
Abstract
Aim
To investigate the clinical application of thromboelastography (TEG) in severe fever with thrombocytopenia syndrome (SFTS).
Methods
One hundred and fifty-seven patients with SFTS were included in the study. The participants were distributed into 3 groups; A, B, and C. And 103 patients in group A met the clinical criteria as they exhibited slight liver and kidney dysfunction. Group B consisted of 54 patients with SFTS who were critically ill while group C was a healthy control group with 58 participants.
Results
Patients with SFTS exhibited lower coagulation than the healthy participants. Group B patients exhibited significantly lower coagulation compared to group A. There was no significant difference in platelet count and fibrinogen content between patients in group A and group B, but platelet aggregation function and fibrinogen activity were significantly lower in group B patients.
Conclusion
Our results suggest that it is risky to solely rely on platelet count and the fibrinogen in SFTS. Monitoring of TEG and other coagulation indexes should be emphasized.
Introduction
Severe fever with thrombocytopenia syndrome (SFTS) is a natural focal disease caused by a novel bunyavirus. The new bunyavirus is also known as SFTS virus (SFTSV). The main clinical manifestations of infection with this new bunyavirus are fever, thrombocytopenia, leukopenia, and multiple organ damage. The SFTSV is a member of phlebovirus, one genus in the family of Bunyaviridae, which was isolated and identified by Chinese scholars for the first time. 1 The prevalence of SFTS has been increasing since its discovery, and the incidence area has been expanding. This new virus mostly exists in mountainous, hilly, and forest areas, and the infection is more common in farmers and the elderly. The occurrence of SFTS has obvious seasonality. Spring and summer are the high incidence seasons of the disease, April to October are the epidemic period, May to July are the epidemic peak period, the epidemic peak in Shandong Province are June to July.2,3 At present, it is generally believed that the transmission of SFTSV is related to ticks. It has a high mortality rate, and is hard to be controlled. There is no specific drug and vaccine for prevention that works well. The mortality in some areas can be as high as 30%. The average mortality of SFTS in China was 5.3% during 2010 to 2017.4,5
Thromboelastography (TEG) was invented by German Harter in 1948. It can detect the level of coagulation factor, fibrinogen function, platelet aggregation function and whether there is hyperfibrinolysis by activating trace whole blood in vitro. The results of TEG can reflect the real-time coagulation state of the body, which is of great significance for judging the cause of bleeding, evaluating the perioperative risk of patients and monitoring the effect of anticoagulant drugs. Routine coagulation function tests, such as prothrombin time (PT) and (APTT), detect the activity of coagulation factors in plasma without the participation of blood cells such as platelets. It only tests a part of the in vitro plasma and coagulation cascade reaction, and only describes the coagulation process piecemeal and partially, reflecting the mechanism of a small part of thrombin formation in the early stage of coagulation. The platelet-related detection in blood routine test is limited to the description of count and platelet morphology, and does not reflect the aggregation function of platelets. TEG has unique advantages in detecting fibrinogen activity and platelet aggregation function. After decades of development, TEG has been widely used in various fields such as heart surgery, postpartum hemorrhage, hemophilia, and brain trauma surgery.6–8
So far, many studies have analyzed the etiology, epidemiology, clinical characteristics, and treatment of SFTS,9–12 but there are few studies on the application of TEG in SFTS. This article retrospectively analyzed the clinical data and TEG test results of 157 patients with SFTS diagnosed in the laboratory of Weihai Central Hospital of Shandong Province from January 2018 to December 2020, and discussed the potential application value of TEG in the treatment of patients with SFTS.
