
Abstract
Patient response to P2Y12 inhibitor therapy is heterogeneous, and those with high on-treatment platelet reactivity (HTPR) are at an increased risk of thrombotic complications. The aim of our study was to determine whether selecting a high-risk patient group of individuals after complex percutaneous coronary intervention (PCI) would show the clinical benefit of HTPR testing for preventing thrombotic complications. Blood samples of patients after complex PCI were acquired 1 day and 1 month after the intervention. The samples were tested using vasodilator-stimulated phosphoprotein phosphorylation (VASP-P) and platelet function assay (PFA). The occurrence of clinically significant stent thrombosis with repeated revascularization of the target vessel was observed over a 1-year period. One day after PCI, 37% of patients had HTPR as established by VASP-P. One month after PCI, the percentage of patients with HTPR decreased to 30.9%. According to PFA, 1 day after PCI, 33.3% of patients had HTPR. This percentage declined to 19.8% after 1 month. All measurements identified a significantly higher proportion of HTPR in patients on clopidogrel compared to ticagrelor and prasugrel. Two cases of early stent thrombosis and 1 case of late stent thrombosis were identified. Further study of adenosine diphosphate receptor blocker on-treatment response in patients undergoing complex PCI is necessary.
Keywords
Introduction
Cardiovascular disease (CVD) is the leading cause of mortality in Europe, accounting for 45% of all deaths. More than 4 million Europeans die every year from CVD, primarily from coronary artery disease (CAD). 1 Percutaneous coronary intervention (PCI) with stent implantation is the cornerstone of invasive CAD treatment. The presence of metal or polymer surface of the stent within the arterial lumen, however, promotes thrombogenesis, which can result in early stent thrombosis. Preserving patency of the implanted stent requires dual antiplatelet therapy consisting of aspirin and a P2Y12 inhibitor. Currently used oral agents in this group include clopidogrel, prasugrel, or ticagrelor. 2
Patient response to P2Y12 inhibitor therapy is heterogeneous. A portion of the patient population does not reach sufficient platelet inhibition levels despite a full dose of an antiplatelet agent. 3 This insufficient platelet inhibition is called high on-treatment platelet reactivity (HTPR). Patients with HTPR were repeatedly shown to be at an increased risk of ischemic complications after PCI.4,5 The highest prevalence of HTPR occurs in patients treated with clopidogrel, reaching between 16% and 50%. 6 Resistance to clopidogrel treatment is caused by a wide array of factors. The foremost factor appears to be a genetic variability of metabolism from a prodrug to an active agent by hepatic CYP2C19. 7 The effectivity of clopidogrel is also influenced by drug–drug interactions8,9 and complex factors such as obesity and diabetes mellitus. 10 Prasugrel and ticagrelor are newer, more potent P2Y12 inhibitors linked to considerably lower rates of HTPR. 11 On the other hand, they are also linked to a significantly increased risk of bleeding compared to clopidogrel.12,13 As recommended by current guidelines, clopidogrel is used both after PCI for chronic coronary syndrome (CCS) and for high-bleeding risk patients with acute coronary syndrome (ACS). Prasugrel or ticagrelor is used mainly in ACS patients or CCS setting with high ischemic risk.14–16
Term complex PCI usually describes interventions on the left main coronary artery, bifurcation lesions, multivessel disease, calcified lesions, or chronic total occlusions. These interventions have lower procedural success rates and a higher risk of recurrence and major adverse cardiac events than noncomplex lesions.17,18 The percentage of patients with findings of complex coronary lesions has risen steadily in recent years. 19 Moreover, due to the aging of the patient population and long-term trends in CAD risk factors, the number of patients with complex coronary lesions can be expected to increase further. This prospect highlights a need for an adequate antithrombotic regimen for patients requiring interventional treatment.
