
Abstract
Background:
The diagnosis of heparin-induced thrombocytopenia (HIT) may be challenging in critically ill patients, as heparin exposures are ubiquitous, and thrombocytopenia is common. Unwarranted ordering and incorrect interpretation of heparin antibody tests can expose a patient to adverse drug events and imposes a significant economic burden on our health care system.
Methods:
A prospective, observational study was performed over 4 months on all adult patients located in 5 intensive care units, with a heparin antibody test ordered.
Results:
A platelet factor 4/heparin enzyme-linked immunosorbent assay (ELISA) test was ordered in 131 patients. In total, 110 patients had a low 4Ts score (0-3), and of these 103 had a negative ELISA result. In patients with a low 4Ts score, 0 (0%) of 110 had an optical density value >1.0. One hundred twenty-nine patients (98%) had another possible cause of thrombocytopenia identified.
Conclusion:
In critically ill patients, low 4Ts scores indicate a low probability of HIT, and heparin antibody testing in these patients is not useful.
Introduction
Heparin-induced thrombocytopenia (HIT) is a serious, immune-mediated reaction that may occur in individuals receiving any dose or form of a heparin agent.1–3 Although, HIT occurs most commonly (1%-5%) with the unfractionated form of heparin (UFH), it has been reported to occur in 0.5% of patients receiving a low-molecular-weight heparin (LMWH) such as enoxaparin or dalteparin.3–5 Heparin-induced thrombocytopenia commonly presents with a drop in platelet count occurring on the 5th day of therapy with a heparin agent, with or without the presence of thrombosis.1,3 Heparin-induced thrombocytopenia induces a prothrombotic state characterized by intense activation of platelets, by platelet factor 4–heparin complexes (PF4/heparin), and robust thrombin generation. Prompt recognition of HIT and initiation of alternative anticoagulation is fundamental in preventing adverse outcomes such as thrombosis, organ damage, and death. 6
In the intensive care unit (ICU), 23% to 58% of patients have some degree of thrombocytopenia which makes the recognition and treatment of HIT even more complex.7,8 There are often many different reasons a critically ill patient may have thrombocytopenia. Sepsis and septic shock, major surgery, intraaortic balloon pumps, and many pharmacological agents are potential causes of thrombocytopenia in the critically ill patients.3,9 Heparin antibody tests are frequently ordered in ICU patients suspected of having HIT but are associated with high rates of false positives and can be interpreted incorrectly. 10 In addition, the decision to discontinue the heparin agent and start an alternative anticoagulant, such as a direct thrombin inhibitor (DTI) can be associated with significant patient safety risks and poses a substantial economic burden on our health-care system.11,12 The appropriate recognition and diagnosis of HIT incorporates clinical scoring tools, such as the 4Ts score, the patient’s clinical picture, and the use of heparin antibody testing. 13 The 4Ts score is a clinical scoring tool used to predict the likelihood of HIT (Table 1). A score total is based on an 8-point scale, accounting for the degree of thrombocytopenia, timing of thrombocytopenia, presence of thrombosis, and alternative causes of thrombocytopenia. A score of 0 to 3 indicates a low probability of HIT, 4 to 5 intermediate probability, and 6 to 8 high probability. The 4Ts scoring system has been validated in several different acute care populations and found to have a strong negative predictive value for the presence of a positive heparin antibody test.14–16 The 4Ts score has also been studied less extensively in critically ill patients but with similar results.17,18
The 4Ts Clinical Scoring Tool.
