
Abstract
Free-floating right-heart thrombus (FFRHT) in the context of a pulmonary embolism (PE) is a rare but serious encounter with no guidelines addressing its management. We performed a systematic review and meta-analysis addressing prevalence, clinical behavior, and outcomes of FFRHT associated with PE. Among the included 397 patients with FFRHT and PE, dyspnea was the main presenting symptom (73.3%). Obstructive shock was documented in 48.9% of cases. Treatment with thrombolytic therapy, surgical thrombectomy, and percutaneous thrombectomy was documented in 43.8%, 32.7%, and 6.5% of patients, respectively. The overall mortality rate was 20.4%. Syncope (p: 0.027), chest pain (p: 0.006), and obstructive shock (p: 0.037) were significantly associated with mortality. Use of thrombolytic therapy was significantly associated with survival (p: 0.008). A multivariate logistic regression model to determine mortality predictors revealed that syncope (OR: 1.97, 95% CI: 1.06–3.65, p: 0.03), and obstructive shock (OR: 2.23, 95% CI: 1.20–4.14, p: 0.01) were associated with increased death odds. Treatment with thrombolytic therapy (OR: 0.22, 95% CI: 0.086–0.57, p: 0.002) or surgical thrombectomy (OR: 0.35, 95% CI: 0.137–0.9, p: 0.03) were associated with reduced death odds. Meta-analysis of observational studies revealed a pooled prevalence of FFRHT among all PE cases of 8.1%, and overall mortality of 23%. Although uncommon, the presence of FFRHT in the context of PE is associated with high obstructive shock and mortality rates. Favorable survival odds are observed with thrombolytic therapy and surgical thrombectomy. Data are derived from case reports and observational studies. Clinical trials elucidating these findings are needed.
Introduction
PE is one of the leading causes of cardiovascular (CVS) mortality worldwide. 1 The mortality rates vary depending on the demographics, nature, and severity of PE. While it is unknown in many developing countries, the annual mortality rate from PE can reach as high as 300 000 deaths in some developed nations. 2 The annual incidence of PE ranges from 1–11.3 per 1000 persons, depending on the age at presentation. 3 Numerous risk factors for the development of PE have been identified with variable associations.4,5 History of VTE is considered one of the strongest risk factors. 4 Other significant risk factors include, but are not limited to, hypercoagulability states, malignancy, recent surgery, and immobilization. 5
Free-Floating Right Heart Thrombi (FFRHT)
In PE, the emboli usually originate from the deep veins of the lower extremities and pelvis. They travel to the lungs by crossing the right heart chambers to get lodged in the proximal or distal pulmonary artery branches where they cause abnormalities in hemodynamics and gas exchange. 6 Right heart thrombi can originate within the right heart chambers (as a result of dilatation of these chambers and secondary blood stasis) (type-B), or travel from the peripheral veins (usually of the lower extremities) to the right heart chambers (type-A). Type-B thrombi are non-mobile, non-specific clots that resemble left heart thrombi. These thrombi rarely result in serious consequences because of their attachment to the heart walls. On the contrary, type-A thrombi are usually a serious encounter and can be seen on echocardiography as worm-shaped FFRHT (also known as clot-in-transit “CIT” or thrombus-in-transit “TIT”) 7 (Figure 1). Because of their nature as highly mobile, unstable, and not attached to the heart walls, FFRHT can result in catastrophic consequences. 7 They can embolize at any moment resulting in a severe form of PE which can impact hemodynamics through right ventricular (RV) dilation, RV failure, reduction in left ventricular filling pressure, reduction of cardiac output, and cardiogenic shock. They can also impact gas exchange, causing ventilation/perfusion (V/Q) mismatch, reduction of alveolar-capillary surface and the opening of intrapulmonary and intracardiac shunts, eventually resulting in arterial hypoxia.8,9 Some studies reported mortality rates from FFRHT higher than 40% when they are present in the context of PE.7,10,11 The exact prevalence of FFRHT among patients diagnosed with PE is uncertain. While some reports estimated a prevalence of around 4%, others suggested a prevalence as high as 18%.12–14 Nevertheless, the condition is probably underestimated because of the underutilization of echocardiography in cases of PE. 13 Despite the reported high mortality and the advances in their detection, the optimal management of FFRHT in the context of PE remains a therapeutic dilemma due to the lack of evidence-based guidelines. Very few pooled analyses previously addressed some of the outcome characteristics of right heart thrombi based on the treatment modalities. Nevertheless, these reports included only case reports and case series with a mix of cases of FFRHT (type-A) as well as the “low-risk” type-B right heart clots regardless of the presence of PE.15,16

Echocardiography showing free-floating right atrium thrombus (arrow).
