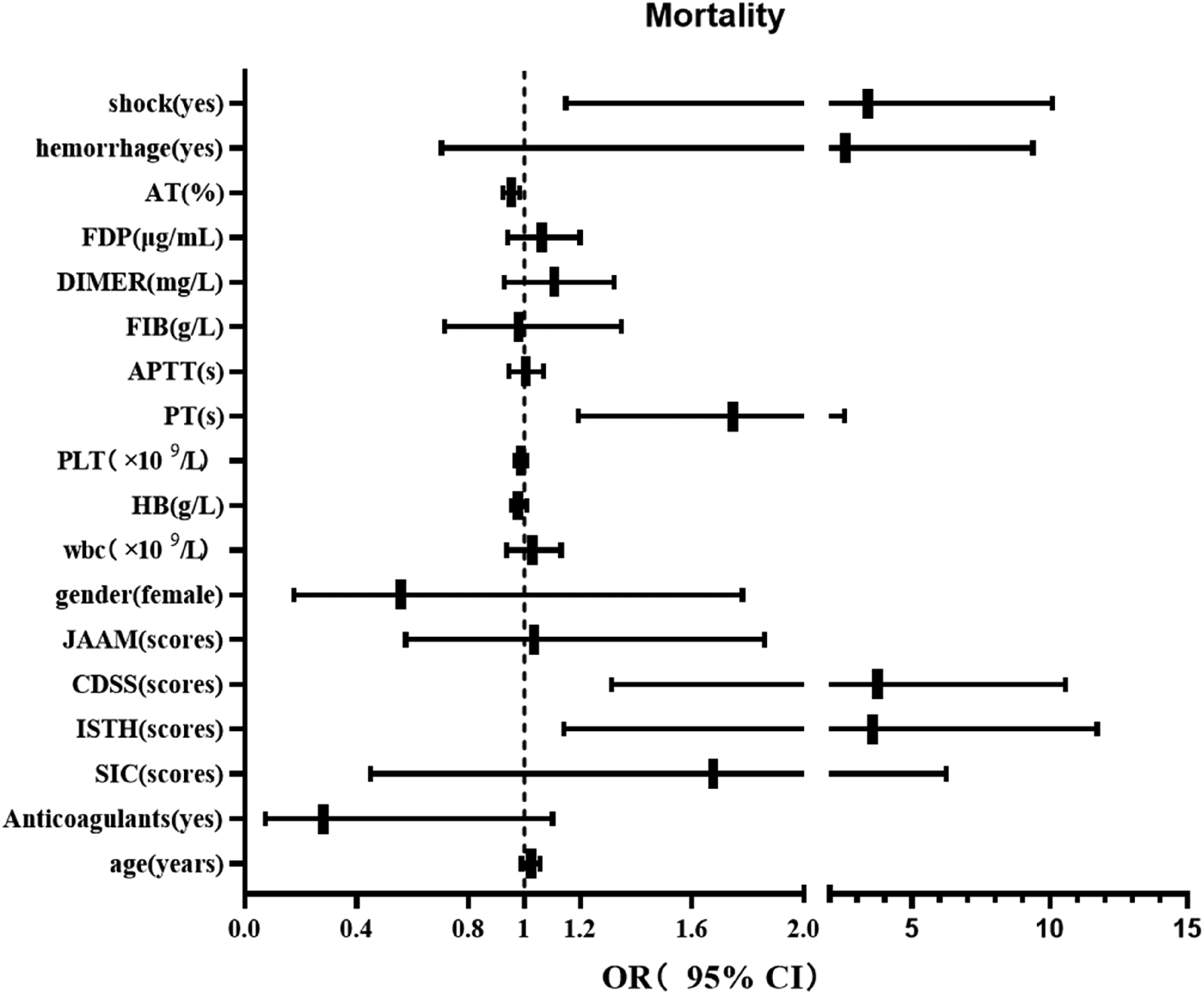
Multivariate analysis, logistic regression analysis of variables with mortality. Abbreviations: SIC, sepsis-induced coagulopathy; ISTH, International Society on Thrombosis and Haemostasis; JAAM, Japanese Association for Acute Medicine; CDSS, Chinese DIC scoring system; WBC, white blood cell; HB, hemoglobin PT, prothrombin time; APTT, activated partial thromboplastin time; FIB, fibrinogen; FDP, fibrin degradation product; AT, antithrombin; OR, Odds Ratio; CI, confidence interval.