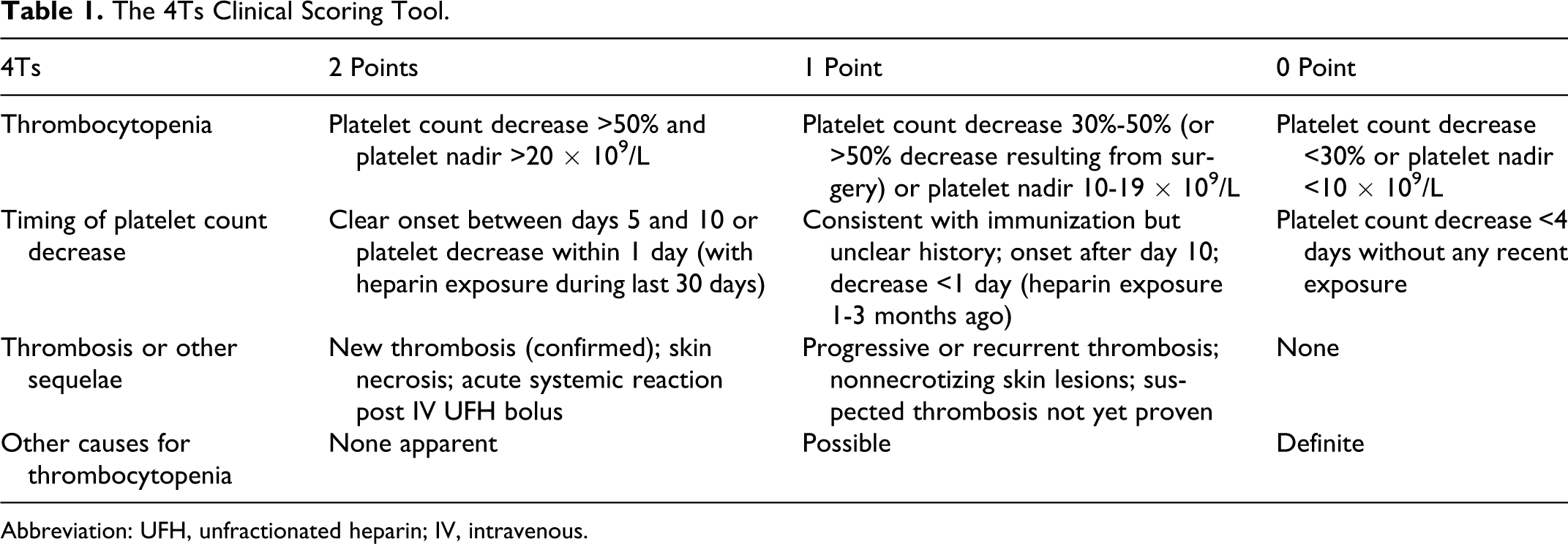
Abbreviation: UFH, unfractionated heparin; IV, intravenous.
With this knowledge, we set out with the objective to characterize the ordering of heparin antibody tests in the ICU based on a patient’s clinical picture utilizing the 4Ts clinical scoring tool. We also wanted to describe the usage of alternative anticoagulation agents and investigate potential cost avoidance associated with the correct recognition and treatment of HIT in ICU patients.
Methods
Patients and Study Design
The study was conducted at The Methodist Hospital, a 948-bed academic tertiary referral hospital located in The Texas Medical Center, Houston, Texas, and was approved by the Institutional Review Board with waiver of informed consent. The hospital has 5 ICUs: cardiovascular surgical, surgical, neurosurgical, medical, and coronary care. Prestudy analysis indicated that approximately 50 heparin antibody tests per month were ordered in the ICUs. We prospectively collected data on all adult patients admitted to any of the 5 ICUs who had a PF4/heparin ELISA test ordered between September 1, 2010 and December 31, 2010. We excluded patients who died while the heparin antibody test result was pending because the results of the antibody test were not reported for some patients once they expired. Characteristics that were recorded on each patient included age, gender, ICU location, hospital and ICU admission date, discharge date, prescribed heparin agent, and length of exposure to the heparin agent. Data were collected from the patient’s electronic medical record, paper medical chart, and pharmacy medication management system.
