
Abstract
Background
Dipeptidyl peptidase 3 (DPP-3) is an intracellular enzyme that causes hemodynamic instability and cardiac depression in several cases such as cardiogenic shock, sepsis and burns where DPP-3 is released into the blood due to cell death. Data on the effect of higher DPP-3 levels on acute coronary syndrome (ACS) patients are currently lacking. The aim of this study was to evaluate the effect of DPP-3 levels on ACS patients.
Methods
In this prospective study, we included ACS patients including STEMI and non-STEMI groups and a control group to compare various demographic, echocardiographic and laboratory parameters including DPP-3. DPP-3 levels were measured at 24th, 48th, and 72nd h from the onset of symptoms in ACS patients and then compared with left ventricle ejection fraction (LVEF) for the assessment of left ventricle systolic function.
Results
A total of 70 ACS patients (age 62.5 ± 11 years, 68.6% male) were recruited and 48 normal individuals were included as control group (age 61.1 ± 10 years, 66.7% male). It has been demonstrated that DPP-3 levels are significantly higher in the ACS group than the control group like troponin I levels. DPP-3 levels were found to be one of the independent predictors of LVEF similar to NT-proBNP and troponin I.
Conclusions
This study suggests that DPP-3 could be an important indicator of myocardial depression predicting left ventricle systolic function in ACS.
Introduction
Acute coronary syndrome (ACS) is a common cause of hospitalizations worldwide and biomarkers have become essential for ACS diagnosis, risk stratification and prognosis of cardiovascular disease. 1 ACS term is used for a spectrum of conditions consistent with acute myocardial ischemia and/or infarction that are mostly related to an abrupt reduction in coronary blood flow. ACSs have numerous clinical presentation scenarios ranging from patients with cardiac arrest, electrical or hemodynamic instability with cardiogenic shock, to patients who are pain free at admission. 2 Even if appropriate and timely revascularization is achieved in some patients with ACS, myocardial damage and development of heart failure cannot be prevented. Therefore, new markers are required to understand the clinical process and etiology of the disease.
From a chemical point of view, dipeptidil peptidase (DPP-3) is an endogenous, cytosolic zinc-dependent enzyme that is involved in the degradation of numerous cardiovascular mediators 3 and digests some bioactive peptides such as angiotensins, enkephalins, and endorphins.4,5 Although a relationship between serum DPP-3 and other cardiac diseases has been shown before, the role of DPP-3 in ACS has not been clearly established yet. 6 Blood pressure regulation, inflammation, and pain modulation are some of the important roles of DPP-3 which are already proven. 3 During the last few years, a new disease mechanism causing short-term organ damage has been identified and it has been shown that the release of DPP-3 plays a pivotal role in deterioration of cardiac function.3,7 In massive cell death conditions such as major surgeries, cardiogenic shock, burns, or sepsis; DPP-3 acts like a toxin-like molecule and inactivates some hormones such as angiotensin II that has a critical role in the cardiac function and cardiac depression and hemodynamic worsening develop as an inevitable result at the end.8–10 High DPP-3 blood levels have been shown to worsen patient's status which can cause to short-term organ failure and death whereas low DPP-3 levels demonstrate a reduced mortality risk.3,7
With this study, we sought the role of serum DPP-3 levels in patients with ACS and investigated whether it has a role in the course of myocardial reserve and left ventricular function.
Methods
Our study was a single center, prospective observational study. Local ethic approval was obtained from Mersin University Ethics Committee numbered 2020/16. 70 acute coronary syndrome (S- elevation myocardial infarction (MI) and Non-ST elevation MI) patients, aged 18–90 years, and 48 patients with chronic coronary syndrome as control group was included in the study. The number of patients was determined by statistical power analysis. Eligible patients were required not to have a previous history of heart failure, chronic renal failure, and chronic liver failure. Additional to these inclusion criteria, percutaneous coronary intervention due to stable angina pectoris and unstable angina pectoris, active infection, and a history of malignancy made up the exclusion criteria of the study. The demographic characteristics of the patients, previous medical history, and the drugs they had been using were recorded at the first admission.
