
Abstract
Objective
Our objective in this study was to determine the predictive factors of thromboembolic complications in patients with previous heart disease and severe covid-19 infection and the impact of previous use of antithrombotics on protection against these complications.
Methods
We conducted a single-center retrospective study of 158 patients with heart disease admitted to an intensive care unit for severe SARS-COV-2 infection. In order to determine the predictive factors, we used logistic regression analysis.
Results
Out of 158 patients, 22 were complicated by a thrombo-embolic event (13.9%), mean age of our population 64.03 (SD = 15.27), with a male predominance of 98 (62%). For the predictive factors of thromboembolic complications, and after multivariate analysis, we find the short duration of hospitalization (OR = 0.92; 95%CI (0.863–0.983), P = .014, previous use of antithrombotic drugs ((OR = 0.288, 95%CI (0.091–0.911), P = .034 for antiplatelet agents) and (OR = 0.322, 95% CI (0, 131–0.851), P = .021) for anticoagulants) as protective factors, and admission thrombocytosis as a risk factor (OR = 4.58, 95%CI (1.2–10.627), P = .021). D-dimer was not detected as a risk factor, and this can be explained by the characteristics of our population. Although prior use of antithrombotic drugs protects against thromboembolic complications during severe infection, there was no benefit in mortality.
Conclusion
Prior use of antithrombotic drugs is a protective factor against thromboembolic complications in patients with a history of heart disease but without effect on mortality.
Keywords
Introduction
Shortly after the declaration of COVID-19 infection as a worldwide pandemic, 1 Although COVID-19 and influenza virus are clinically similar, 2 it was shown that it is not only an infection that affects the airways, but it is a multifaceted general disease with a very high thromboembolic risk, 3 therefore, the management and thus the prevention of thromboembolic events 4 of the disease remains a real challenge for physicians. 5 Coagulopathy during COVID-19 infection affects both the microcirculation and the macrocirculation, 6 and this coagulopathy can be explained by the inflammatory storm secondary to storm cytokines 7 on the one hand, and the elevated secretion of the following pro-inflammatory mediators: Interleukin −6, Interlukine-17 A, and Tumor necrosis factors alpha, 8 which will result in hyperactivation, and thus a high secretion of tissue flacteur and as consequences a major activation of coagulation, 9 this converges with a concomitant increase of inflammation markers in both situations, ie COVID-19 10 or Thrombo-embolic events. 11 Another parameter not to be forgotten in the generation of this thrombotic state is platelet activation. 12
A rather special population that has posed a real problem of therapeutic management is patients with underlying heart disease, given the impact of the treatments used on the cardiovascular system, 13 and thus on the evolution of the disease, since it has been shown that the presence of underlying heart disease represents a factor of poor prognosis of the disease. 14 Regarding thromboembolic complications, several series found that patients with a history of heart disease, are more likely to develop these complications with a higher intra-hospital mortality, 15 and with a more difficult management given the hemorrhagic risk that is generally high in this population on the one hand, and the associated co-morbidities that make the pharmacological environment too loaded and with a higher risk of interaction. 16 In this cohort, we tried to know the predictive factors of thromboembolic events in patients with heart disease admitted for a severe form of COVID-19 disease, and thus to know the impact of the previous use of antithrombotic drugs of all classes on these complications.
Materials and Methods
Study Setting
The COVID-19 pandemic has disrupted the daily life of medical and paramedical staff as well as hospital activity in the intensive care unit. In our hospital, the intensive care unit (ICU) has played an essential role in the management of patients with severe SARS-COV-2 infection in continuous collaboration with cardiologists, radiologists and biologists.
The criteria for admission to the ICU are defined as follows
A) A patient with proven or probable COVID-19 infection with only one of the following criteria;
RF greater than 30cpm Hemodynamic instability Disturbance of consciousness Severe comorbidity such as heart failure and coronary artery disease. SpO2 less than 90%.
All hospitalized patients underwent thoracic imaging, arterial gasometry and a biological workup on admission, followed by multi-day monitoring of clinical status, and thus possible complications mainly thrombo-embolic events.
Type and Objectives of the Study
Our objective is to determine the predictive factors of thromboembolic complications of all types (pulmonary embolism, myocardial infarction, acute ischemia of the limbs, deep vein thrombosis, ischemic stroke) in patients with cardiac disease and hospitalized for serum COVID-19 infection and thus to know the impact of the early use of antithrombotic drugs of all classes on these thromboembolic events. For this purpose, we conducted a mono-centric retrospective study on patients admitted to the intensive care unit of the CHU Mohammed VI of OUJDA, over a period between March 2020 and March 2022.