Methods
Design and Patients
This preliminary prospective observational single-center study investigated patients from the Department of Cardiology and Department of Internal Medicine, University Hospital Martin, Slovakia, who underwent PCI of a complex coronary artery lesion for non-ST-elevation ACS (NSTE-ACS) and CCS between February 2020 and June 2021. A complex coronary intervention was defined as PCI of a left main coronary artery, PCI of a calcified lesion requiring preparation with a scoring, cutting, or lithotripsy balloon, PCI of a bifurcation with a side branch diameter over 2.5 mm, stent implantation in the side branch or requiring kissing technique and PCI with implantation of 3 or more stents into a single coronary artery. Patients meeting inclusion criteria were identified by reviewing catheterization laboratory records. We excluded patients on long-term anticoagulation therapy, patients with PCI for an acute ST-elevation myocardial infarction, or PCI for a chronic total occlusion. Patients with diseases causing markedly abnormal levels of blood platelets (essential thrombocytosis, aplastic anemia, myelodysplastic syndrome, etc) were also excluded. The selection of a P2Y12 inhibitor was at the discretion of the treating physician in our institution. The choice was based on the current European Society for Cardiology dual antiplatelet therapy, 14 NSTE-ACS, 15 and CCS 16 guidelines, and was influenced by individual bleeding and ischemic risk of the patient. Clopidogrel treatment was initiated by a 300 mg loading dose followed by a 75 mg once daily maintenance dose, ticagrelor dosing was 180 mg loading dose followed by a 90 mg twice daily maintenance dose, and prasugrel dosing was a 60 mg loading dose followed by 10 mg once daily maintenance dose. The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Jessenius Faculty of Medicine, Comenius University in Bratislava, Slovakia.
Platelet Function Testing
Blood samples of these patients were collected 1 day after PCI and 1 month after PCI. The samples were tested using vasodilator-stimulated phosphoprotein phosphorylation (VASP-P) flow cytometric analysis and platelet function assay (PFA). The primary endpoint of this study was the level of platelet inhibition on day 1, but only patients that provided samples both after 1 day and 1 month were included in the final analysis, to enable observation of changes in platelet function over time.
The VASP-P measurements were carried out according to the manufacturer's instructions using a commercially available kit PLT VASP/P2Y12 (Biocytex, Marseille, France). Then 10 μL of citrate-anticoagulated whole blood was incubated with either prostaglandin E1 (PGE1) or PGE1 + adenosine diphosphate (ADP) and fixed in paraformaldehyde. Platelets were then permeabilized, labeled with an anti-CD61 phycoerythrin-labeled platelet-specific antibody and a fluorescein isothiocyanate-labeled anti-phosphorylated VASP (VASP-P)-specific mouse monoclonal antibody or an isotype control antibody. Samples were analyzed on a BD FACSVerse™ flow cytometer (BD Biosciences, Haryana, India). Geometric mean fluorescence intensity (MFI) values were determined in the presence of PGE1 with or without the addition of ADP. The extent of VASP-P was expressed as PRI calculated from the MFI values (after deduction of MFI obtained with isotype control) using the following formula: PRI (%) = (MFI PGE1 – MFI (PGE1 + ADP)/MFI PGE1 × 100. HTPR was defined by the flow cytometric VASP-P analysis as a PRI > 50%.20,21
The Innovance P2Y cartridge was used on the PFA-100 (Siemens Healthcare Diagnostics Products Gmbh, Marburg, Germany) according to the manufacturer's instructions. The Innovance P2Y is a cartridge specifically designed for the detection of P2Y12 receptor inhibitor activity. The cartridge contains a membrane coated with ADP, calcium, and PGE1. For this test, the cartridges were brought to room temperature for 30 min. Then 800 μL of citrate-anticoagulated whole blood was injected into each cartridge, and the test was started. Finally, the instrument measured the time to obtain complete occlusion of the aperture reported as “closure time” up to a maximum of 300 s. HTPR was defined by a closure time of under 208 s.20,21
Adverse Cardiac Events
The secondary endpoint was an occurrence of clinically significant stent thrombosis with the need for repeated revascularization of a target vessel. This data was obtained during an office visit scheduled 1 month after PCI and then was followed by means of an electronic health record (EHR) search. Acquired results were compared between patients classified as with and without HTPR.