Aims of the Systematic Review
In this systematic review and meta-analysis, we aimed to pool the available data on the prevalence, clinical behavior, and outcomes specific to the presence of FFRHT in the context of PE. Additionally, we aimed to study the associations of various factors, including treatment modalities, with the mortality outcomes. To the best of our knowledge, this is the first and most comprehensive report that specifically focuses on the freely mobile non-attached right heart thrombi when present in the context of acute PE.
Methods
Data Sources and Search Strategy
The protocol of this systematic review has been registered in PROSPERO (No. CRD42020221538). A systematic literature search was performed for articles published in English using PubMed, Google Scholar, and SCOPUS for any date up to November 18, 2020. Search terms used were: Free-floating right heart thrombi” OR “Free-floating cardiac thrombi” OR "Free-floating right atrial thrombi" OR "Free-floating RA thrombi" OR “Free-floating right ventricular thrombi” OR “Free-floating RV thrombi” OR "Thrombus-in-transit" OR "Clot-in-transit" OR “Right heart thrombi” OR “Right atrial thrombi” OR “RV thrombi” OR “Mobile heart thrombi” OR “Mobile right heart thrombi”. Retrieved articles were analyzed independently by one of three authors (FA, SA, and TO).
Study Selection
All the extracted citations were initially screened from the title and abstract, and subsequently, a detailed manual screening was performed. Original studies (case reports, series, observational retrospective, prospective studies, and clinical trials) that reported FFRHT causing a PE were included in the review (Figure 2). Studies reporting FFRHT that did not result in PE (in absence of PE), or thrombi attached to the valves or walls of the right atrium, RV, or an intracardiac device (not free-floating) were excluded. Four studies met the inclusion criteria were excluded from final qualitative analysis because their data on FFRHT could not be individualized. Authors of three of these studies did not reply to our emails while the author of the fourth one replied but could not provide requested data on FFRHT (Figure 2).

PRISMA flow diagram of the article screening process with the details of included and excluded studies.
Quality Assessment
The Quality of observational studies was assessed using the Methodological Index for Non-Randomized Studies (MINORS) assessment tool. 17 The items included are; a clearly stated aim, inclusion of consecutive patients, prospective collection of data, endpoints appropriate to the aim of the study, unbiased assessment of the study endpoint, follow-up period appropriate to the aim of the study, loss to follow up less than 5%, and prospective calculation of the study size. Additional criteria for comparative studies included: adequate control group, contemporary groups, baseline equivalence of groups, and adequate statistical analyses. 17 Two authors (FA/AS) independently assessed the potential risk of bias in the studies included using the MINORS. The items were scored 0 if not reported; 1 when reported but inadequate; and 2 when reported and adequate. The global ideal score was 16 for non-comparative studies and 24 for comparative studies. The quality of the added cases was assessed by two reviewers independently (FA and HC) using the Joanna Briggs Institute case report appraisal checklist for inclusion in systematic reviews. 18 In case of any dispute in the quality assessment, a third reviewer (WI) decision was required.