Materials and Methods
Subjects and Groups
We collected the clinical data of patients with SFTS diagnosed in Weihai Central Hospital from January 2018 to December 2020 according to the guidelines for the prevention and treatment of fever with thrombocytopenia syndrome (2010 version) 13 issued by the Ministry of health of China. According to these guidelines, a patient is considered a probable case if he or she presents with acute fever, thrombocytopenia and leucopenia interpreted together with an epidemiological exposure by virtue of having lived, worked or traveled to an endemic area or having had contact with ticks 2 weeks prior to the manifestation of the disease. A confirmed case is defined as satisfying one or more of these criteria: seroconversion accompanied by a 4-fold increase in IgG titers between acute and convalescent blood samples taken 2 weeks apart; a positive culture; or a positive molecular detection of the viral RNA.
On excluding patients with unclear outcomes such as those referred elsewhere and cases with incomplete relevant data, 157 patients with SFTS were included in the study after screening, all of whom were residents of Weihai, China. The study was approved by the Ethics Committee of Weihai Central Hospital.
The participants were divided into 3 groups A, B, and C, of which group A was the improved/discharged group. The patients in this group met the clinical discharge criteria and presented with slight liver and kidney dysfunction, a total of 103 cases. Group B was the critically ill group consisting of 54 patients who gave up treatment due to serious illness or died due to serious virus infection. Group C was the healthy control group composed of 58 healthy participants recruited from the physical examination center of Weihai Central Hospital.
Sample Collection and TEG Detection
Whole blood samples were collected and anticoagulated with 3.2% sodium citrate. The samples were then sent to the laboratory in time, incubated at 37 °C for 15 min according to the standard operating procedures, and prepared the equipment and reagents required for TEG test as required. After the samples and reagents were prepared, we used TEG5000 thromboelastogram analyzer (Haemoscope Corp, USA) to carry out general TEG test according to the TEG operating procedures. The TEG analyzer automatically records the dynamic changes of blood clot, dynamically analyzes the whole process of coagulation and fibrinolysis in the form of curve, and obtains the results of coagulation state after comprehensive analysis of the measured parameters.
Statistical Analysis
Data analysis was performed using SPSS 19.0 statistical software package. Normality of the data was tested with Kolmogorov-Smirnov test with P > .05 indicating normal distribution. Normally distributed data was expressed as mean ± standard deviation, and the comparison between the 2 groups done using an independent sample t-test. Skewed data was expressed as median or interquartile range (P25-P75), nonparametric rank sum test was used for comparison between the 2 groups. The 3 groups were compared by one-way analysis of variance. The data counts were expressed as frequency (composition ratio), and the chi-square test used for inter group comparison. All tests were 2-sided and the difference was statistically significant when P value was <.05.
Results
Epidemiological and Clinical Characteristics of Patients With SFTS
There were 103 cases (48 males and 55 females) in the improved/discharged group (group A) with an average age of 64.11 ± 10.27 years, and 54 cases (33 males and 21 females) in the critically ill group (group B) with an average age of 71.61 ± 8.41 years. There was a significant difference between patients with critical illness (group B) and those in the improved/discharged group (group A) in terms of age, diabetes, neuropsychiatric symptoms, requirement for hemostasis therapy, temperature on admission, requirement for intensive care unit (ICU) treatment and length of hospitalization. However, there was no significant difference observed in the ratios of patients with abnormal TEG parameters and coagulation markers. The details are as shown in Table 1.
Epidemiological and Clinical Characteristics of Patients With SFTS.
