
Abstract
Background
Heparin-induced thrombocytopenia (HIT) is a common differential diagnosis in cardiothoracic surgery. The latex immunoturbidimetric assay (LIA) is an enhanced immunoassay that has recently been introduced for the detection of total HIT immunoglobulin and retains a higher specificity of 95% compared to the enzyme-linked immunosorbent assay.
Objectives
To investigate if a semiquantitative relationship exists between increasing LIA levels beyond the current positivity threshold and its correlation to positive serotonin release assay results in cardiothoracic surgery.
Methods
This was a multicenter, observational cohort of cardiothoracic surgery patients initiated on anticoagulation with heparin-based products. To conduct sensitivity and specificity analysis of LIA values, HIT positive was defined as a LIA value ≥1 unit/mL and HIT negative was defined as a LIA level <1 unit/mL. A receiver operating characteristic (ROC) analysis was utilized to evaluate the predictive performance of the LIA.
Results
At the manufacturer cutoff of ≥1 unit/ml, LIA sensitivity and specificity was 93.8% and 24%, respectively, yielding a false positive rate of 76%. At a higher cutoff of 4.5 units/mL, LIA sensitivity and specificity was 75% and 71%, respectively, yielding a false positive rate of 29% and an area under the ROC curve of 0.75 (P = .01; 95% confidence interval: 0.615 - 0.88). Bivalirudin was initiated in 84.6% of false positive LIA results.
Conclusion
This study suggests that the diagnostic accuracy of the LIA can be optimized by increasing the LIA positivity threshold. Proposing a higher LIA cutoff, may mitigate unwarranted anticoagulation and bleeding outcomes.
Introduction
Thrombocytopenia is commonly seen in critically ill patients with an incidence varying between 35% and 45%. Cardiothoracic surgical patients (CTS) and those requiring mechanical circulatory support are particularly susceptible. The prolific use of heparin for circuit patency in cardiopulmonary bypass (CPB) and in extracorporeal membrane oxygenation (ECMO) places heparin-induced thrombocytopenia (HIT) as a common differential diagnosis. Artificial surfaces used in CPB and ECMO circuits are responsible for a pronounced elevation in platelet factor 4 (PF4) release generating a substrate for developing HIT with an incidence of 0.1% to 4% in CTS.1,2 Alternative causes for postoperative thrombocytopenia ranging from hemodilution and consumptive processes to prothrombotic pathologies make the clinical diagnoses for HIT challenging.2–6
Existing diagnostic tools include clinical risk scores along with confirmatory functional and immunoassays each with respective limitations. 7 Screening tools, such as the 4Ts score, provide a formidable negative predictive value in the general population but have not been reproduced in CTS. The positive predictive value of the 4Ts score is poor with a 9% to 17% predictive value.8,9 The enzyme-linked immunosorbent assay (ELISA), a commonly used immunoassay, yields a high sensitivity (98%-99%) for detecting HIT antibodies but limited in specificity, thus yielding a high risk of false positives.10,11 Functional assays, such as the serotonin release assay (SRA), are considered a gold standard test for HIT diagnosis with a combined sensitivity and specificity of 90% to 100%. However, the SRA is technically demanding and therefore limited to select laboratories resulting in prolonged turnaround times. 7
Given the limitations of existing immunoassays, novel laboratory tests such as the latex immunoturbidimetric assay (LIA) have been developed. The LIA is the first fully automated latex-enhanced immunoassay that has recently been introduced for the detection of total anti-PF4/heparin immunoglobulins via competitive inhibition, and therefore, decreased aggregation of latex nanoparticles coated with a HIT-mimicking monoclonal antibodies. As compared to ELISA, this on demand test can be performed in approximately 20 minutes. A LIA value ≥1 unit/mL confers a positive test.12,13 The specificity and positive predictive value of the LIA was noted to be superior with a 90% agreement to an SRA as compared to the ELISA at 75% while maintaining an equivalent negative predictive value.13,14 The LIA is also suggestive of having a higher sensitivity than the 4Ts score in predicting the likelihood of HIT. As a result of varied differential diagnoses and limitations of established assays, HIT is often over diagnosed and exposes patients to unnecessary bleeding risk with irreversible nonheparin anticoagulants. Understanding how LIA's enhanced diagnostic characteristics perform in a high-risk CTS cohort is vital in mitigating hemostatic complications. Unlike the ELISA, it is important to note that to date, studies which have formally validated or established a true semiquantitative correlation between LIA values and SRA positivity were not conducted specifically in a cardiothoracic surgical population, and instead used a heterogenous demographic.12,15,16 The assumption that specificity will increase as LIA values rise beyond the currently established positivity threshold (≥ 1 unit/mL) without compromising sensitivity is unknown. Moreover, due to the increased risk of HIT in post-CTS patients, it is important to establish and evaluate the validity of LIA thresholds in this cohort. The goal of this study, therefore, was to identify if a semiquantitative relationship exists between LIA values and SRA positivity specifically in CTS patients.
Methods
This was a multicenter, observational, retrospective, cohort study performed in CTS patients at a quaternary medical center from 2018 to 2020. Approval was obtained from the Institutional Review Board at AdventHealth-Orlando (IRB-1685388). Inclusion criteria consisted of adults ≥18 years of age, CTS, initial anticoagulation with unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH), and collection of combined LIA and SRA tests. Upon chart review, 4Ts scores were calculated to evaluate the clinical probability of HIT.
The primary objective was to investigate if a semiquantitative relationship exists between increasing LIA values beyond the current positivity threshold and its correlation to positive SRA results in the diagnosis of HIT in CTS patients. Patients were divided into 2 cohorts, SRA positive and SRA negative. Typically, SRA samples were only analyzed in those patients with a positive LIA (Figure 1). Within each cohort, sensitivity and specificity analysis of LIA thresholds were conducted. LIA positivity for HIT was defined as a value ≥1 unit/mL and HIT negative was defined as a value <1 unit/mL. Secondary endpoints included the use of alternative anticoagulation limited to bivalirudin and fondaparinux, duration of bivalirudin or fondaparinux, false positive LIA results in SRA negative patients, calculated 4Ts score correlation with LIA values, and prevalence of bleeding. Bleeding was predefined as any documentation of overt bleeding requiring surgical intervention upon chart review, drop in hemoglobin level of ≥2 g/dL, or red blood cell transfusion requirements.