The heparin antibody ELISA test was ordered by either the interdisciplinary intensivist-led team caring for the patient or a consult service. At the time the heparin antibody ELISA test was ordered, the 4Ts score was calculated by the primary researcher. The heparin antibody test result was not immediately available, taking up to 72 hours to be reported. Thus, the primary researcher was blinded to the result of the PF4/heparin test while computing the 4Ts score. The primary researcher determined the patient’s 4Ts score by using information from the patient’s electronic medical record, paper medical chart, and pharmacy medication management system. Patient data such as length of therapy with heparin agent, timing of thrombocytopenia, extent of platelet drop, presence of thrombosis or skin lesions, and other possible medication or comorbid-induced causes of thrombocytopenia were evaluated. There was no active intervention in the care of the patient made by the primary researcher or study team. An attempt was made to identify the true day of heparin initiation by reviewing in-hospital documentation of all heparin exposure and records from outside facilities for those patients transferring in from other institutions.
The primary outcome of the study was to determine the number of heparin antibody tests appropriately ordered based on the patient’s 4Ts score. Appropriate was defined as a patient with a heparin antibody order who scored an intermediate (4-5) or high (6-8) 4Ts score. Inappropriate was defined as a patient with a heparin antibody order who scored a low (0-3) 4Ts score. Secondary outcomes looked at the potential cost avoidance associated with the unnecessary ordering of heparin antibodies and the initiation of alternative anticoagulation. Medications used for alternative anticoagulation were also collected.