Data Extraction and Statistical Analysis
Data concerning demography, clinical presentation, laboratory, and imaging profile as well as treatment and outcome data were noted for each case. Because of variation in reporting the timing of PE-related death among different studies, the overall PE-related mortality was considered. Categorical variables were expressed as numbers and percentages. Continuous variables were expressed using the mean ± standard deviation (SD), or the median with the interquartile range (IQR). The Chi-square test, fisher's exact test, or Mann-Whitney U test was used to compare variables where appropriate. A binary logistic regression model of analysis was used to study the association between mortality and different treatment modalities as well as hemodynamic status. Meta-analysis using the random-effect model was performed to estimate the pooled prevalence, percentage, and corresponding 95% confidence interval (CI) from observational studies. The Freeman-Tukey Transformation (Arcsine Square Root Transformation) was used to stabilize the variances and calculate the weighted summary proportion. The measure of heterogeneity reported included the Cochrane's Q statistics and the I2 index with the level of heterogeneity defined as poor < 25, moderate > 50, and high > 75. Publication bias was assessed with a funnel plot and the Egger test. Data handling and analysis were performed using the IBM SPSS Statistical software version 26 (Armonk, NY: IBM Corp.) and the MedCalc Statistical Software version 20.109 (MedCalc Software bv, Ostend, Belgium; https://www.medcalc.org).
Results
A total of 211 publications (168 case reports, 32 case series, 8 retrospective studies, and 3 prospective studies) comprising 397 cases were included in the final analysis based on the inclusion and exclusion criteria (Figure 2).
Demographics and Clinical Features of all FFRHT Cases
Among the 397 FFRHT patients with PE included in this review, the average age at presentation was 59.1 ± 16.8 years (males constituted 53.4%). Dyspnea was the most reported symptom in 73.3% of patients. Obstructive shock was documented in 48.9% of patients, and syncope/unconsciousness was the initial manifestation in about 28.4%. (Table 1) and (Figure 3).

Clinical presentation of FFRHT in the context of PE.
Clinical and Demographic Characteristics of the Included Patients (N = 397).

Risk Factors and Associated Comorbidities among all FFRHT Cases
Immobility was the most reported risk factor in 30.1% of cases. About 29% of the patients were reported to have concomitant DVT, and 16.3% had a prior history of VTE. No provoking factor was reported in 12.8% of cases (Table 1).
Diagnostics
Echocardiography was the image of choice in detecting the FFRHT in 99.4% of cases. In one case, the FFRHT was captured by an electrocardiogram-gated, contrast-enhanced, multi-slice computed tomography as an impending paradoxical embolism from a floating thrombus entrapped in a patent foramen ovale (PFO). 19 In another case, the FFRHT was diagnosed via a point of care ultrasonography. 20 Associated PE was diagnosed by CTPA, V/Q scan, or magnetic resonance imaging (MRI) of the thorax in 60.5%, 37.3%, and 2.2% of cases, respectively. RV strain pattern was reported on electrocardiography (ECG) in 19.4% of cases (Table 1).
Management
Among the total of 397 patients, thrombolytic therapy was used in 43.8% of patients, whereas, surgical thrombectomy and percutaneous thrombectomy were performed in 32.7% and 6.5% of cases, respectively. Anticoagulation was the only reported treatment in 15.8% of patients (Table 2).
Treatment Modality and Outcomes (N = 397).

Outcome Analysis
Eighty-one patients were reported to have died resulting in an overall mortality rate of 20.4%. PE recurrence was reported in 5.5% of cases (Table 2).
Predictors of Mortality Outcome
Initial presentations with syncope/unconsciousness (p: 0.027), Obstructive shock (p: 0.037), or chest pain (p: 0.006) were significantly associated with death from FFRHT in the context of PE. On the contrary, the use of thrombolytic therapy was significantly associated with survival (p: 0.008) (Table 3). A multivariate logistic regression model was used to analyze the relationship between the treatment modality, hemodynamic status, and mortality outcome. The model revealed that treatment with thrombolytic therapy (OR: 0.22, 95% CI: 0.086–0.57, p: 0.002) or surgical thrombectomy (OR: 0.35, 95% CI: 0.137–0.90, p: 0.03) was significantly associated with reduced odds of death whereas, presentations with syncope/unconsciousness, and Obstructive shock were associated with increased odds of death (OR: 1.97, 95% CI: 1.06-3.65, p: 0.03), and (OR: 2.23, 95% CI: 1.20–4.14, p: 0.01), respectively (Table 4).