Inclusion Criteria
Patients included in the study are: All patients admitted to the intensive care unit of CHU MOHAMMED VI OUJDA with a positive RT-PCR for COVID-19 or with chest imaging suggestive of COVID-19 infection and who are being followed for heart disease. The patients were divided into two groups: Group A, those who were previously taking antithrombotic drugs, and Group B, those who were not (Figure 1).

General scheme of our study as well as the patients included.
Data Collection
Medical information was collected between March 2020 and March 2022 by the medical staff of the unit and stored in the medical observations database used at CHU MOHAMMED VI OUJDA. For each patient, the collection took into account demographic information (sex, age). The medical and surgical history, anamnestic data concerning the infection including the duration of symptoms, the duration between the beginning of symptoms and the consultation, the symptoms of the COVID-19 infection, biological and imaging data, the treatment used during the hospitalization, and then the evolution with regard to the complications presented and mortality.
Statistical Analysis
The objective of the study was to determine the predictive factors of thromboembolic complications in patients hospitalized in our intensive care unit for severe COVID-19 infection and who are known to have heart disease, and thus to know the impact of the previous use of antithrombotics on these events and the intra-hospital evolution.
For this purpose, we divided our population into two groups: group of patients who presented a thromboembolic complication and group of patients who did not present these events. The data were collected and processed with IBM SPSS statistics 26.0 statistical software. Normally distributed quantitative variables were described as mean and standard deviation, and analyzed between the two groups by the t-student test. Non-normally distributed quantitative variables were described as median and interquartile range, and analyzed by nonparametric tests. Categorical variables were described in numbers, and analysis between the two groups was done by Pearson's chi-square test or Fisher's exact test. Anonymity and confidentiality were respected in all stages of data processing.
To determine the predictors of thromboembolic complications, a statistical analysis of multivariate logistic regression was applied. First, a univariate approach was performed for all covariates, and then a multivariate analysis was performed for all covariates that showed statistical significance in the univariate analysis. To estimate the probability of developing a thromboembolic event during hospitalization, Kaplan-Meier curves were used and compared between co-variables using log-rank tests. The associated 95% confidence interval (CI) and 2-sided p value were reported. For all statistical tests, a p value less than 0.05 was considered statistically significant.
Ethical Approval
This study does not require formal ethics committee approval. Access to patient data was authorized by Mohammed VI University Hospital and approved by the head of department, given the retrospective design of this study. The requirement for patient consent was waived. Data anonymity was respected in accordance with national and international guidelines.
Results
General Presentation
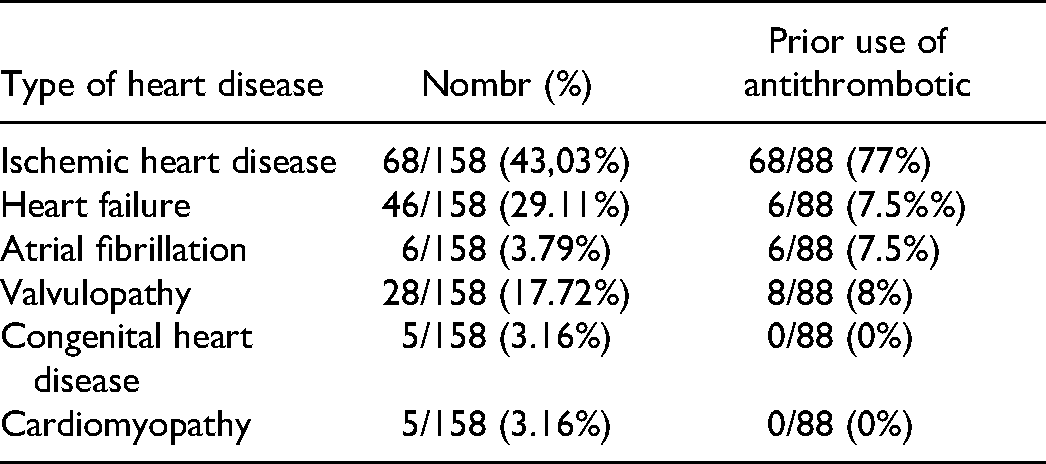
In 1115 patients admitted to intensive care units for severe covid-19 disease, 158 had heart disease, ischemic heart disease in 68 patients (43.3%), heart failure in 46 patients (29.11%), atrial fibrillation in 6 patients (3.79%), 28 patients had valve disease (17.72%), and finally cardiomyopathy and congenital heart disease in 10 patients, 5 in each (3.16%). The number of patients who were already taking an antithrombotic drug was 88 (Table 1).