As shown in Figure 3, Kaplan-Meier analysis suggested that the low AT activity group (below 70%) might be related to higher mortality compared to the normal AT activity group in patients with confirmed SIC (OR 2.31, 95% [CI] 1.41∼3.77, P 0.00). Moreover, the Kaplan-Meier survival curve showed that the 28-day mortality of the normal AT activity group and the low AT activity group were 32.7% and 61.4%, respectively. In addition, the results of the paired-sample T-Test showed a decreasing trend in AT activity during ICU stays in the non-survival group comparing AT-diagnosis against AT-ending, as shown in Figure 4.
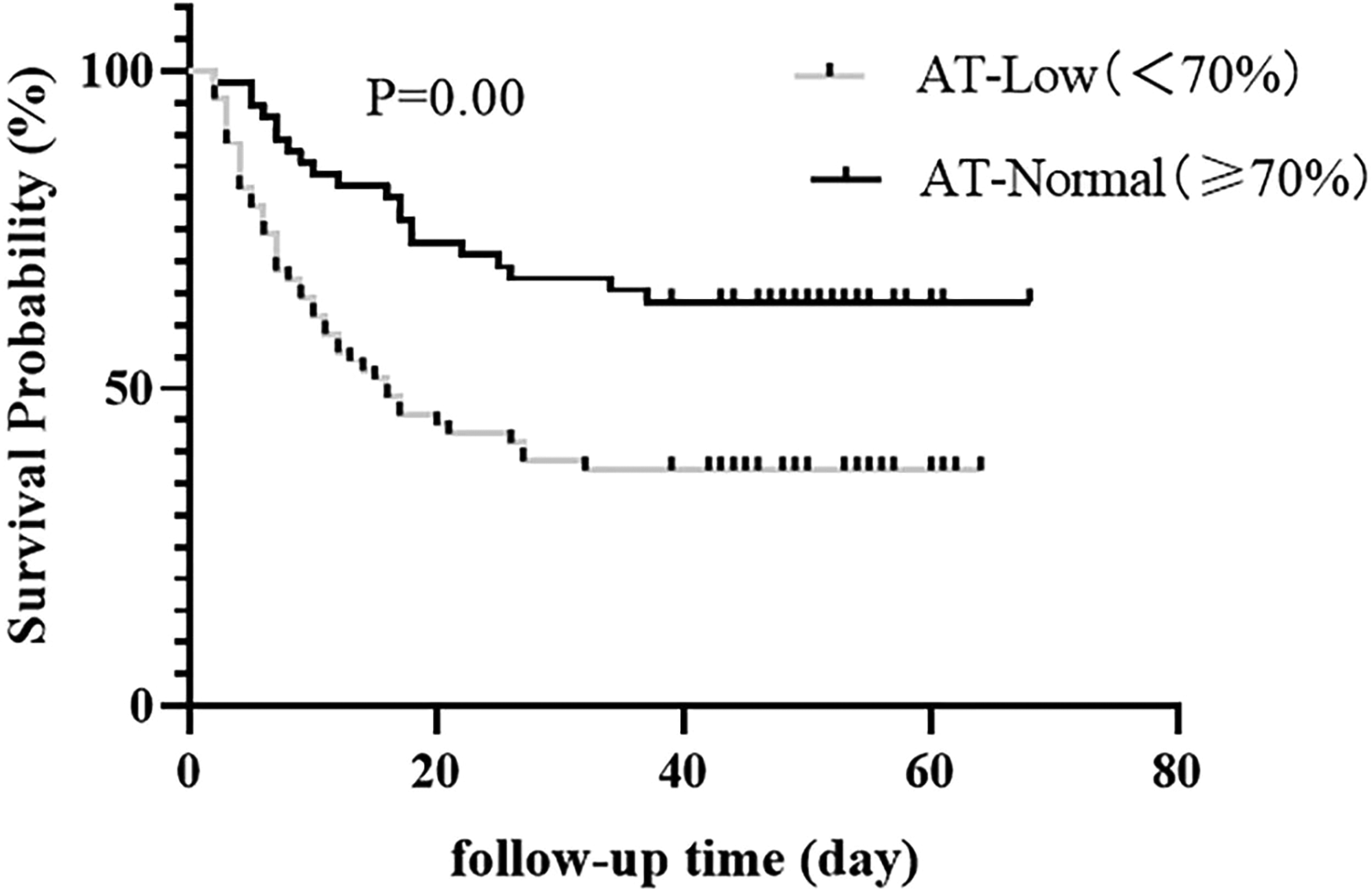
The impact of the AT level on survival probability. Kaplan-Meier curves were calculated to compare the survival probability between the AT-Low and AT- Normal group.