Distribution of Patient Characteristics by Mortality Outcome.

Logistic Regression for Mortality Outcome*.
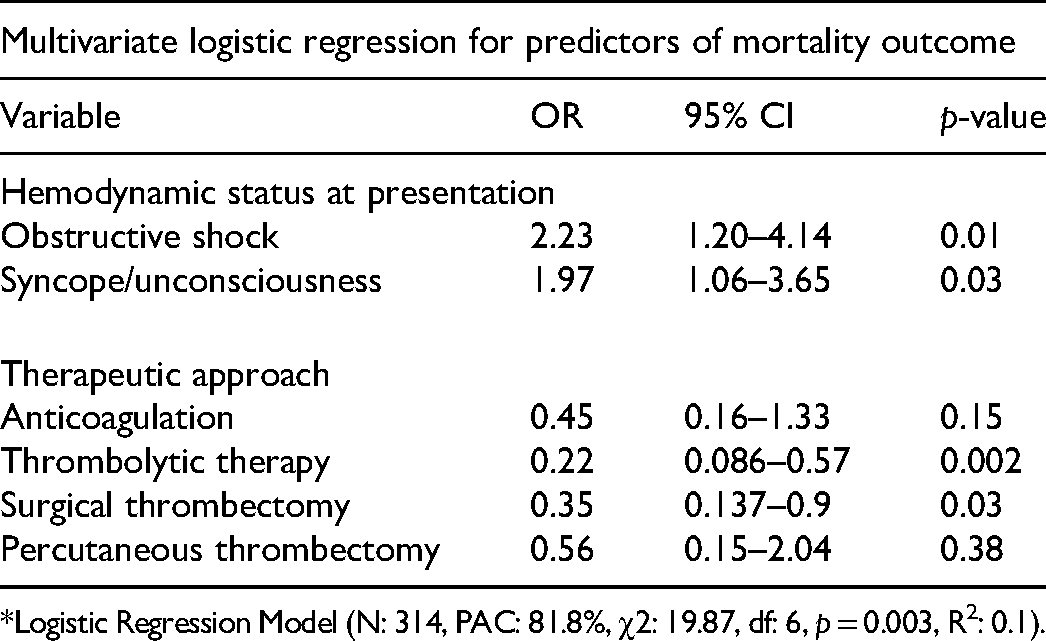
*Logistic Regression Model (N: 314, PAC: 81.8%, χ2: 19.87, df: 6, p = 0.003, R2: 0.1).
Meta-Analysis of the Included Observational Studies
Tables 5 and 6 summarize the clinical characteristics and treatment of FFRHT associated with acute PE from observational studies. Meta-analysis of these observational studies revealed a pooled prevalence of FFRHT among all PE cases of 8.1% with an overall mortality of 23% (Table 7).
Clinical Features of FFRHT in the Context of PE from Observational Studies (N = 7).

Treatment and Outcomes of FFRHT in the Context of PE from Observational Studies (N = 7).

Meta-Analysis of Prevalence, Outcomes, and Echocardiographic Features from Observational Studies (N = 11) (Random-Effect Model).

Quality Assessment of the Included Observational Studies
The results of quality assessment of the included observational studies using the MINORS assessment tool are shown in Table 8.