Types of Heart Disease in our Patients.
To approach our analysis, we divided our patients into two groups: Group A: patients who presented a thromboembolic complication and Group B: patients who did not present this complication.
Demographic, Anamnestic and Medical-Surgical Characteristics
Our study included 158 patients, 22 patients presented a thrombo-embolic event (13.9%) and 136 patients did not present this type of complication. The mean age was 64.03 (SD = 15.27) with no difference between the two groups. 98 (62%) of the patients were men with 15 (68.2%) in group A and 83 (61%) in group B. There was no significant difference between the two groups regarding comorbidities (hypertension, diabetes, obesity and active smoking). The average length of hospitalization in the general population was 8.29 (SD = 6.63), with a difference between the two groups: 11.5 (SD = 9.02) in group A and 7.77 (SD = 6.05) (P = .014). 88 of the patients were using anti-thrombotics before admission, with a significant difference between the two groups: 8 (36.4%) in group A and 80 (58.8%) in group B (P = .042). (Table 2).
Demographic, Anamnestic, and Medical-Surgical Characteristics.
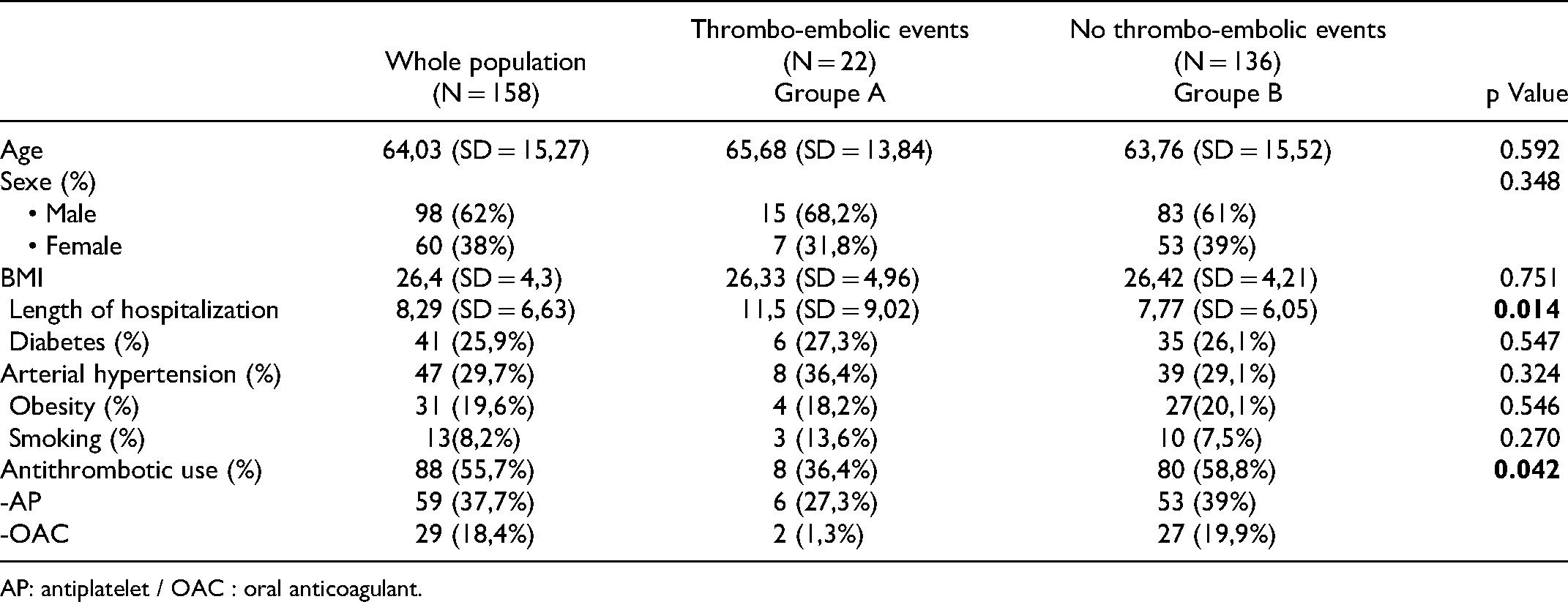
AP: antiplatelet / OAC : oral anticoagulant.