Statistical Analysis
Data analysis was performed using STATISTICA v 5.0 (StatSoft, Tula, USA). Data were checked for normality with the Shapiro–Wilk test (data are displayed as mean ± standard deviation in the case of normally distributed ones and as median and range in the case of asymmetrically distributed ones). Mean VASP-P values were compared statistically between individual drugs. Patients were classified as with or without HTPR, and differences between these 2 groups were analyzed with a chi-squared test. A p-value of <.05 was considered statistically significant.
Results
Patient Population
One day after PCI, blood samples were acquired from 154 patients; 81 returned after 1 month for the second blood sampling and were eligible for the follow-up. Forty-four patients were on clopidogrel 75 mg o.d., 33 were on ticagrelor 90 mg b.i.d., 4 were on prasugrel 10 mg o.d. Fifty-seven of these patients were male, 24 were female, and the average age was 66.4 ± 9.5 years.
The predominant indication for PCI was NSTE-ACS at 51.9% (n = 42), CCS accounted for 48.1% (n = 39) of indications for PCI.
PCI of a combined complex lesion meeting more than 1 criterium (ie, calcified left main bifurcation) was represented at 40.7% (n = 33). PCI of a simple long lesion requiring 3 or more stents accorded for 24.7% (n = 20), PCI of a bifurcation lesion 16% (n = 13), and PCI of a calcified lesion requiring preparation with scoring, cutting, or lithotripsy balloon accorded for 12.4% (n = 10). PCI of a simple left main represented 6.2% (n = 5). The baseline characteristics are summarized in Table 1, additional population information including CAD risk factors and concomitant medications are outlined in Table 2.
Baseline Characteristics of the Studied Population.

Abbreviations: HTPR, high on-treatment platelet reactivity; PCI, percutaneous coronary intervention; ACS, acute coronary syndrome; CCS, chronic coronary syndrome.