Quality Assessment of the Observational Studies Using the MINORS Assessment Tool. 17 *
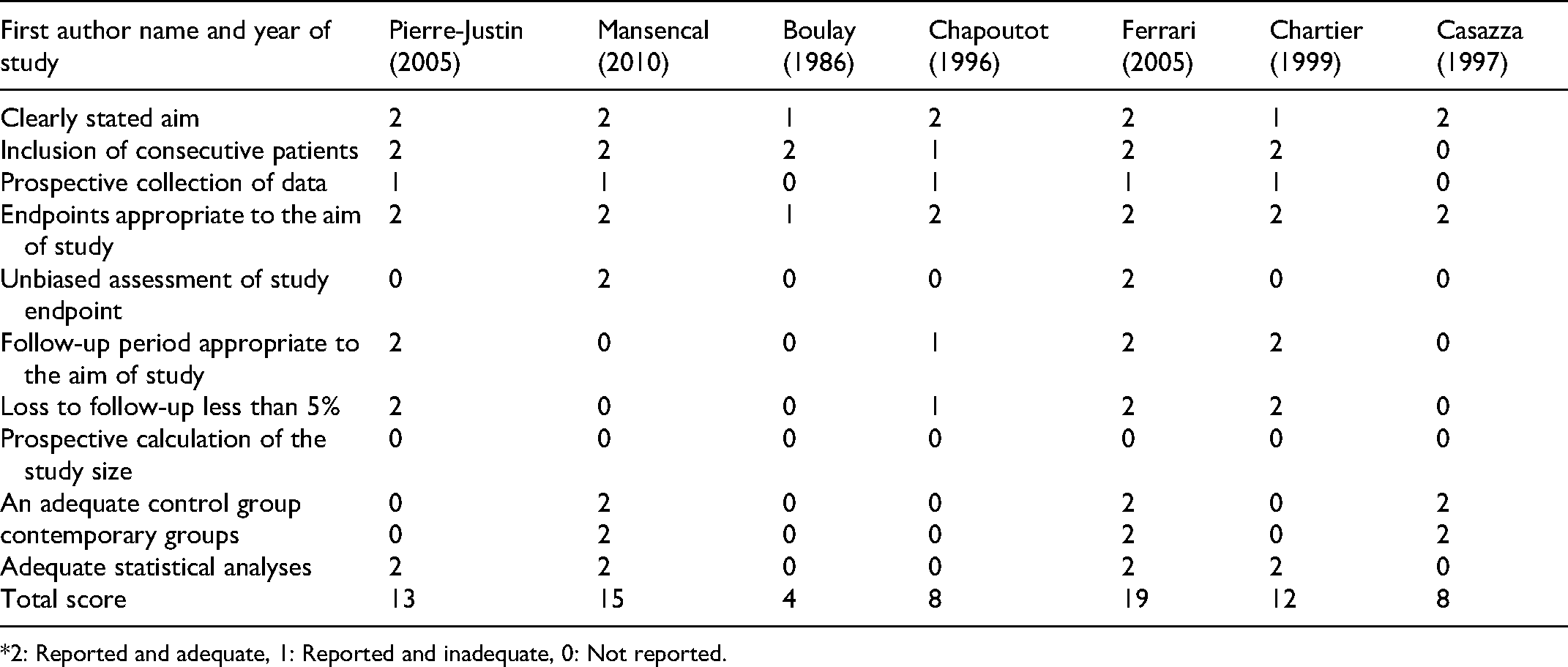
*2: Reported and adequate, 1: Reported and inadequate, 0: Not reported.
Discussion
Major Findings in the Current Review
The current systematic review and meta-analysis represent the most extensive review of 397 cases of FFRHT associated with PE. It confirmed the previously reported high mortality rate (20.4%) among patients with FFRHT and PE. In two pooled analyses of patients with right heart thrombi in general, Athappan et al, and Islam et al reported mortality rates ranging from 18.7%-23.2%.15,16 The Right Heart Thrombi European Registry Group reported a 30-day mortality rate of patients with all types of right heart thrombi and PE of 19% as compared to those with PE alone (8%). 21 Another striking finding in the present review is the high rate of obstructive shock (about 49%) among patients with FFRHT and PE. Such a high figure of rapid decompensation has also been reported by other investigators and emphasizes the notion that FFRHT represents an extreme medical emergency and should be treated urgently and promptly. In a retrospective study of 38 patients with FFRHT and PE, Chartier et al reported a rapid decompensation and death in 21.1% of the patients within the first day after admission. 13 A 33.5% prevalence of shock was also reported by Islam et al among patients with right heart thrombi. 16 The frequency of hemodynamic instability among patients with right heart thrombi, in general, was estimated to be around 20% in another review. 15 Nevertheless, unlike the current review, these reviews included also cases of attached thrombi (immobile thrombi) that are associated with lower rates of complications. 15 Obstructive shock seems to occur more frequently in patients with FFRHT and PE than in patients with PE alone (10%). 22 Several plausible reasons can explain such high rates of mortality and serious hemodynamic consequences. On one hand, the highly mobile nature, and instability of the FFRHT make such clots embolize and result in a severe PE at any moment. Some reports have suggested that over 90% of FFRHT can end up in PE.12,21 Furthermore, despite the lack of previous studies documenting the correlation between the hemodynamic consequences and the size of the FFRHT, the latter seems another plausible explanation that warrants further evaluation. Finally, the lack of a clear consensus and guidelines specific to the management of FFRHT in association with PE could have contributed to the dismal outcomes. The current review reported important risk factors and comorbidities associated with the presence of FFRHT. These risk factors were not different from those of VTE in general. Concomitant DVT was observed in 28.8% of patients in the current review, whereas; a prior history of VTE was reported in about 16.3%. DVT is considered one of the most important risk factors of FFRHT and PE 11 as the clot originates from DVT in a lower limb in the majority of cases. Nevertheless, previous studies utilizing compression ultrasonography of the deep veins (sensitivity >90%) reported a DVT prevalence of only 30–50% in patients with PE.4,23–25 Utilizing venography as the diagnostic test, DVT was found in 70% of patients with proven PE. 26 In agreement with previous studies on PE and DVT, immobility, CVS diseases, malignancy, and trauma were important risk factors. 27 Interestingly, COVID-19 infection was reported as the main risk factor in 3% of cases in the current review.20,28–32 Recent evidence suggests that the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) interacts with different cellular molecules including enzymes, endothelial cells, platelets, neutrophil extracellular traps, thrombin, and histones, resulting in endothelial damage and formation of microthrombi. 33 In agreement with the prior evidence, 34 we found that combined CVS diseases (including CAD disease, valvular disease, atrial fibrillation, and patent foramen ovale ”PFO”) to be the most commonly reported comorbidity. Interestingly, the presence of PFO was documented in 23 cases in the current review, out of which one died. PFO is a high-risk condition for the development of cardiac thrombi due to its tunneled anatomy, leading to potential stasis and thrombus development. 