The PF4/heparin ELISA tests (PF4 IgG Solid Phase ELISA, Gen-Probe GTI Diagnostics, Inc, Waukesha, Wisconsin) were performed in-house on a daily batch schedule, Monday through Friday. An optical density (OD) value of 0.40 or greater was reported as a positive antibody result, according to the Clinical and Laboratory Standards Institute. We performed a subgroup analysis of OD values of 1.0 or greater as a separate positive cutoff (due to the high rates of false positives with OD values less than 1.0), and the stronger serotonin-release assay (SRA) confirmation associated with OD values greater than 1.0. 19 The positive and negative predictive values of the 4Ts scoring tool were evaluated as it compared to the PF4/heparin ELISA antibody test result. Descriptive statistics were performed on the demographic, primary, and secondary outcome data. Data were summarized as mean (± standard deviation), median, and percentages.
Results
A total of 134 patients met the inclusion criteria during the enrollment period. Three patients were excluded from study analysis because they died before the PF4/heparin antibody test result was reported. The baseline characteristics of the study population are summarized in Table 2. The majority of patients were surgical patients (n = 79, 60%), with 81 (62%) PF4/heparin antibody tests ordered on patients in the cardiovascular surgery ICU. Every other ICU had at least 4 antibody tests ordered during the study period.
Baseline Characteristics of the Study Patients.
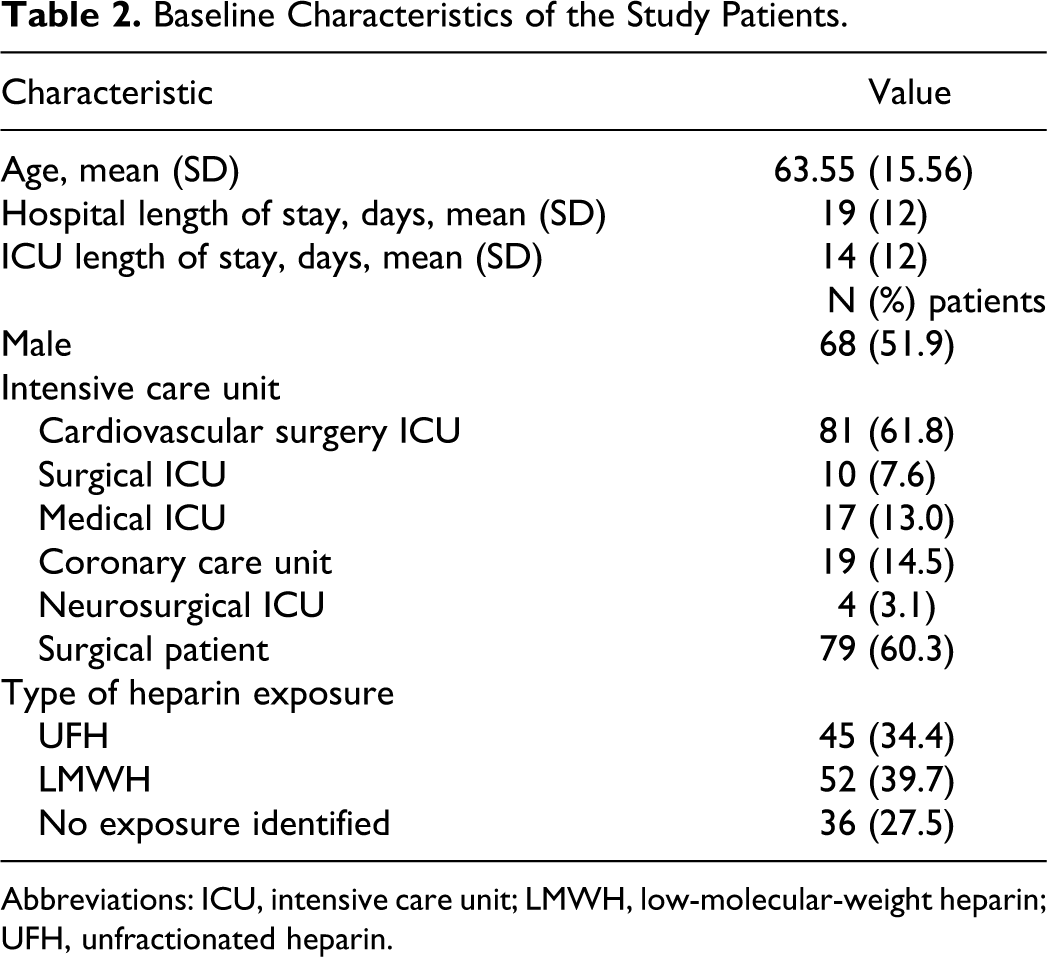
Abbreviations: ICU, intensive care unit; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin.
Thirty-six patients (28%) were not exposed to heparin or LMWH during their admission at our hospital, nor could any exposure from outside institutions be identified.