Institutional HIT diagnostic and treatment pathway. **National Reference Laboratory—ARUP Laboratories: 500 Chipeta Way Salt Lake City, UT, USA. Abbreviations: HIT, heparin-induced thrombocytopenia; LIA, latex immunoturbidimetric assay; SRA, serotonin release assay.
The primary endpoint, defined as the semiquantitative relationship between LIA values and SRA positivity, was analyzed using an area under the receiver operating curve (AUROC) analysis. Sensitivity and specificity for each LIA value
Results
Of the 200 patients reviewed, 100 patients met inclusion criteria. Patients included were predominantly male (73%), with a mean age of 60 years. Indications for CTS included ECMO runs in 34 patients with the remaining indications being non-ECMO in nature including coronary artery bypass graft, valve replacements, lung, and heart transplant. One patient was initially anticoagulated with LMWH and the remaining 99 patients received UFH. LIA values ≥ 1 unit/mL were present in 80% of the patients and prevalence of SRA positivity was 16% (Table 1).
Patient Demographics.

Abbreviations: CKD, chronic kidney disease; CT, cardiothoracic; ECMO, extracorporeal membrane oxygenation; LIA, latex immunoturbidimetric assay; SRA, serotonin release assay; UFH, unfractionated heparin; VTE, venous thrombotic embolism.
Our study cohort consisted of 84 SRA negative and 16 SRA positive patients. Baseline characteristics were equally distributed between SRA negative and SRA positive patients except for age, stroke, 4Ts scores, and LIA positivity (Table 2). Of the 16 patients identified with a positive SRA test, 15 had LIA values ≥ 1.0 unit/mL (true positive) and 1 had a LIA value < 1 unit/mL (false negative). In the 84 patients who had a negative SRA result, 65 had a LIA ≥ 1.0 units/mL (false positive) and the remaining 19 had a LIA < 1.0 unit/mL (true negative).
Patient Demographics Based on SRA Result.