Blood samples were taken from the patients at 24th, 48th, and 72nd h from the onset of symptoms, and the blood was centrifuged to separate the serum and stored at −20°C. All blood was sent by cold chain to Mersin University Faculty of Medicine, Department of Biochemistry, and the experimental procedures were entirely performed in this unit. DPP-3 levels were measured with the Human DPP-3/Elisa kit (USCN, China) and Troponin I levels were measured with the Human Troponin I (TNI) Elisa kit (USCN, China) in the serum of the patients at the 24th, 48th, and 72nd h. Human N terminal brain natriuretic peptide (NT-ProBNP) Elisa kit and NTproBNP (USCN, China) measurements were made in the serum of the patients at 72nd h, in accordance with the manufacturer's instructions. All patients’ routine laboaratory parameters, NT-ProBNP and troponin levels were checked and rotine transthoracic echocardiograpy was performed on each individual at admission. Heart rate and blood pressure and Killip of each patient were recorded.
Statistical Analysis
Categorical values are presented as number of patients. Normally distributed values are presented as mean ± standard deviation, non-normally distributed values are presented as median (range). The Kolmogorov–Smirnov test for continuous variables was used to evaluate the normal distribution. While Student's t-test was used to evaluate differences in the parametric variables, Mann–Whitney U test was used nonparametric groups. Categorical variables were compared using the chi-square test. Correlation analysis was performed using the Wilcoxon correlation method. Multiple linear regression analysis was used to study the predictive factors for left ventricular ejection fraction. Statistical analysis of these parameters was performed with SPSS (Windows, version 22.0, SPSS Inc., Chicago, IL, USA). Analysis results were evaluated within a 95% confidence interval, and P < .05 was interpreted as a statistically significant difference.
Results
We recruited 118 patients (70 MI patients vs. 48 control patients) in this study. The two patient groups were well-balanced with respect to baseline characteristics (Table 1). There was no significant difference in terms of age between groups and gender distribution was also similar in both groups (Table 1). 