A total of 95 patients received a heparin agent, 45 with UFH and 52 with LMWH. Two patients had been exposed to both agents prior to ordering the PF4/heparin antibody test. Of the 95 patients exposed to a heparin agent, 41 (43%) had the medication discontinued at the time the heparin antibody test was ordered. Alternative nonheparin anticoagulants, including DTIs and fondaparinux were initiated in 16 patients. In all, 10 patients were initiated on fondaparinux, 4 on bivalirudin, and 2 on argatroban.
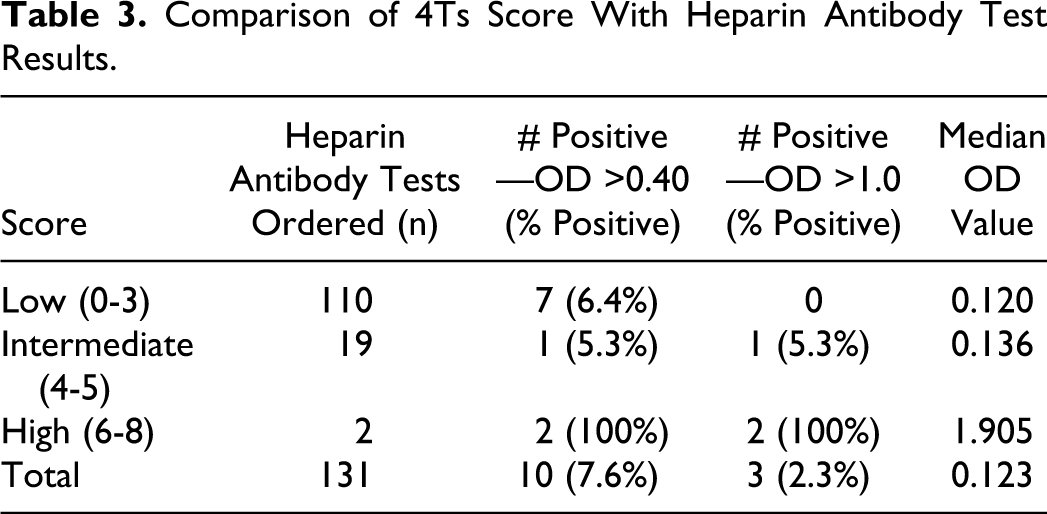
Table 3 displays the comparison of the 4Ts score with heparin antibody test results. The 4Ts score was calculated to be low in 110 (84%) patients, intermediate in 19 (15%) patients, and high in 2 (1%) patients. Of the 110 patients with a low 4Ts score, 7 (6%) had a positive OD value (OD >0.40). None of the patients with a low 4Ts score had an OD value greater than 1.0. One patient (5%) with an intermediate 4Ts score had a positive OD value of greater than 0.4. This particular patient’s OD value was 3.188 and was diagnosed with HIT by medical staff. In patients with a high 4Ts score, 2 (100%) had an OD value greater than 0.4. The median OD value of these 2 patients was 1.90, and each of them ultimately received a diagnosis of HIT by a hematologist. The 3 patients diagnosed with HIT and their treatments and outcomes are described in Table 4. The negative predictive value in patients with a low 4Ts score was 93.6%. When using an elevated OD cutoff of 1.0 for a positive antibody test value, the negative predictive value of patients with a low 4Ts score was 100%. The positive predictive value of the 4Ts scoring tool in patients with a high score was 100%.
Comparison of 4Ts Score With Heparin Antibody Test Results.
Demographics, Treatment, and Outcomes of Patients Diagnosed With HIT.a
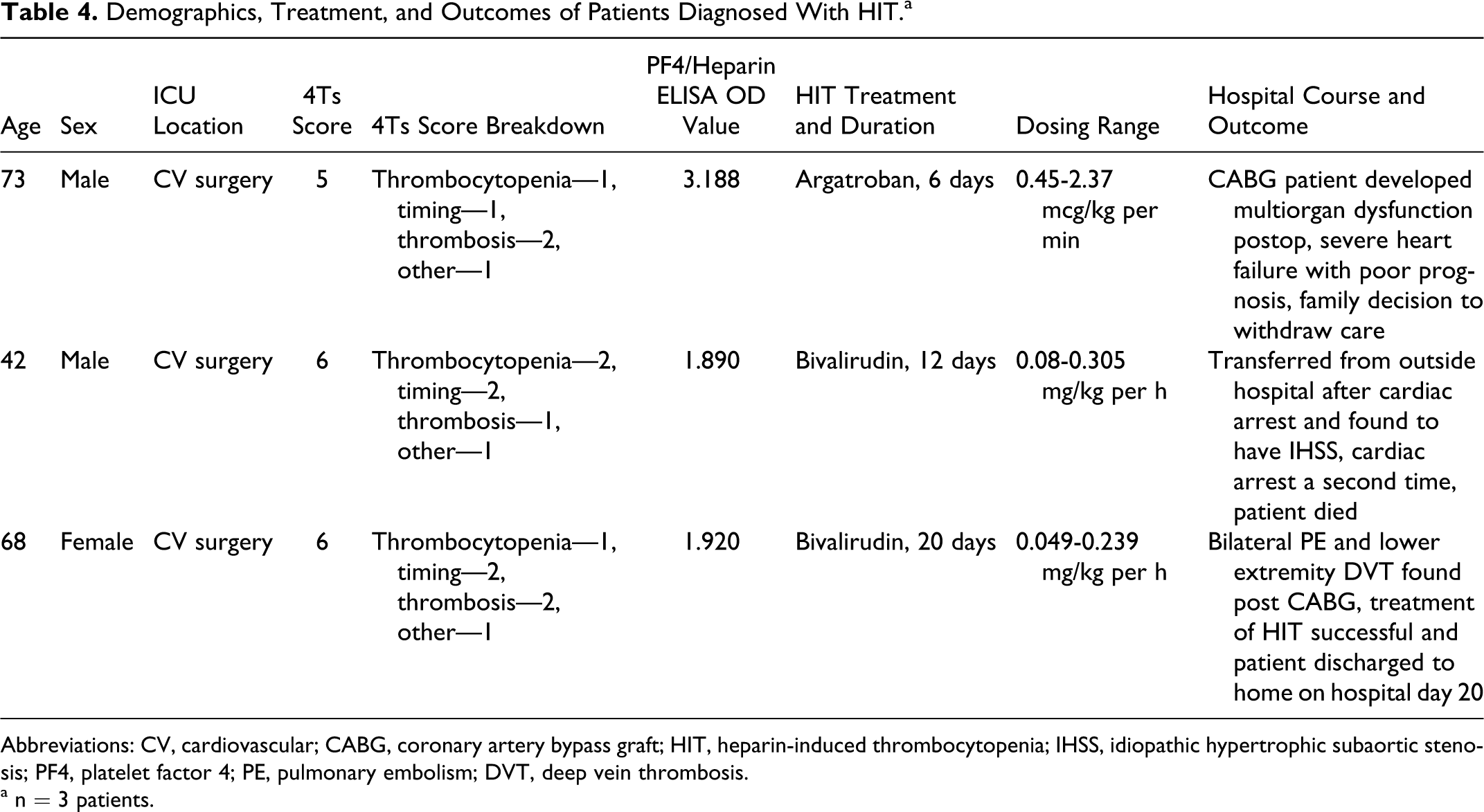