Abbreviations: CKD, chronic kidney disease; ECMO, extracorporeal membrane oxygenation; LIA, latex immunoturbidimetric assay; SRA, serotonin release assay; VTE, venous thrombotic embolism.
Sensitivity and specificity of the LIA at various cutoffs are shown in Figure 2. The aggregated data for all CTS patients show that the current cutoff for LIA positivity of 1 unit/mL is highly sensitive. However, it lacks specificity and results in elevated false positivity rates. Alternatively, a LIA value of 4.5 units/mL tempers sensitivity but improves specificity from 24% to 71% (Table 3). Using a LIA threshold of 4.5 units/mL resulted in an AUROC predictive diagnosis for HIT of 0.75 (95% confidence interval [CI] 0.615 - 0.88; P = .01).

LIA AUROC at various LIA cutoffs. Abbreviations: AUROC, area under the receiver operating curve; LIA, latex immunoturbidimetric assay.
Sensitivity and Specificity Analysis.
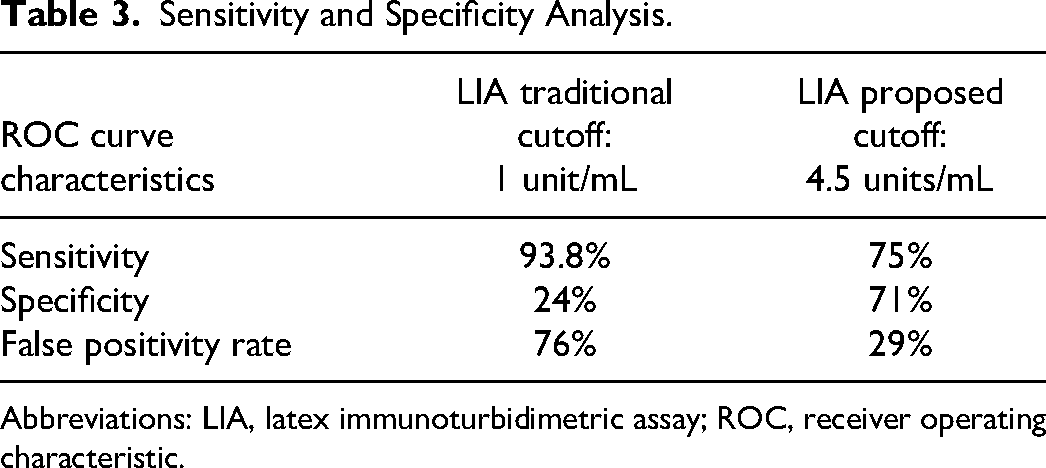
Abbreviations: LIA, latex immunoturbidimetric assay; ROC, receiver operating characteristic.
Secondary endpoints are shown in Table 4. Alternative anticoagulation was initiated in 79.8% and 93.8% of SRA negative and positive patients, respectively. Median days on alternative anticoagulation were 5 days in SRA negative and 9.5 days in SRA positive patients (P = .007). Overall, there were a total of 65 patients with LIA false positive results in which 55 were initiated on bivalirudin (84.6%). Clinically significant bleeding was more common in SRA negative patients (P = .0004). Correlation of 4Ts with LIA values are shown in Table 5.
Secondary Endpoints.

Abbreviations: LIA, latex immunoturbidimetric assay; SRA, serotonin release assay.
4Ts Score Correlation With LIA Values.

Abbreviations: LIA, latex immunoturbidimetric assay; n/a, not applicable.
Stratum-specific likelihood ratios (SSLR) were calculated to determine the odds of a true HIT diagnosis. The SSLR results separated by LIA value tertiles indicate an increasing probability of diagnosing true HIT as LIA values rise. Incorporating data from the main AUROC analysis, a LIA threshold of 4.5 units/mL or higher increases the likelihood of having true HIT from 1.21 (with a LIA value of ≥ 1 unit/mL) to 2.6 (Table 6).
Stratum Specific Likelihood Ratios (SSLR) based Degree of Positivity

**HIT Positive defined as SRA positive ***HIT Negative defined as SRA negative
Stratum Specific Likelihood Ratios (SSLR) of Established versus Proposed Likelihood Ratios

**HIT Positive defined as SRA positive ***HIT Negative defined as SRA negative
The likelihood ratio served to further analyze the 4Ts score pretest probability of developing HIT against the post-test probability of LIA. The LIA threshold of 5 units/mL or greater amplifies the odds of SRA positivity whereas the LIA value stratum of 1 to 4.9 units/mL seems to display similar predictive probabilities as the 4Ts score (Table 7).