When analyzed from the standpoint of meeting individual inclusion criteria, 55.6% (n = 45) of lesions involved a bifurcation, 34.6% (n = 28) can be defined as a long lesion requiring implantation of 3 or more stents into a single coronary artery, 24.7% (n = 20) lesions were calcified requiring preparation with scoring or lithotripsy balloon, and 40.7% (n = 33) of lesions involved the left main coronary artery.
Additional Population Information—Risk Factors of CAD and Concomitant Medication.
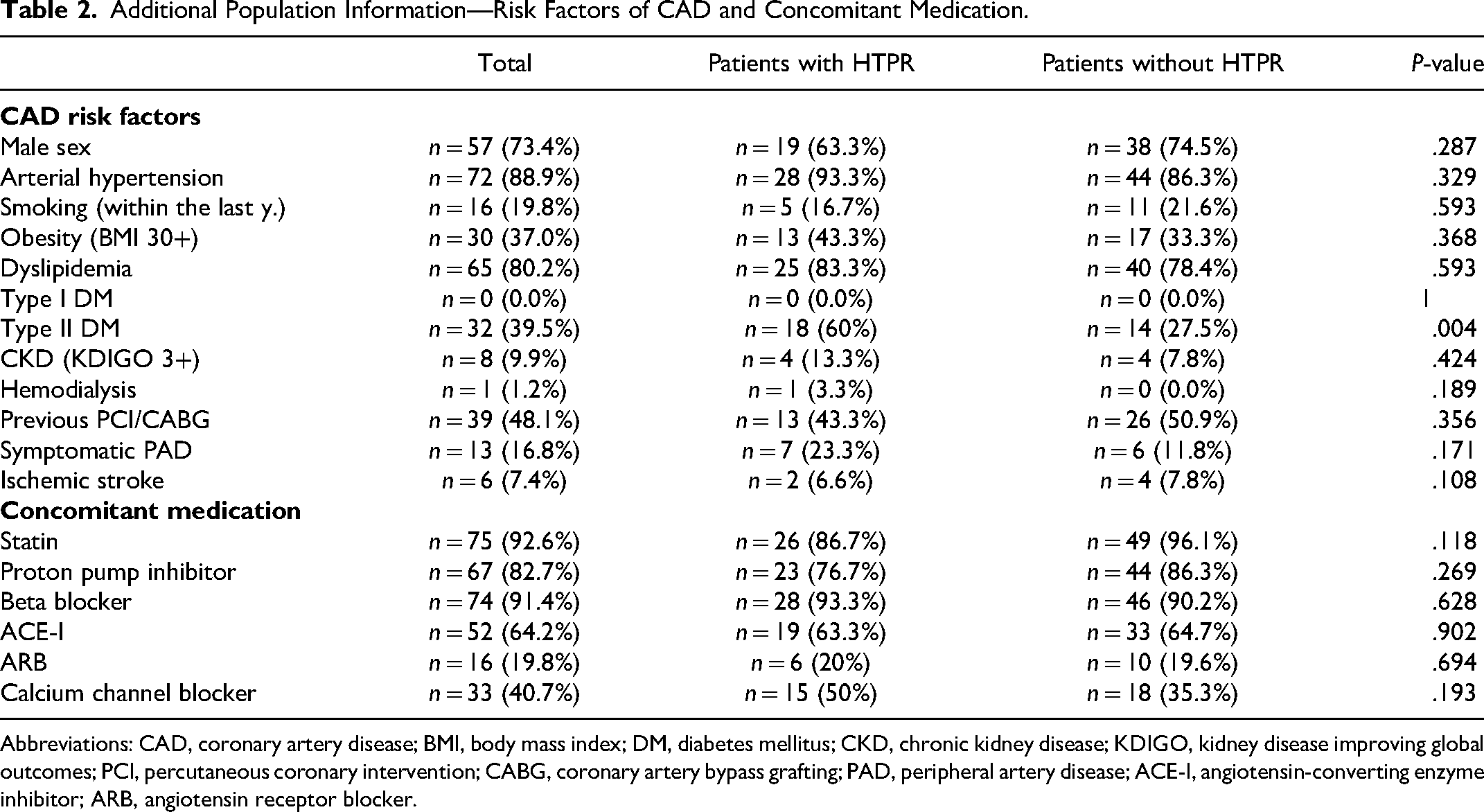
Abbreviations: CAD, coronary artery disease; BMI, body mass index; DM, diabetes mellitus; CKD, chronic kidney disease; KDIGO, kidney disease improving global outcomes; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; PAD, peripheral artery disease; ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker.
Platelet Reactivity and the Prevalence of HTPR
One day after PCI, 37% of patients (n = 30) had HTPR as established by VASP-P of more than 50%. One month after PCI, the percentage of patients with HTPR declined to 30.9% (n = 25). According to PFA, 1 day after PCI 33.3% of patients (n = 27) had HTPR established by PFA of <208 s, and 1 month after PCI this percentage decreased to 19.8% (n = 16).
From the standpoint of individual P2Y12 inhibitors, 59% (n = 26) of patients on clopidogrel had HTPR on day 1% and 50% (n = 22) on day 30 according to VASP; 50% (n = 22) on day 1 and 34.1% (n = 15) on day 30 according to PFA. In the ticagrelor subgroup 12.1% (n = 4) of patients had HTPR on day 1 and 9.1% (n = 3) on day 30 according to VASP; 15.2% (n = 5) on day 1% and 3% (n = 1) on day 30 according to PFA. The difference in the number of HTPR patients between the clopidogrel and ticagrelor subgroups was statistically significant (P < .05) in both measurements conducted with VASP-P and both conducted with PFA. All patients on prasugrel (n = 4) had adequate platelet inhibition according to VASP-P and PFA.