Abbreviations: CV, cardiovascular; CABG, coronary artery bypass graft; HIT, heparin-induced thrombocytopenia; IHSS, idiopathic hypertrophic subaortic stenosis; PF4, platelet factor 4; PE, pulmonary embolism; DVT, deep vein thrombosis.
a n = 3 patients.
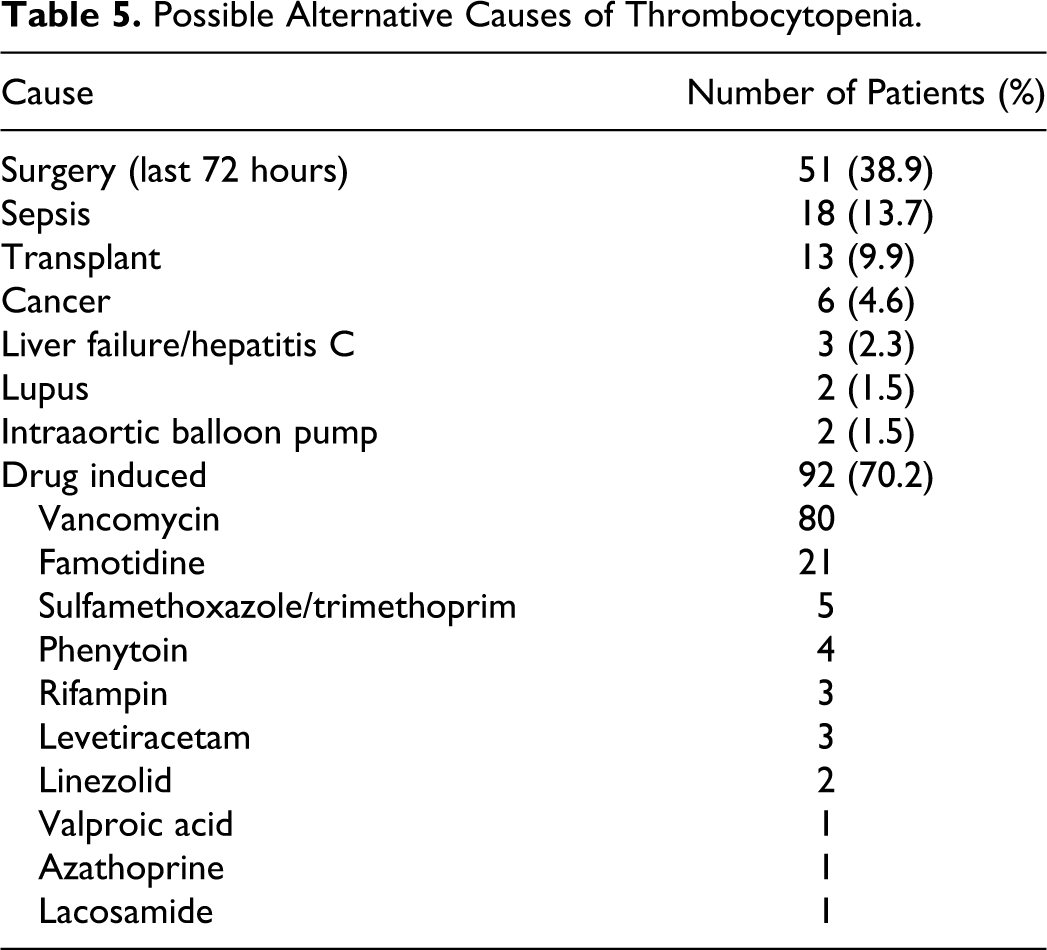
Possible alternative causes of thrombocytopenia were identified in 129 (98%) patients (Table 5). The most common alternative cause of thrombocytopenia was drug induced, with vancomycin being administered to 80 (61%) patients. Other medications such as famotidine (n = 21, 16%) and sulfamethaxazole/trimethoprim (n = 5, 4%) were frequently prescribed to the study participants. Fifty-one patients (38%) had major surgery in the last 72 hours and 18 patients (14%) had sepsis, 2 possible alternative causes that may have attributed to their thrombocytopenia.
Possible Alternative Causes of Thrombocytopenia.
Cost Avoidance
In the 110 patients with an antibody test ordered who had a low 4Ts score, a potential cost avoidance of $18 150 (United States) was calculated. 20 In 7 patients with either a low 4Ts score or an intermediate-to-high 4Ts scores and a negative antibody test, a total of 47 days of fondaparinux treatment and 4 days of bivalirudin were administered. The additional cost incurred with these treatments was found to be $23 246. Over the course of 4 months, a total potential cost avoidance of $41 396 was seen in study patients when considering cost of the heparin antibody test and medication cost with alternative anticoagulants. This cost avoidance does not include the cost associated with monitoring of DTIs or cost associated with treating adverse events from DTIs.
Discussion