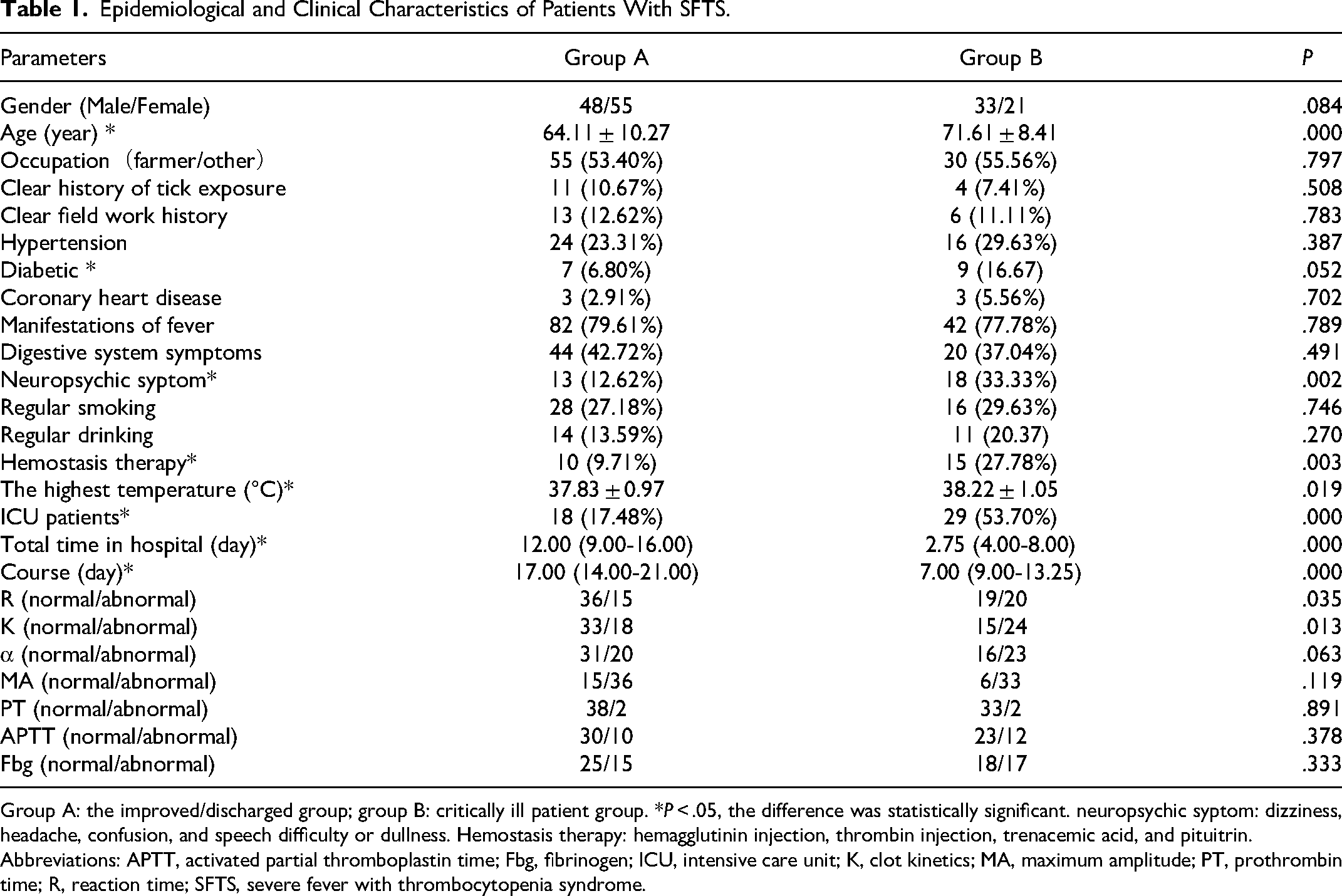
Group A: the improved/discharged group; group B: critically ill patient group. *P < .05, the difference was statistically significant. neuropsychic syptom: dizziness, headache, confusion, and speech difficulty or dullness. Hemostasis therapy: hemagglutinin injection, thrombin injection, trenacemic acid, and pituitrin.
Abbreviations: APTT, activated partial thromboplastin time; Fbg, fibrinogen; ICU, intensive care unit; K, clot kinetics; MA, maximum amplitude; PT, prothrombin time; R, reaction time; SFTS, severe fever with thrombocytopenia syndrome.
Analysis of TEG Results in Patients With SFTS
After admission, the first TEG results of patients with SFTS before treatment were compared with those of the healthy control group. Seventy-nine cases in the improved/discharged group (group A) were included in the analysis, and 40 cases in the critically ill patient group (group B) were included in the analysis. Compared with the healthy control group, patients with SFTS were older and in a relatively low coagulation state. In patients with SFTS, compared with the improved/discharged group, the patients with critical illness were older and had lower coagulation function. Details are shown in Table 2.