VASP-P results can also be analyzed as a mean for each measurement. The average VASP-P value on day 1 was 36.8%. The average value for clopidogrel patients was 49.4% and 21.3% for ticagrelor patients, respectively (P < .001). On day 30, the average VASP-P value was 32.9% with an average value for clopidogrel patients was 45.3% and 18.9% for ticagrelor patients (P < .001) (Figures 1 to 3).

VASP-P 1 day and 1 month after PCI (VASP-P value expressed in %. The red line represents the 50% cut-off, above which platelet inhibition is deemed insufficient).

PFA 1 day and 1 month after PCI. (PFA value expressed in seconds. The red line represents the 208 s cut-off, below which platelet inhibition is deemed insufficient. Purple line marks samples evaluated by the assay as 300 + seconds).

High on-treatment platelet reactivity (HTPR) in individual P2Y12 inhibitors grouped by day and method of testing. (Values expressed: the number of patients with HTPR on an individual P2Y12 inhibitor grouped by day and method of testing [n]. The overall number of patients on clopidogrel is 44, and on ticagrelor is 33. Four patients on prasugrel are not visualized in this graph, as none of these patients had HTPR. The p-value of comparison between clopidogrel and ticagrelor patients in measurements on the corresponding day with the corresponding method of testing is <.01.).
Adverse Cardiac Events
Three instances of stent thrombosis occurred during a 1-year follow-up. Two were cases of early stent thrombosis 2 and 21 days, respectively, after PCI. Both patients were on clopidogrel and had inadequate platelet inhibition according to VASP-P (50.1% and 51.53%, respectively, 54.6% and 61.4%), results according to PFA were inconclusive (57 s and 300+ s, respectively, 300+ s and 112 s). The third case was a late stent thrombosis 8 months after PCI in a patient on ticagrelor with adequate platelet inhibition according to both VASP-P and PFA (VASP-P 8.97% and 10.8%; PFA 300+ s and 300+ s). The connection between HTPR and stent thrombosis was not statistically significant with VASP-P (p-values: .279 and .171) nor with PFA (p-values 1 and .547). From the location standpoint, 1 case of stent thrombosis occurred in mid-left anterior descending artery (LAD), and 2 cases of stent thrombosis occurred in the left main.
Discussion
Multiple studies have shown that patients with HTPR during P2Y12 inhibitor treatment are at greater risk for major adverse cardiac events. 5 Subsequently, several randomized controlled trials have studied the personalization of antiplatelet therapy based on platelet function testing (PFT). However, these trials provided conflicting results.22–27 We have focused on the patient population with complex coronary lesions. These patients are at a higher risk of thrombotic complications after a coronary intervention.
Overall, we detected 30 patients with HTPR according to VASP-P, 26 of these patients were on clopidogrel, and only 4 were on ticagrelor. The prevalence of HTPR in the clopidogrel group measured with both VASP-P and PFA was at 56% and 50%, respectively. This high percentage is consistent with several, mostly Asian trials, and sits at the upper range of the data collected by the authors of the HTPR consensus paper. 6 After 1 month there was a drop in the number of patients with HTPR primarily driven by the clopidogrel group. A similar development was seen in both VASP-P and PFA results. Presumably, patients have achieved more adequate platelet inhibition after a prolonged period of exposure to clopidogrel given its variable absorption and conversion from prodrug. The prevalence of HTPR on ticagrelor was significantly lower in all measurements also in accordance with data from earlier studies. 11 We have not detected a case of HTPR in patients on prasugrel, however, the number of patients on prasugrel was marginal (n = 4).
The rate of 1-year stent thrombosis after PCI is approximately 0.8%.