The objective of this study was to characterize the ordering of PF4/heparin ELISA antibody tests in critically ill patients based on clinical suspicion. We evaluated all heparin antibody orders in the ICU over the course of 4 months to determine whether a patient’s clinical picture warranted the ordering of a heparin antibody test. Our results show that the majority of patients (110 of 131, 84%) had a low clinical suspicion of HIT based on a low 4Ts score and should not have had the laboratory test ordered. Although 7 of these patients had positive heparin antibody results with OD values between 0.4 and 1.0, none were ultimately diagnosed with HIT. The results confirm the strong negative predictive value of the 4Ts score, further validating previous data that the 4Ts score is effective in identifying critically ill patients with a low probability of HIT.17,18 In patients with a low 4Ts score, the clinician should first look to identify possible alternative causes of thrombocytopenia before ordering a heparin antibody test or initiating alternative anticoagulation.
Other causes of thrombocytopenia can often be found in critically ill patients, as evidenced by the 98% rate seen in our study patients. It is important to evaluate all other possible causes of thrombocytopenia as this is the component of the 4Ts score that is most susceptible to interrater variability. 13 The most frequent cause of thrombocytopenia seen in our patients was medication induced. Many study participants were initiated on vancomycin therapy as empiric treatment for suspected infection, which may cause thrombocytopenia (1%-8%).21,22 Famotidine was frequently administered to our study patients and its use has been associated with thrombocytopenia, although data are limited and somewhat controversial.23,24 Major recent surgery was also common in our patient population, many of whom were located in the cardiovascular surgery and surgical ICUs. When assessing for HIT it is important to take these other causes into consideration because they are so frequently seen in critically ill patients and may obscure the clinical picture.