35 Moreover, prior studies have linked the finding of PFO to the poor outcome of patients with acute PE. In a prospective study of 139 consecutive patients with major PE who underwent contrast echocardiography at presentation, PFO was diagnosed in 48 patients (35%). Those patients had a death rate of 33% as opposed to the 14% in patients with a negative echo-contrast examination. The difference was statistically significant. 36 Nevertheless, we could not find any significant association between any of the reported commodities and the mortality/survival outcomes in the present review. Similar to those with isolated PE, common presenting symptoms in patients with FFRHT and PE, in the current review, were dyspnea and chest pain. 37 Interestingly, syncope was reported in about 28.4% of patients in the present review. The rate of syncope among patients with FFRHT and PE was more than in those previously reported with isolated PE. Previous studies on acute PE alone estimated a prevalence of syncope ranging from 1% to 20%. Three pathophysiological mechanisms have been proposed for the development of syncope in acute PE including acute right heart failure, hemodynamically unstable dysrhythmia (such as bradycardia or tachycardia), and vasovagal reflex. 38 Furthermore, in agreement with previous reports that linked presentation with syncope to mortality from PE, this association was also confirmed in the current review. 39 Significant mortality associations with the presence of chest pain, and obstructive shock (as initial presenting features) were also found in this review. In a retrospective study on 38 patients with FFRHT, Chartier et al found only severe hypoxia and cardiac arrest to be significantly associated with mortality. None of the other presenting features showed a statistically significant difference concerning mortality outcome. 13 Concurring with the findings in the current review, Islam et al, in their review on all types of right heart thrombi, reported dyspnea as the commonest presenting complaint (77%) with no statistically significant associations of the presenting feature with outcomes. 16 In contrast, Athappan et al, in a review of 328 patients with all types of right heart thrombi, reported a significant association of dyspnea and hemodynamic instability with mortality. 15 Unfortunately, there is no pretest probability scoring system to predict the presence of FFRHT. Appropriate cardiac imaging is required for its diagnosis. CTPA has replaced conventional pulmonary angiography as the gold-standard method for diagnosing PE. Besides being minimally invasive, CTPA provides a high level of image quality resulting in a diagnostic performance that equals or surpasses that of conventional pulmonary angiography, with sensitivity and specificity varying between 83%–100% and 89%–96%, respectively. In addition, CTPA identifies the exact location of the PE.40–44 Nevertheless, CTPA is not the modality of choice in diagnosing intracardiac thrombi. Furthermore, important clot characteristics such as mobility are difficult to assess by CTPA. Transthoracic echocardiogram (TTE) and transesophageal echocardiogram (TEE) provide the diagnostic tools of choice for FFRHT with better visualization and characterization of the thrombi. 11 However, the sensitivity and specificity of TTE and TEE in diagnosing right heart thrombi can significantly decrease in certain unfavorable circumstances such as arrhythmia, the variable posterior position of right ventricular thrombi, or an obese habitus. In some cases, right heart thrombus might be missed due to its proximity to the myocardium and their similar echogenicity. 