Abbreviations: HIT, heparin-induced thrombocytopenia; LIA, latex immunoturbidimetric assay; SRA, serotonin release assay.
Discussion
Existing diagnostic tools for HIT have notable limitations and are poorly studied in the CTS patient population. The 4Ts score lacks robust positive predictive probability, ELISA has diminished specificity as low as 50% contributing to high false positives, and the SRA is technically demanding with a delayed turnaround time. 17 Despite the field's advancements in understanding the interplay between HIT pathogenesis and modifications of conventional assays, the detrimental impacts of HIT as a hypercoagulable disorder continue to demand tests with increased accuracy and speed. The LIA offers an attempt to address both these attributes providing rapid sensitivity and specificity of 97.4% and 94%, respectively, at a LIA cutoff of ≥ 1 unit/mL when compared to both IgG and poly-specific ELISA. Though the probability of HIT positive was also observed to increase with rising LIA thresholds, this seminal work by Warkentin et al included a mixed cohort of medical and surgical patients. 12
To date, no studies have formally validated or established a true semiquantitative correlation between LIA values and SRA positivity exclusively in cardiothoracic surgery. The expanding use of mechanical circulatory support, elevated hemostatic instability, and scarce cardiothoracic demographic representation in HIT diagnostic validation studies prompted us to investigate if the LIA's performance translated specifically to cardiothoracic patients. We sought to determine if a semiquantitative correlation between rising LIA values and SRA positivity exists and if a more suitable LIA threshold for positivity is feasible.
Historical precedent for increasing thresholds of positivity to optimize diagnostics has been researched in ELISA literature as well. To improve specificity, several studies sought to investigate the relationship of higher optical density (OD) thresholds without compromising sensitivity. Warkentin et al 15 were able to observe a relationship between rising ELISA OD thresholds and the odds of a positive SRA. In this study, the odds of a positive SRA increased 6.39 times for every increase of 0.5 OD units (P < .0001). Raschke et al identified an ELISA OD of 0.8 units/mL to be the most discriminant single cutoff by ELISA for the diagnosis of HIT rather than 0.4 units/mL and reduced false positive rates from 31% to 6%. These datasets and the predictive values, however, were not exclusive to cardiothoracic patients. 17 In response to these clinical challenges and paucity in data, Kataria et al investigated the application of ELISA OD thresholds and the SRA results in patients on ECMO. Outcomes from this retrospective study showed that a higher ELISA OD threshold of 1 unit/mL resulted in an improved specificity (89%) while preserving the negative predictive value. 16
Overall, our study in cardiothoracic patients demonstrates that the current LIA cutoff for positivity of ≥ 1 unit/mL in CTS patients is highly sensitive at 93.8%, similar to findings from Warkentin et al. 12 However, specificity is lacking yielding an elevated false positivity rate of 76% in our cohort. By proposing a new LIA cutoff for positivity of 4.5 units/mL, specificity increased from 24% to 71%, therefore, decreasing false positivity rates by 62%. In aggregate, the AUROC of the LIA at the new proposed cutoff of 4.5 units/mL was 0.75 (95% CI 0.615 - 0.88; P = .01) indicating an overall good performance of this screening test for the evaluation of HIT in CTS patients.
SSLR offer an additional perspective into the performance characteristics of the LIA. The SSLR serves to measure the odds a patient has a true positive result within prespecified weak, moderate, and high positivity LIA thresholds. In other words, it allows providers to put into context what the odds of true HIT may be based on the LIA value. Though limited by our total sample size, the SSLR data offers a signal for semiquantitative relationship between rising LIA levels and SRA positivity. A LIA threshold of 4.5 units/mL or higher augments the likelihood of diagnosing true HIT over 2-fold compared to the established threshold of 1 unit/mL. Additionally, SSLR data was used to describe post-test probabilities of the LIA as compared to the 4Ts score. The 4Ts score is the most widely endorsed clinical assessment tool for HIT. Though alternative scores using CT surgical-specific parameters have been proposed, predictive performance in CTS have been inconsistent. Warkentin et al 12 and Linkins et al 18 have proposed 4Ts score pretest probabilities listed in Table 7. Using Bayesian analysis, we observed that weak positive LIA thresholds between 1 and 4.9 units/mL display a similar pretest and post-test probability performance relative to the 4Ts score. Post-test probabilities of true HIT diagnoses are enhanced at moderate to high positivity LIA thresholds despite low 4Ts scores. Though a low 4Ts score is noted to have a high negative predictive value, moderate to high LIA levels enhanced the probability of detecting true HIT approximately 3-fold despite a low 4Ts score.