34% of the patients were STEMI, while 66% of them were non-STEMI. Heart rate and diastolic blood pressure of the patients showed a significant difference between two groups, whereas average systolic blood pressure showed a similar value. Killip Score was assessed in the MI group itself and 60% of the patients (n = 42) were presented with Killip 1, 35.7% of them (n = 25) were presented with Killip 2, and 4.3 of the patients (n = 3) were presented with Killip 3, while there was no patient presented with Killip IV. Among laboratory tests, only the low-density lipoprotein (LDL) level was significantly higher in the MI group than control group whereas other parameters showed no significant difference. Mean left ventricular ejection fraction (EF) was significantly higher in MI group than that of control group. From cardiac biomarkers; NT-proBNP, troponin I, and DPP-3 levels showed significant difference between two groups, and average DPP-3 level was 28.2 ng/mL in MI group, whereas it was 18.6 in the control group (P < .001).
Baseline Demographic, Biochemical, Echocardiographic and Clinical Features of Patients with Myocardial Infarction and Healthy Subjects.
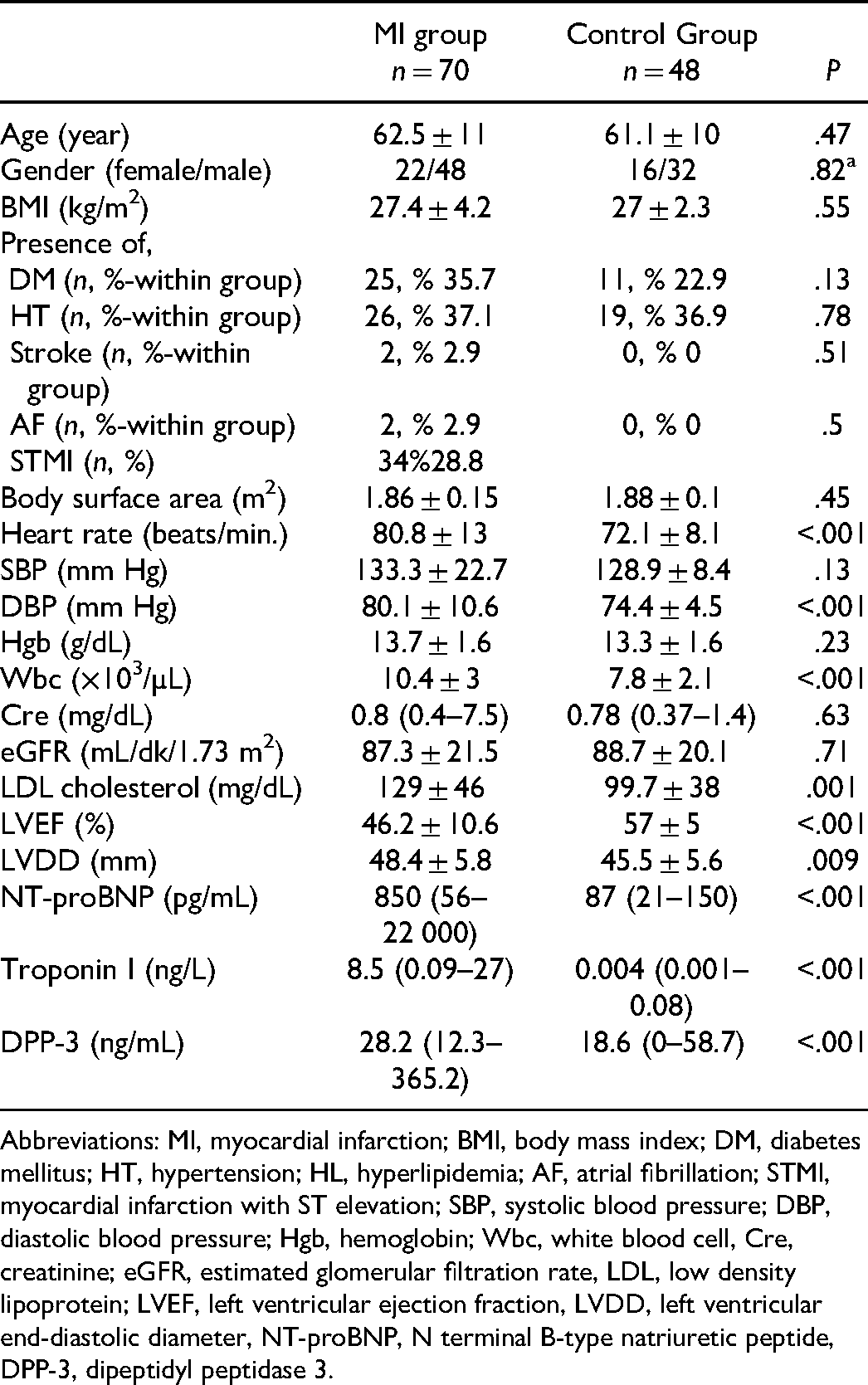
Abbreviations: MI, myocardial infarction; BMI, body mass index; DM, diabetes mellitus; HT, hypertension; HL, hyperlipidemia; AF, atrial fibrillation; STMI, myocardial infarction with ST elevation; SBP, systolic blood pressure; DBP, diastolic blood pressure; Hgb, hemoglobin; Wbc, white blood cell, Cre, creatinine; eGFR, estimated glomerular filtration rate, LDL, low density lipoprotein; LVEF, left ventricular ejection fraction, LVDD, left ventricular end-diastolic diameter, NT-proBNP, N terminal B-type natriuretic peptide, DPP-3, dipeptidyl peptidase 3.
DPP-3 level revealed a significant difference between 48th and 72nd h, as well as between 24th and 72nd levels. On the other hand, there was no significant difference between 24th and 48th h; whereas troponin levels were significantly different in all these time comparison groups (Table 2).
Comparison of Parameters at 24, 48, and 72 h in MI Group.

comparison of 24th h versus 48th h parameters.
comparison of 48th h versus 72nd h parameters.
comparison of 24th h versus 72nd h parameters.
The independence of multiple correlations was assessed using multiple linear regression analysis. In the model, troponin I, NT-proBNP, DPP-3, heart rate, body mass index (BMI), and Wbc levels were used as independent variables, and EF was used as the dependent variable. According to this analysis, DPP-3 level was found to be independent predictors of EF similar to NT-proBNP and troponin I, whereas white blood cell (WBC), heart rate (HR), and BMI were not (Table 3).
Multiple Linear Regression Analysis of the Predictive Factors for Left Ventricular EF (Adjusted r2 = 0.38) After MI.