45 In two cases included in the current review, the initial diagnosis of FFRHT was made by electrocardiogram-gated, contrast-enhanced, multi-slice computed tomography, and point of care ultrasonography.19,20 The role of point of care ultrasonography as a fast and easy tool for the detection of FFRHT in patients with PE warrants further evaluation in future studies. RV strain on TTE or ECG is one of the risk stratification markers in patients with PE. In the present review, a significantly higher rate of RV strain pattern on ECG was observed in the survived group than in those who died (21.5% vs 9.3%). Nevertheless, this finding should be interpreted with caution as it correlates mortality with the RV abnormalities on ECG rather than TTE which were not reported in many cases. Furthermore, in a previous review on right heart thrombi, Athappan et al reported no significant correlation between RV strain and mortality. 15 Similarly, Islam et al reported RV strain in 60% of the survived and 71% of deceased patients, with no significant correlation with mortality. 16 We have demonstrated in the current review that thrombolytic therapy and surgical thrombectomy were the treatment modalities associated with favorable odds of survival. In another pooled analysis conducted on right heart thrombi in general, a survival benefit with thrombolytic therapy but not with surgical thrombectomy over anticoagulation alone was reported. 15 Similar findings were also reported by Islam et al. 16 Furthermore, in a retrospective study of 177 patients with right heart thrombi in general, Rose et al found that patients who received thrombolytic therapy were noted to have an OR for mortality of 0.33 (95% CI, 0.11 to 0.98), indicating a protective effect for thrombolytic therapy compared to anticoagulation alone. The OR for mortality in the surgical thrombectomy group was 0.86 (95% CI, 0.32 to 2.29) compared to anticoagulation, but the effect was not statistically significant. 46 On the contrary, an earlier meta-analysis by Kinney et al reported that heparin treatment was associated with somewhat more favorable odds of survival compared to thrombolytic therapy or surgical thrombectomy. Nevertheless, not all patients in their meta-analysis had PE and their analysis included also attached thrombi. 47 A large retrospective comparison of 2111 adults with acute PE who underwent either thrombolytic therapy (n = 1854; 88%) or surgical thrombectomy (n = 257; 12%) as the first-line therapy did not find difference in the 30-day mortality between those who underwent thrombolytic therapy and those who underwent surgical thrombectomy (15.2% vs 13.2%; OR; 1.12, 95% CI; 0.72–1.73). 48 Evidence supporting the use of percutaneous thrombectomy in acute PE is largely derived from registries and case series.4,49,50 A word of caution needs to be mentioned concerning the reported associations between surgical thrombectomy and percutaneous thrombectomy with the survival outcome. Multiple potential confounders such as sicker patients being considered for surgical thrombectomy or percutaneous thrombectomy, local expertise, and patient preference can affect this association. Moreover, the timing of these procedures seems to have a critical role as most patients who survived surgical thrombectomy had the intervention planned and carried out in the first few hours of presentation.12,51–54 Such factors, along with the plethora of evidence supporting the use of thrombolytic therapy in PE, its easy availability, and reduced needs for expertise (compared to surgical thrombectomy or percutaneous thrombectomy) may explain the more established role of thrombolytic therapy in various types of PE as compared to surgical thrombectomy and percutaneous thrombectomy. Interestingly, we found a half-dose (50 mg alteplase) used in a case series of five patients, with excellent outcomes. 55 There were no thrombolytic therapy-related complications in the majority of patients. In general, specific thrombolytic therapy-related complications were reported in only six patients and included intracranial hematoma, epistaxis, mild hematuria, circulatory collapse, allergic reaction to urokinase, and unspecified sudden death.56–60 A retrospective study on right heart thrombi and PE from Turkey reported major bleeding after thrombolytic therapy in 18% of patients, similar to bleeding trends seen in PE from other causes. 61 Our review found a median hospital stay of 9.5 days in patients with FFRHT in the context of PE which seems longer than that of PE in general (6 days). 62 This outcome has not been reported previously.