Comparison of TEG Levels Between Patients With SFTS and Healthy Controls.
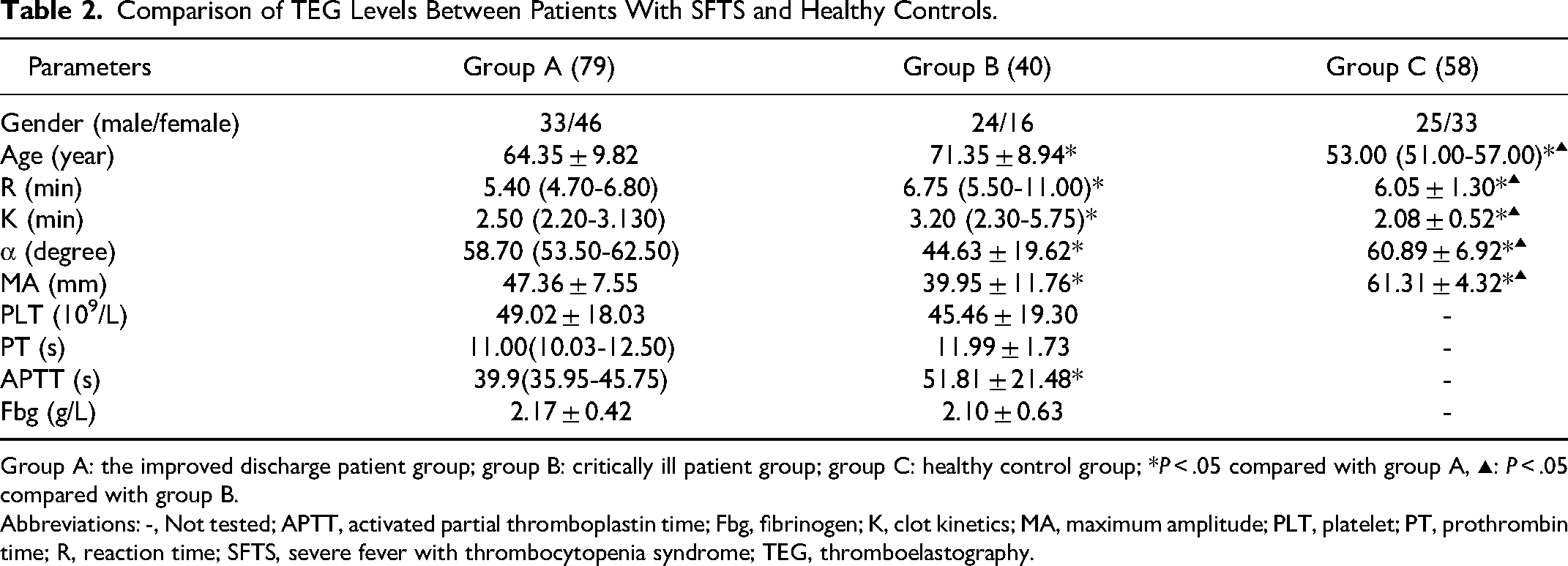
Group A: the improved discharge patient group; group B: critically ill patient group; group C: healthy control group; *P < .05 compared with group A, ▴: P < .05 compared with group B.
Abbreviations: -, Not tested; APTT, activated partial thromboplastin time; Fbg, fibrinogen; K, clot kinetics; MA, maximum amplitude; PLT, platelet; PT, prothrombin time; R, reaction time; SFTS, severe fever with thrombocytopenia syndrome; TEG, thromboelastography.
Transfusion of Blood Products in Patients With SFTS
We analyzed the transfusion requirement for platelets, plasma, and cryoprecipitate in patients with SFTS and found that the probability of transfusion of various blood products in patients with critical illness was different from that in patients with mild illness group. The probability of transfusion of cryoprecipitate in patients with severe illness was significantly higher than that in patients with mild illness. The details are shown in Table 3.