This study provides data to support a higher LIA threshold of 4.5 units/mL in CTS patients for the evaluation of HIT. Application of this new LIA value cutoff would observe a decrease in false positive rates from 65 to 24 patients. As a result, unwarranted initiation of inappropriate anticoagulation would also decrease by 61.8%. However, it is important to note that sensitivity is not preserved by increasing the LIA threshold beyond 1 unit/mL.
Aligning with previous ELISA OD threshold studies, the implications of our results suggest that elevating the LIA threshold for positivity may enhance specificity. Though hypothesis generating, the clinical applications of our observations are several fold. Improved specificity along with decreased false positives has the potential to minimize exposure to irreversible and unwarranted anticoagulation, bleeding sequelae, hospital length of stay, and overall healthcare costs. It is noteworthy, however, to highlight the dilutional effect on sensitivity with a proposed increase in LIA threshold to 4.5 units/mL and should be further evaluated in larger studies.
Identifying HIT as a cause of thrombocytopenia in CTS patients, though essential, often leads to overdiagnosis. In fact, early onset thrombocytopenia alone is sometimes a trigger to initiate alternative, nonheparin-based anticoagulants empirically despite the low probability of true HIT associated with early-onset thrombocytopenia in CTS. 19 The findings of this study differ from previously published reports regarding HIT diagnostics. Specifically, this analysis focused exclusively on LIA's performance characteristics in cardiothoracic patients of which 34% were on ECMO suggestive of a particularly critically ill cohort. The risk of thrombosis and bleeding is a delicate balance in critically ill surgical patients. Therefore, enhancing LIA's capacity to detect true HIT to reduce overdiagnosis and mitigate the use of alternative, irreversible anticoagulants in a high-risk bleeding cohort is of utmost importance.
Our study is limited by its retrospective design and small sample size. Additional limitations include the inability to evaluate the application of LIA thresholds in patients exclusively on mechanical circulatory support, confounding variables contributing to bleeding events, and the absent collection of venous thromboembolism events for the diagnosis of HIT. Finally, it is worth noting that the results in Table 5 are counterintuitive. Based on the 4Ts high negative predictive value, one would assume that the low 4Ts score cohort would have more negative LIA values (< 1 unit/mL), for instance. 20 This counterintuitive outcome may be due to the retrospective nature of this trial. Specifically, given that 4Ts scoring was not always prospectively conducted at our institution, components of the 4Ts score may not have been documented or captured. Furthermore, isolated thrombocytopenia was frequently a trigger to send for LIA testing. These factors combined may have created the observed imbalance. In fact, retrospective 4Ts scoring is a cited limitation as noted by Crowther et al. 21 This group noted discrepant scoring between real-time scoring as compared to central adjudication. Crowther et al further concluded that the validity of low 4Ts score to definitively rule out HIT in critically ill patients may not be sufficient. These observations parallel, at least in part, to our study's observations.
Conclusion
This study is the first to evaluate the semiquantitative relationship between increasing LIA values beyond the current positivity threshold and its correlation to positive SRA results in CTS patients. Our results suggest that a higher LIA cutoff of 4.5 units/mL may improve specificity, therefore, decreasing false positives by 62%. The implications of this study have the potential to minimize bleeding events and better guide the use of irreversible anticoagulants.
Footnotes
Glossary of Abbreviations
Authors’ Note
All authors contributed to concept and design, analysis and/or interpretation of data; critical writing or revising the intellectual content; and final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.