Clinical, Paraclinical, Therapeutic and Evolution Characteristics
Clinical Results
Concerning the clinical characteristics, the most frequent symptom in our patients was dyspnea with a percentage of 81.6%, on the other hand the least frequent symptom was chills with a percentage of 34.8%, the same results are observed in both groups but without significant difference.
The saturation was lower than 90% at room air on admission in 80 patients, ie (50.6), 7 presented a thrombo-embolic event afterwards, ie 31.8% compared with all the patients in group A, and 73 did not present this event, and no difference was observed between the two groups concerning the saturation on admission.
Biological Findings
Biologically, ferritin was elevated in more than 50% of patients in both groups, secondary to the inflammatory state pathognomonic of this condition, but without significant difference. Highly sensitive troponin was detected in 46.2% of patients in the general population, with a predominance in group A by a percentage of 72% compared to 42% in group B, but without significant difference. More than 55% of patients in both groups had elevated D-dimer and C-RP levels but without significant difference. Platelet count was normal in 105 (66.5%) patients at admission with 42 (26.6%) patients having thrombocytosis but no difference between the two groups, and 11 patients had thrombocytosis but with significant difference between the two groups (P = .021) (Table 3).
Clinical and Paraclinical, Management and Outcomes Characteristics.

Imaging Results
Regarding the imaging, the most frequent level of involvement was between 50% and 75% with a percentage of 40.5%, followed by the 75%-100% level (30.4%), then 25–50% (14.6%) and finally less than 25% (8.2%), and between the two groups there was no significant difference (Table 3).
Treatment Management
Regarding drug management, all patients received the national anti-covid protocol made of: Azithromycin, Zinc, Vitamin D, Vitamin C. For anticoagulation, all patients had the indication of a curative anticoagulation, the protocol used was low molecular weight heparin 100 IU/Kg/12.
Concerning oxygen therapy, the majority of patients required a high concentration mask 123 (77.8%) with no difference between the two groups, OHD was used in 90 patients (57%) with a difference between the two groups (P = .04) for non-invasive ventilation, it was performed in 58 (36.7%), and 43 patients (42.4%) had recourse to mechanical ventilation without difference between the two groups. The ventral decubitus is used in 67 patients (42.4%), and finally, venous-venous ECMO is installed in 2 patients, each in one group (Table 3).
Outcome of Complications
Concerning complications, myocarditis was observed in 1.9% of patients, pericarditis as the most frequent cardiac complication with a number of 10 patients (6.3%) with a significant difference between the two groups (P = .034), pleurisy was the most frequent pleuro-pulmonary complication with a percentage of 13.3%. Acute renal failure was observed in 77 patients (48.7%), thrombocytopenia was observed in 38 patients (24.1%) and bleeding events of all classes were observed in 4 patients with no significant difference between the two groups (P = .443). Among the 4 patients who developed a bleeding event, 2 patients were previously on an anticoagulant (50%), and the other two were not taking any antithrombotic medication.
In total, 61 patients died (38.6%), with a higher rate in group A (50%) than in group B (36.8%) but without significant difference (P = .24) (Table 2).
Predictors of Thromboembolic Events and the Impact of Prior Antithrombotic use
Length of hospital stay is a factor that may interfere with the genesis of thromboembolic complications with Ou = 0.92, 95% CI (0.863–0.983), (P = .014), ie, decreasing the length of stay by one day, will decrease the risk of thromboembolic events by 8%. Previous use of antithrombotic drugs and protective factors against thromboembolic events in our cohort. For the previous intake of an antiplatelet, with OR = 0.288, 95%CI: (0.091–0.911), and (P = .034), which means that these patients are protected 70% compared to other patients to develop a thromboembolic complication For previous use of an anticoagulant OR = 0.322, 95%CI: (0.131–0.851), and (P = .021), which means almost the same result as taking an antiplatelet drug. Thrombocytosis on admission was a risk factor with a 4-fold increased risk compared to patients with normal platelet count (OR = 4.58; 95%CI (1.2–10.627) and P = .021), and thrombocytopenia itself was not a risk factor in our cohort (Table 4).
The Factors Influencing the Thrombo-Embolic Events and Prior Anti-Thrombotic use Impact.

HFNC: High-Flow Nasal Cannula Oxygen.