Statistics of Blood Transfusion in Patients With SFTS.

Group A: the improved discharge patient group and group B: critically ill patient group. *P < .05.
Abbreviations: RBC, red blood cell; SFTS, severe fever with thrombocytopenia syndrome.
Discussion
The main feature of patients with SFTS is fever accompanied by thrombocytopenia. The course of infection can be divided into fever, progression, and recovery stages. 14 Patients with severe condition often die due to multiple organ failure. In this study, according to the analysis results in Table 1, the ICU hospitalization time of critically ill patients was longer and the total course of disease shorter, which suggests that the condition of critically ill patients changed more rapidly getting worse. At present, there is no specific drug for SFTSV infection. The main treatments include etiological treatment, immune support treatment, plasma exchange, symptomatic support treatment, etc.15–17 The guidelines for the prevention and treatment of fever with thrombocytopenia syndrome issued by the Ministry of Health of China 13 pointed out that when the patient's platelet count is <30 × 109/L with coagulation dysfunction, platelet, cryoprecipitate, and fresh frozen plasma should be infused according to the patient's situation. At present, there are few studies on the quantity and timing of blood transfusion products in patients with SFTS with coagulation dysfunction, which requires that the coagulation function of patients be comprehensively and systematically evaluated and monitored in the process of diagnosis and treatment of patients with SFTS, and a reasonable and effective personalized treatment scheme be formulated according to the clinical situation of patients so as to further reduce the mortality.
Studies have shown that as people grow older, the coagulation function of body tends to enhance, and the normal elderly are in a relatively hypercoagulable state.18–20 Through the analysis of the data, we found that patients with SFTS were older, but in an obvious low coagulation state, especially in the critically ill group. At present, the clinical monitoring of patients’ coagulation function includes PT, APTT, and other traditional coagulation markers and platelet count.
There was no significant difference in fibrinogen content and platelet count between patients in bad state and improved/discharged group, but fibrinogen activity and platelet aggregation function are significantly lower in the worse-off patients. These results tell us that the decline of fibrinogen activity and platelet aggregation function is earlier than the decline of its content in patients with SFTS, especially critically ill patients, which gives us an important guidance, that is, relying solely on the detection results of fibrinogen content and platelet counts may mislead clinical treatment.
Previous studies suggest that TEG has unique advantages in monitoring coagulation function in patients with some specific diseases.21,22 TEG can accurately reflect the activity of fibrinogen and the aggregation function of platelets, which makes up for the shortcomings of traditional coagulation indexes and platelet count. In this study, fibrinogen activity and platelet aggregation function were not measured directly. These parameters were obtained from maximum amplitude of TEG which reflects both.
Patients with SFTSV were older and with a poor immune function. These patients often suffered from diabetes, hypertension, coronary heart disease, and other underlying diseases. The coagulation function of patients with SFTS was in a relatively low coagulation state, and the decrease of platelet and fibrinogen quantity and function was particularly obvious for critical patients, which may have led to the rapid aggravation of patients’ condition especially in the case of visceral hemorrhage and intracerebral hemorrhage which usually bring great challenges to clinical treatment.
Table 3 shows that the transfusion probability of platelet, plasma, cryoprecipitate, and other blood products in critically ill patients was higher than that of the improved/discharged group with the transfusion probability of transfusion with cryoprecipitate significantly different. It is probable that increasing number of cases in this study would have increased the probability of transfusion with all blood products in the critically ill to significant levels. That aside, this study suggests that judging whether to infuse blood products on the basis of platelet counts and fibrinogen content only cannot effectively reduce the risk of bleeding in SFT. Accordingly, there is need to emphasize the dynamic monitoring of TEG and other coagulation parameters.
Footnotes
Acknowledgements
All participants are grateful to Department of Blood Transfusion Laboratory (Weihai Central Hospital, Weihai, China) for the assistance rendered in the collection and analysis of samples.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.