Points of Strength in the Current Review
The current review represents the most updated and extensive systematic review that focused on the free-floating type of right heart thrombi (the most unstable and risky type of right heart thrombi). In two previous pooled analyses, Athappan and Islam included only case reports and case series with a mix of cases of FFRHT (type-A) as well as the “low-risk” type-B right heart clots.15,16 Furthermore, the presence of associated acute PE as an inclusion criterion was reported in only one of these analyses. 15 In the current review, we have also elucidated the associations of clinically significant variables with the survival outcome. This review offers insights and direction for conducting large prospective studies in this patient population to validate its results and formulate guidelines for managing FFRHT-associated PE.
Limitations of the Current Review
A major limitation of the current review is publication bias. Although retrospective and prospective studies were more represented compared to previous reviews, the results of the current review are largely derived from case reports and case series. Medical journals often publish only cases that show a positive response to a certain treatment modality or have a peculiar presentation. We could not find any clinical trial on FFRHT in the context of PE to include in the current review. Furthermore, only published reports in the English language were included in the current review. Another limitation of the current review is the lack of information on some potential confounders affecting survival outcomes. Examples of such confounders are the availability, and the local expertise with surgical thrombectomy and percutaneous thrombectomy as treatment approaches for individualized cases.
Conclusion
The prevalence of FFRHT among all PE cases is 8.1% and its presence in the context of acute PE is associated with serious hemodynamic consequences including obstructive shock and a high mortality rate. Knowledge about the clinical behavior, management, and outcomes of FFRHT in the context of PE is largely derived from case reports and observational studies. Concomitant peripheral DVT may be seen in about one-third of patients. The use of thrombolytic therapy and surgical thrombectomy in patients with FFRHT and PE may have a potentially positive impact on the odds of survival, whereas, initial presentations with syncope/unconsciousness or obstructive shock are associated with increased odds of death. Prospective and randomized controlled trials elucidating these findings are desperately needed to validate the results of this review and formulate guidelines and clear consensus specific to the management of FFRHT in association with acute PE. The role of point-of-care ultrasonography as a simple and rapid diagnostic tool for FFRHT also deserves further evaluation.
Supplemental Material
sj-docx-1-cat-10.1177_10760296221140114 - Supplemental material for Prevalence, Outcome, and Optimal Management of Free-Floating Right Heart Thrombi in the Context of Pulmonary Embolism, a Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cat-10.1177_10760296221140114 for Prevalence, Outcome, and Optimal Management of Free-Floating Right Heart Thrombi in the Context of Pulmonary Embolism, a Systematic Review and Meta-Analysis by Wanis H. Ibrahim, Fateen Ata, Hassan Choudry, Huzaifa Javed, Khaled M Shunnar, Abdullah Shams, Abdullah Arshad, Adel Bosom, Mohammed H.A. Elkahlout, Bisher Sawaf, Shahda M.A. Ahmed and Tinuola Olajide in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The Qatar National Library funded the publication of this manuscript.
Author Contributions
Data Availability Statement
All relevant data is presented in the review and Supplemental material.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This systematic review does not involve endangering participant rights. Ethical approval was not required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.