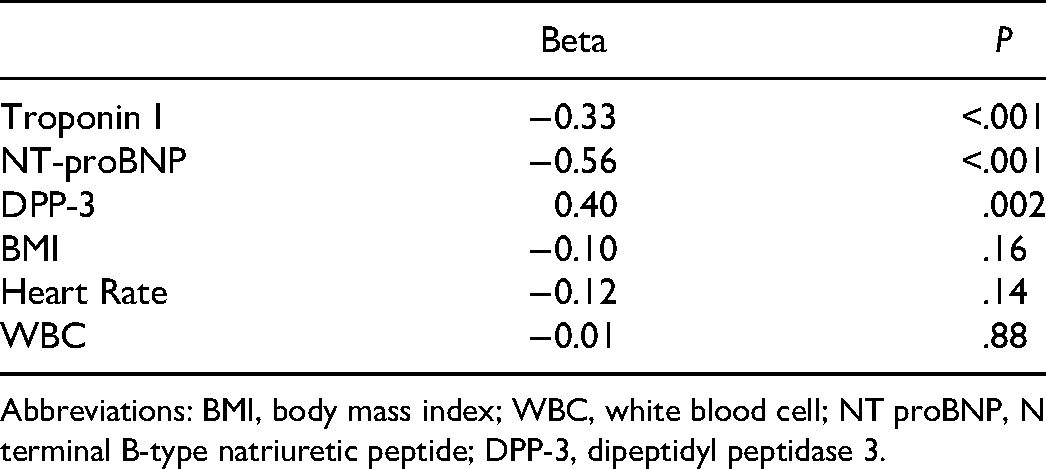
Abbreviations: BMI, body mass index; WBC, white blood cell; NT proBNP, N terminal B-type natriuretic peptide; DPP-3, dipeptidyl peptidase 3.
Discussion
To the best of our knowledge, this is the first study in the literature that demonstrates the association between DPP-3 level and myocardial injury after ACS which may also help to create a new risk assessment system in the setting of ACS and an advanced understanding of the role of DPP-3 in this patient group may offer new therapeutic treatment options in the near future.
Dipeptidil peptidades have crucial roles in different mechanisms such as oxidative stress defense, protein maturation and degradation, bioactive peptides processing and degradation, and cell cycle regulation.11,12 DPP-3 is given this name as it was the third discovered protein from this family and shown to be related with several critical physiological and pathological pathways in mammals.13,14 Yet, these pathopyhsiological mechanisms in the heart are not very well-defined.
There are already some studies in the literature that showed that the low levels of DPP-3 in healthy humans increase dramatically under several important acute conditions such as septic, cardiogenic, and vasodilatory shock. 15 It has been also demonstrated that higher DPP-3 levels are related to mortality in patients with cardiogenic shock and intravenous DPP-3 administration results in a fast negative inotropic action in healthy mice and the inhibition of DPP-3 by procuzimab (PCZ) restored the worsened cardiac detorieration during sepsis in rats. According to this study, PCZ dramatically restored left ventricle ejection fraction (LVEF) from 39% ± 4% to 51% ± 2% within only 30 min of PCZ initiation. 16 However, there is no previous study in the literature regarding the worsening effect of DPP-3 on heart in the particular setting of acute coronary syndrome. In accordance with the literature, our data provided strong evidence of the pivotal role for DPP-3 in the pathophysiological pathway of acute coronary syndrome-related cardiac depression. Our prospective study demonstrated that DPP-3, an intracellular enzyme, is a crucial factor plasma levels of which are significantly higher in the MI group than in the control group similar to troponin level which is already proven to get increased during cardiac injury conditions. One of the findings of our study was regarding its course and there was no significant difference between 24th and 48th h of ACS; whereas there was a significant difference between 24th and 72nd h, and 48th and 72nd h of ACS which proves that the level of DPP-3 gets significantly higher after the 48th h of acute coronary syndrome.
A very important result of the study was that DPP-3 was a predictive factor for EF similar to troponin and NT-proBNP. As DPP-3 affects the distribution of angiotensin peptides in the RAS, it indicates a crucial role in the regulation of this system that was emphasized in a series of reports which defined DPP-3 as a risk factor in several acute medical conditions such as heart failure, septic shock, and kidney failure and all these emergent roles indicate DPP-3 as a predictive parameter for the evaluation of short term outcome particularly on the left ventricle systolic function, for the risk stratification, for the prognostic improvement and treatment guidance and on the basis of all these a potential new target might be the development of specific inhibitors of DPP-3 to decrease DPP-3 levels to protect heart from its depressant effects.
Of course, these results of our study will need further confirmation in other studies in order to establish the role of DPP-3 in ACS patients. A limitation of our study is the relatively small number of our sample population. However, this study is a prospective study and it includes three important cardiac markers ‘DPP-3, troponin I and BNP’ levels which were measured in determined consecutive time points (24th, 48th, and 72nd h) and compared with each other and with other parameters precisely.
Conclusion
This study suggests that DPP-3 could be a potential myocardial worsening factor in ACS patients similar to the conditions like cardiogenic shock and further randomized controlled trials are required to add DPP-3 as a new indicator of myocardial depression as a supportive test to troponin I and NT-proBNP levels. DPP-3 might be a good predictor for left ventricle systolic dysfunction after ACS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.