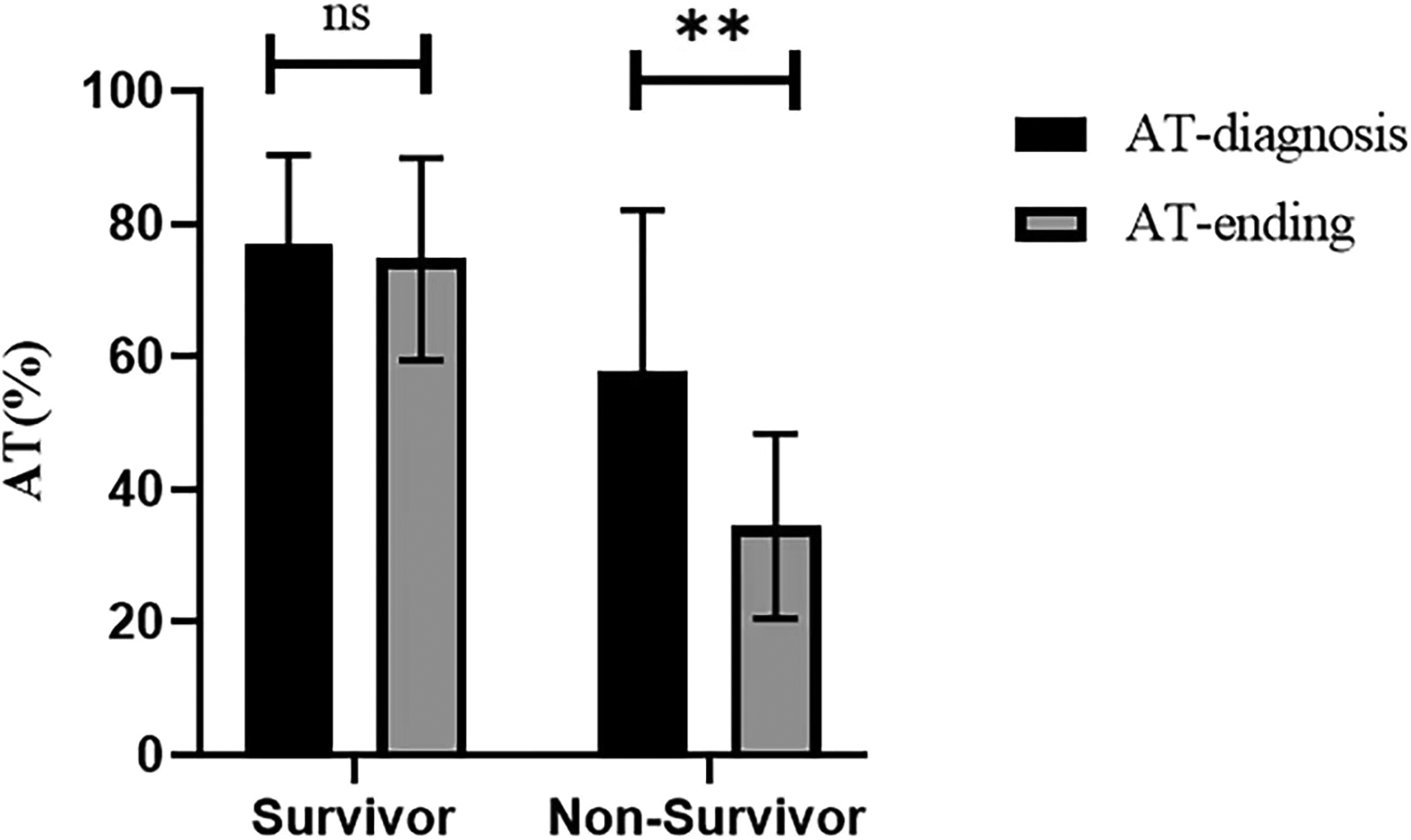
Paired-Samples T test of the changing trend in AT activities during ICU stays.