To establish the impact of previous use of antithrombotic drugs, Kaplan Meier survival analysis was performed, showing a highly significant difference (Log-Rank test P = .014) between the use or not of antithrombotic drugs on protection against thromboembolic events during hospitalization (Figure 2), but with no difference in mortality between the two groups (Log-rank test 0.461) (Figure 3) and this, during the hospitalization period.

The Kaplan Meier curve showing the significant difference in terms of thrombo-embolic complications between previous use or not of antithrombotic during hospitalization on the log-rank test.

The Kaplan Meier curve showing no difference in terms of mortality between previous use or not of antithrombotic during hospitalization on the log-rank test.
Discussion
The present study tries to study the impact of the previous intake of antithrombotic drugs, either an antiaggregant or an anticoagulant, in a population at risk of developing a thromboembolic event, namely patients with a severe form of covid-19 disease and an underlying cardiopathy. According to our analysis, previous use of all classes of antithrombotics protects against thromboembolic complications, with a percentage of 71% for antiplatelet agents and 68% for anticoagulants, but without any effect on intra-hospital mortality.
Several reports have tried to find out the relationship between the previous use of antithrombotic drugs and the evolution of the disease in terms of mortality, admission to intensive care units, recourse to mechanical ventilation and thus the occurrence of thromboembolic events, but this is done on patients with or without heart disease, to our knowledge, this is the first cohort that studies this question in a rather special population: patients with previous heart disease. Concerning published reports, Chantal et al, 17 reported the same result as our study, with a protective effect on thromboembolic complications (OR = 0.19, 95% CI (0.04; 0.84) P = .029), but no effect on mortality, as well as in the same series, thromboembolic complications were more frequent in patients with high platelet reactivity to TRAP-6 with (0.96 95%CI (0.930.99), P = .02). Rivera et al, 18 reported in a large cohort, in COVID-19 positive patients, prior treatment with direct oral anticoagulants at the time of diagnosis was not associated with an improvement in thromboembolic events or rehospitalization compared to patients not taking OAC therapy, but this was in a population quite different from mine. A cohort published by Tomiteru et al 19 found a reduction in severity between patients treated with anticoagulants and antiplatelets, but this difference was not significant. Concerning platelet levels, several cohorts have demonstrated the impact between the occurrence of thromboembolic complications and thrombocytopenia. 20
In a cohort of 1476 patients by Yang et al, 21 thrombocytopenia was also associated with high risk of severity and mortality of covid-19 disease. Hanny et al, 22 found that thrombocytosis >450 × 109/L is a risk factor for thrombosis during hospitalization (adjusted OR, 3.56 [95% CI, 1.27–9.97]), the same result found in our cohort. In contrast to all the results found in published studies in the direction of risk factors of thromboembolic events, the high level of D-dimers was always associated with a high risk of thromboembolic events, 23 however, in our study, the difference was not significant, and this can be explained by the characteristics of our population: patients with heart disease, who have already experienced a thrombotic event before, linked this high level without difference in case of occurrence of thromboembolic complications or not. The results published in this sense, found high rates in patients generally without comorbidities, and without loaded cardiovascular terrain. Finally, concerning the length of hospitalization, bed rest itself and a historical factor of thrombosis, it is the case of patients admitted in intensive care units for a severe infection, our study finds that one day less in ICU will decrease the risk of a thromboembolic event by 10%, the same finding found in the results of al wafi et al 24 with a multiplication of the risk 5 times with each day more.
Regarding mortality, our result did not show a beneficial effect on the decrease of intra-hospital mortality, and this is the same result found in a meta-analysis of 12 cohorts published by Meng. 25
Limitations of the Study
Our study has several limitations, like the majority of other studies, first, the fact that it is a monocentric study, and the number of samples that is a little limited especially with regard to the number of patients who presented a thromboembolic event which is 22, again the problem of poor compliance regarding the intake of antithrombotic drugs, and drug interactions with drugs used in covid-19 such as steroids that were not taken into account, but despite its limitations, the results remain satisfactory, and let us still in the obligation to have several other reports on this issue in this special population: patients with previous heart disease.
Conclusion
COVID-19 remains a general disease, with a pro-thrombotic component that cannot be avoided, the previous use of antithrombotic drugs, although it does not improve the evolution and prognosis, but it can be a protective factor against thrombo-embolic events, especially in the population with heart disease.
Footnotes
Acknowledgments
We would like to thank the medical and nursing teams of Mohammed VI University Hospital for their significant involvement in the manage-ment of the patients included in our study
Consent
This is retrospective study
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.