28
In our high-risk patient population undergoing complex PCIs, the rate of clinically significant stent thrombosis more than quadrupled
The majority of left main interventions (21 out of 33) were intravascular ultrasound (IVUS) guided in this study. Two cases of stent thrombosis occurred after left main stenting, and in both cases, stent apposition was deemed adequate after IVUS control. IVUS and optical coherence tomography can reduce the risk of stent thrombosis attributable to mechanical complications, such as stent malposition or fracture. 29 However, the limitations of intracoronary imaging are nonnegligible financial cost and the additional time required for performing the imaging. 30 Recommendations for the utilization of intravascular imaging remain unclear and mainly at the level of expert consensus due to the paucity of randomized controlled trial data. However, the benefit of these methods appears to be the greatest in complicated lesions. 31
Detection of HTPR after complex PCI is most pertinent in patients treated with clopidogrel. Even though all the methods of HTPR detection have limited specificity, VASP-P is recognized as the most reliable assessment method of platelet inhibition due to the specific measurement of P2Y12 receptor activity. 20 Furthermore, intravascular imaging as a method of detecting mechanical causes of stent thrombosis is deemed more time and cost-effective in complex lesions. 31 The high-risk patient population with complex lesions may benefit from a broader adoption of PFT to assist with the choice of the P2Y12 inhibitor to balance ischemic and bleeding risks. This step, together with a wider utilization of intravascular imaging, can help improve outcomes for high-risk populations.
Our study has several limitations. First is a relatively small sample size. This problem was exacerbated by a very high drop-out rate (47.4%) between the first and second measurements. The study took place at the height of the COVID-19 pandemic, and this fact might have reduced the willingness of patients to return to the hospital for the second measurement. The plan for an office visit after 1 year was abandoned and replaced by an EHR search for the same reason. Second, the small number of events precludes us from reaching a statistically significant result. Third, intravascular imaging was not used in all procedures because of cost and time constraints, thus a mechanical cause of stent thrombosis cannot be definitively ruled out. Fourth, the assessment of adherence to P2Y12 therapy after discharge was based on patient self-report during an office visit after 30 days. This limitation stands out, especially in ticagrelor with its twice-daily dosing and relatively frequent occurrence of side effects (eg, dyspnea). Fifth, we did not perform a subanalysis of some of the possible baseline differences (the criteria for selection of P2Y12 inhibitor, length of the lesions, presence of bifurcation lesions, and presence of type 2 diabetes) that could, in theory, influence on-treatment platelet reactivity and the risk of post-PCI ischemic adverse events. Finally, all the interventions were not performed by the same operator, and the study is of a nonrandomized design.
Conclusion
The study identified HTPR in 37% of the investigated patients after complex PCI. Our results identified a significantly higher proportion of HTPR in patients on clopidogrel compared to ticagrelor and prasugrel. Two cases of early stent thrombosis were identified in patients with HTPR on clopidogrel, and 1 case of late stent thrombosis occurred in a patient on ticagrelor with adequately inhibited platelet reactivity. Based on our results, further study of ADP receptor blocker on-treatment response in patients undergoing complex PCI is necessary.
Footnotes
Authors’ Contributions
Matej Samoš, Ján Staško, and Lukáš Urban conceptualized and planned the methodology of the study. Lukáš Urban enrolled potential patients. Ingrid Škorňová and Jana Žolková performed laboratory testing. Lukáš Urban analyzed the data and drafted the manuscript. Matej Samoš and Tomáš Bolek obtained the necessary resources for the study and supervised its performance. All authors read and approved the final manuscript.
Availability of Data and Material
All data and material analyzed during the study are available from the corresponding author upon reasonable request.
Consent to Participate
Informed consent was obtained from all subjects involved in the study.
Consent for Publication
Written informed consent was obtained from the patients to publish this paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Jessenius Faculty of Medicine, Comenius University in Bratislava, Slovakia.
Funding
This study was supported by Slovak Research and Development Agency grant (APVV 16-0020).