The AUC-ROC of AT in DIC diagnosis was 0.62 when using ISTH as diagnostic criterion (P 0.03, 95% [ CI], 0.52–0.72). The optimal cutoff value for AT was 62.70%, and the sensitivity and specificity were 73.2% and 53.7%, respectively. The AUC-ROC of AT in DIC diagnosis was 0.68 when using CDSS as the diagnostic criterion (P 0.01, 95% [ CI], 0.58–0.78). The optimal cutoff value for AT was 67.25%, and the sensitivity and specificity were 81.8% and 56.5%, respectively. In contrast, the AUC-ROC of AT in DIC diagnosis was 0.57 when using JAAM as the diagnostic criterion (P 0.08, 95% [CI], 0.41–0.73), which did not reach statistical significance. The results are shown in Figure 5.
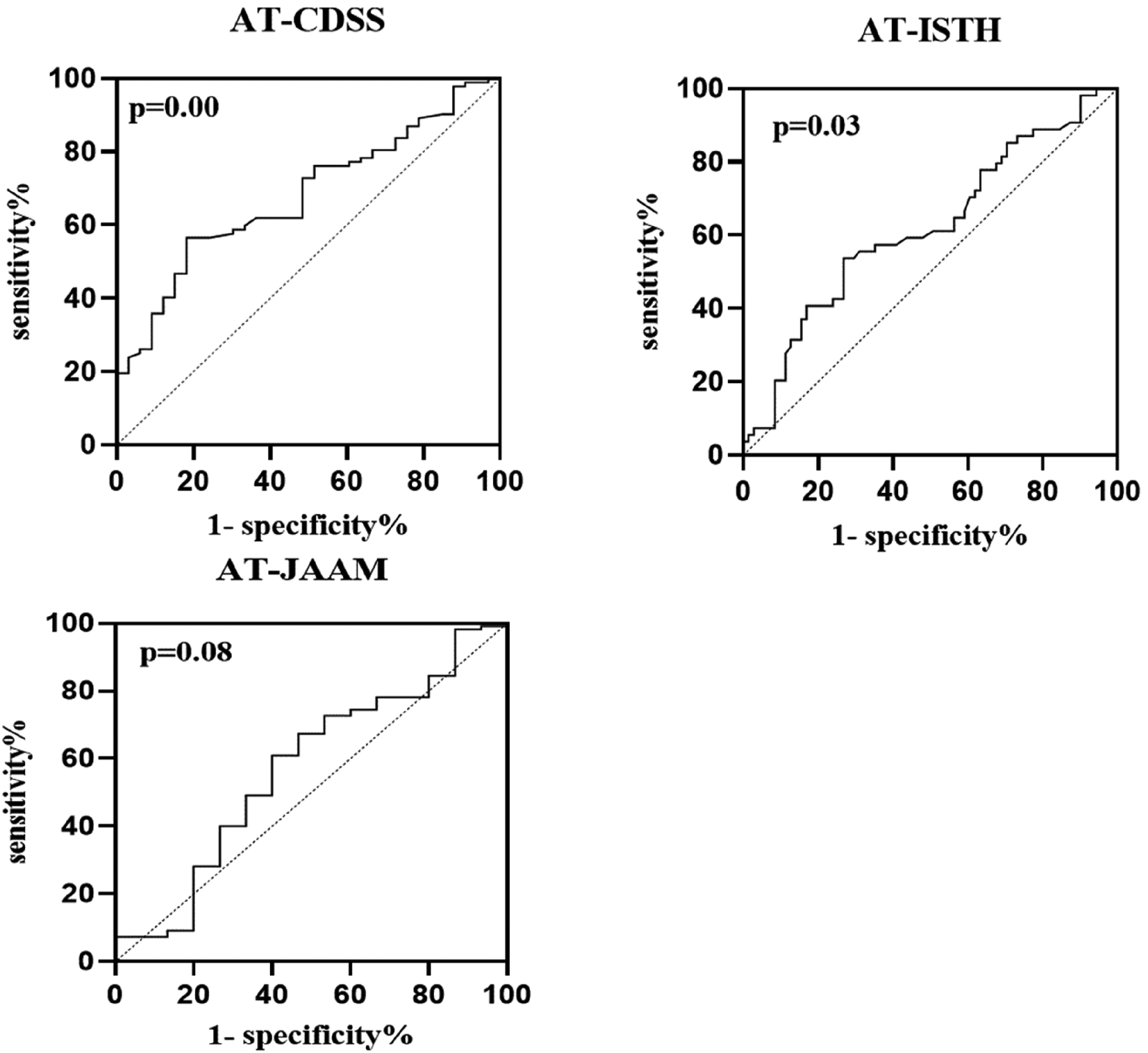
Receiver operating characteristic curve of AT for DIC diagnose (using ISTH, JAAM and CDSS as diagnostic standard). Abbreviations: ISTH, International Society on Thrombosis and Hemostasis; JAAM, Japanese Association for Acute Medicine; CDSS, Chinese DIC scoring system; AT, antithrombin.