An interesting finding was the low (43%) rate of heparin agents discontinued when the antibody test was ordered. Many patients continued to receive treatment with heparin, which may indicate that the clinician ordering the heparin antibody test had a low suspicion of HIT. It is possible that the heparin antibody tests are frequently being used to rule out HIT in patients with thrombocytopenia rather than confirm a diagnosis based on high clinical suspicion. Due to the fact that ELISA tests have a high rate of false positives, this places increased responsibility on the clinicians to correctly interpret the results to prevent unnecessary exposure to DTIs. An alternative to using the PF4/heparin antibody tests to rule out HIT may be the use of the 4Ts score itself, which has shown a strong negative predictive value in many clinical trials and in a variety of patient populations.
The choice of alternative anticoagulation options for HIT displays a relative shift from what we have seen in previous years. Our institution has pharmacy-driven protocols for managing argatroban and bivalirudin, and other patient-specific factors such as renal or hepatic insufficiency may have attributed to the choice of one DTI over another. From the previous 12 months, 68% of patients started on a DTI for HIT were initiated on argatroban compared to only 32% of patients initiated on bivalirudin. This represents a change in DTI treatment choice compared to our study where 67% of patients were initiated on bivalirudin and 33% of patients on argatroban.
Significant cost avoidance can be appreciated from the correct evaluation, recognition, and treatment of patients with HIT. 11 Significant cost can be attributed to the unwarranted ordering of heparin antibody test, however the majority of cost can be credited to the unnecessary or inappropriate initiation and monitoring of agents such as bivalirudin, argatroban, and other nonheparin anticoagulants. The initiation of these agents is extremely costly to the health care system, when taking into account the acquisition cost of the medication, nursing monitoring and care, pharmacy monitored dosing protocols, and treatment of side effects and adverse events. A study published in 2006 described the incremental average cost of treating a patient with HIT to be 41 000 USD. 11 At our institution, the cost avoidance from this study extrapolated over the course of 12 months is over 120 000 USD for critical care patients alone, not taking into account acute care patients. The number of heparin antibody tests ordered in the ICU and acute care floors at our hospital is very similar on a monthly basis. We anticipated 200 patients enrolled in the study prior to data collection, and only enrolled 131 so cost avoidance may be underestimated due to a less than expected enrollment. We also anticipate cost avoidance to be significantly higher when taking into account drug and laboratory monitoring costs.
This study methodology has limitations that should be discussed. First, the largest limitation to the study was that none of the patients had a follow-up SRA to confirm their diagnosis of HIT. While the SRA has shown to have stronger predictive value than the PF4/heparin ELISA test and is used for confirmation of PF4/heparin ELISA tests, it is a send-out laboratory test with a long turnaround time. Instead, the diagnosis of HIT by a trained hematologist was used as the gold standard in patients with a positive OD result at our institution. Another limitation was that a single researcher was responsible for calculating the 4Ts score. The 4Ts score has been validated in many populations over time but can be subjective and open to interrater variability. Although having a single person calculating the 4Ts score increased the internal validity of the study, it may compromise our external validity and extrapolation of our results. Another limitation was the lack of information regarding heparin exposure from outside institutions. Since our study hospital is a large, tertiary care center with many transfers from outside institutions, we were aware of the possible high rate of recent heparin exposure at outside institutions with no available documentation. A total of 37 patients had no documented or charged heparin exposure at our hospital or an outside institution. In addition, since there was no active intervention or involvement in care by the research team, we were unaware of patient information that was conveyed to members of the patients' medical team but not documented in the patients chart or medical record.
Conclusion
Our study found the 4Ts score to have a strong negative predictive value for assessing the probability of HIT in critically ill patients. When using an elevated OD cutoff of 1.0, the negative predictive value of patients with a low 4Ts score was 100%. The 4Ts scoring tool should be used as an initial method of evaluating critically ill patients with thrombocytopenia following exposure to heparin or LMWH. In patients with a low 4Ts score, alternative causes of thrombocytopenia should be evaluated as they are frequently present. Patients with a low 4Ts score generally do not warrant the routine ordering of a heparin antibody or initiating alternative anticoagulation.
Footnotes
Acknowledgment
Lawrence Rice serves as a consultant to Canyon Pharmaceuticals® and is on the speaker’s bureau for GlaxoSmithKline®.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.