Discussion
Sepsis is the most common precipitating factor of DIC and is characterized by coagulation activation and impaired fibrinolysis.3,9 Microcirculatory clot formation, mainly due to tissue factors expressed on macrophages, neutrophils, and damaged endothelial cells, is the fundamental pathogenesis in the process of coagulation activation. Moreover, some procoagulants such as PAI-1 produced by derangement endothelial cells play a crucial role in the suppression of fibrinolysis, 19 Therefore, sepsis-associated DIC is classified as suppressed fibrinolytic-type DIC, with the development of more common symptoms of organ dysfunction than hemorrhage. 18 Theoretically, this type of DIC can benefit from anticoagulant therapy. However, the effectiveness of anticoagulant therapy in sepsis-associated DIC remains controversial.20,21 Recent studies have reported that anticoagulant therapy greatly improves the clinical outcome of patients.22–24 In contrast, patients in the advanced stage of coagulopathy, including those satisfying the ISTH criteria of overt DIC, may not benefit from anticoagulant therapy, which is largely attributed to the increased risk of bleeding.20,25 This study aimed to identify septic patients with early coagulation disorder in the ICU departments of three comprehensive hospitals based on SIC criteria and to conduct further diagnostic and prognostic analyses.
This study first evaluated the clinical utility of three widely used DIC scoring systems in SIC patients. Good DIC diagnostic criteria should meet the following three conditions: (1) readily available and easy to use, (2) enable diagnostic accuracy, and (3) have prognostic value. 26 ISTH, the globally recognized DIC criterion, has shown some prognostic power, as evidenced by the proportional increase in mortality risk of SIC patients with higher ISTH scores in this study. A previous study also reported similar results, confirming the prognostic power of ISTH in DIC patients. 27 However, diagnosis may be delayed when using the ISTH criteria in sepsis. 28 The diagnosis rate of overt DIC in SIC based on ISTH was significantly lower than those of CDSS and JAAM. Notably, even in non-survival groups, the diagnostic rate was no more than 60%. Nonetheless, the diagnostic rate remains insufficient to reliably detect clinically critical syndromes. JAAM was designed specifically for the diagnosis of septic DIC and was the original template of the SIC criteria since the SIRS score was abandoned from the publication of Sepsis 3.0 6 ; therefore, JAAM demonstrated the highest diagnostic accordance rate for SIC patients. In our opinion, in the era of sepsis 3.0, SIC can replace JAAM due to its comparable diagnostic rate in the early sepsis stage. However, the predictive power of SIC for mortality was controversial in previous research. Iba et al highlighted the performance of the SIC score to predict 28-day mortality. 7 In contrast, Helms et al indicated that the specificity of the SIC score alone to predict mortality was very low. 29 Our study showed no evidence of a significant correlation between the scores of SIC and JAAM and the corresponding risk of mortality in multivariate analysis. Currently, CDSS has surpassed ISTH as the most widely used DIC criterion in China. Our analysis indicated that the CDSS had a relatively ideal ability for both diagnosis and prognosis. CDSS demonstrated a moderate DIC diagnostic rate in SIC (CDSS 73.6%, below the 88.0% of JAAM, but higher than the 43.2% of ISTH), with a comparable DIC diagnostic rate in the severe group (CDSS 87.5% vs JAAM 89.1%, P = 0.83). Similar to ISTH, the mortality risk of SIC patients increased proportionally with higher CDSS scores. Nevertheless, CDSS is the most complex DIC scoring system among these three and has not been widely applied outside of China. Some of the indicators included in the CDSS may be redundant. For example, fibrinogen is an acute-phase protein, and its plasma levels often remain within or beyond the normal reference range in sepsis. 30
Besides its anticoagulant properties, AT exerts anti-inflammatory effects in the context of sepsis. 31 AT plays a vital role in the attenuation of glycocalyx injury. The glycocalyx on the luminal surface of endothelial cells plays an essential role in maintaining antithrombogenicity in the vascular lumen. 10 Unfortunately, in septic patients, AT is rapidly consumed by thrombin and cleaved by neutrophil elastase and the bacterial enzyme thermolysin, resulting in a reduction in plasma levels. 32 The low AT levels are related to poor prognosis; hence, using recombinant AT is recommended during the early phase of sepsis in Japan. 33 Several Japanese studies have proposed incorporating AT activities into septic DIC scoring systems to guide preemptive anticoagulation therapy.18,34 The present study proved that AT had satisfactory and affirmative prognostic value for SIC. Univariate and multivariate analyses revealed that among all indicators, only AT and PT had a significant impact on mortality. In addition, when the cutoff value of AT referred to in JSTH was used to divide the SIC into two groups, the Kaplan-Meier survival curve analysis demonstrated that low AT activities (<70%) on admission were significantly correlated with higher mortality. The 28-day mortality in the Normal-AT group was 32.7% compared to 61.4% in the Low-AT group. Moreover, the decreasing tendency of AT after clinical interventions was correlated with increased mortality. 35 In the non-survival group, AT activity decreased significantly, which did not occur in the survival group. These results indicated that AT is an ideal prognostic indicator for SIC. Despite its outstanding prognostic ability, the diagnostic capabilities of AT, especially in the early stage of SIC, were further explored. The AU-ROC of AT showed statistical significance when the CDSS and ISTH were used as diagnostic standards, except for JAAM. Since JAAM exhibited the highest DIC diagnostic rate for SIC, the diagnostic power of AT for SIC seemed relatively limited. In summary, the results suggested that the prognostic value of AT was better than its diagnostic value for SIC. Adding AT to SIC may be an easy way to increase its prognostic power.
Nevertheless, the limitations of the present study should be acknowledged. First, this was a retrospective, multicenter study with a small sample size. A prospective study with a larger sample size is warranted to address these issues. Second, the application of LMWH for anticoagulant therapy was largely determined by the clinical experience of doctors in this study. This study found that anticoagulant therapy yielded no benefit in SIC. Third, only data from ICU patients were analyzed, with most of them being in serious condition with high modified SOFA and APACHE II scores when confirmed with SIC. Our next research will be a prospective study including SIC patients in the ICU, hematology departments, and infection departments to validate the utility of the SIC scoring system combined with AT.
Conclusion
Sepsis-induced disseminated intravascular coagulation is a life-threatening complication characterized by systemic activation of coagulation and suppression of fibrinolysis. Early detection of DIC is extremely important as the condition quickly progresses to multiple organ dysfunction and failure. SIC, the latest scoring system, focuses on the early detection of coagulation disorders in sepsis, enabling prompt initiation of treatment without missing any therapeutic opportunities. In this study, the diagnostic and prognostic value of three widely used DIC scoring systems were assessed in patients with confirmed SIC. JAAM exhibited the highest diagnostic rate for DIC among confirmed SIC cases, while the mortality rate of SIC patients demonstrated a proportional increase with higher ISTH and CDSS scores. In addition, the value of AT was analyzed in detail. SIC patients exhibited poor prognoses if they showed low AT activities at the time of confirmed SIC and/or a descending tendency in AT during treatment. In contrast to its remarkable prognostic value, the diagnostic value of AT for SIC remains relatively limited. Incorporating AT into the SIC scoring system may improve its accuracy in predicting mortality and increase its prognostic power.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 1.3.5 Project for Disciplines of Excellence, West China Hospital, Sichuan University, (grant number ZYJC21007).