
Abstract
Background
Unfavourable clot microstructure is associated with adverse outcomes in ST elevation myocardial infarction (STEMI). We investigated the effect of comorbidities and anti-platelet treatment on clot microstructure in STEMI patients using fractal dimension (df), a novel biomarker of clot microstructure derived from the visco-elastic properties of whole blood.
Methods
Patients with STEMI (n = 187) were recruited sequentially receiving aspirin with Clopidogrel (n = 157) then Ticagrelor (n = 30). Patient characteristics and blood for rheological analysis obtained. We quantified df using sequential frequency sweep tests to obtain the phase angle of the Gel Point which is synonymous with the clot microstructure.
Results
Higher df was observed in males (1.755 ± 0.068) versus females (1.719 ± 0.061, p = .001), in patients with diabetes (1.786 ± 0.067 vs 1.743 ± 0.046, p < .001), hypertension (1.760 ± 0.065 vs 1.738 ± 0.069, p = .03) and previous MI (1.787 ± 0.073 vs 1.744 ± 0.066, p = .011) compared to without. Patients receiving Ticagrelor had lower df than those receiving Clopidogrel (1.708 ± 0.060 vs 1.755 ± 0.067, p < .001). Significant correlation with df was found with haematocrit (r = 0.331, p < .0001), low-density lipoprotein (LDL) (r = 0.155, p = .046) and fibrinogen (r = 0.182, p = .014). Following multiple regression analysis, diabetes, LDL, fibrinogen and haematocrit remained associated with higher df while treatment with Ticagrelor remained associated with lower df.
Conclusions
The biomarker df uniquely evaluates the effect of interactions between treatment and underlying disease on clot microstructure. STEMI patients with diabetes and elevated LDL had higher df, indicating denser clot. Ticagrelor resulted in a lower df than Clopidogrel signifying a less compact clot.
Introduction
Coronary thrombosis is well established as a central feature of acute myocardial infarction 1 and the risk of myocardial infarction is increased by both inherited and acquired hypercoagulable states. 2 Most myocardial infarctions are precipitated by rupture of vulnerable atherosclerotic plaque with exposure of the subendothelial matrix to blood leading to promotion of platelet activity and coagulation pathway activation resulting in arterial thrombosis, vessel occlusion and myocyte necrosis. 3
In the treatment of ST-elevation myocardial infarction (STEMI) early revascularisation with primary percutaneous intervention is the priority to restore perfusion and limit cell necrosis, significantly improving morbidity and mortality. 4 Following revascularisation, treatment of co-morbid risk factors such as diabetes, hypertension, hyperlipidaemia and smoking is required and a dual antiplatelet regime including aspirin and a second antiplatelet agent is recommended to maintain stent patency and prevent further thrombus related ischaemic events. 5
Recent studies have shown the importance of the mechanical properties of the clot in both the effectiveness of treatment and patient outcome, with poor outcome associated with clot formation of highly dense and tightly packed fibrin microstructures which are resistant to deformation and therapeutic breakdown.6,7 Current techniques such as electron microscopy that are used for assessing clot microstructure are not suitable for routine use in a clinical setting. 8 A novel biomarker of clot quality has been developed that assesses the viscoelastic properties of coagulating blood to quantify its clot microstructure in terms of a fractal dimension (df) with increasing values representing denser, more complex clots. 8 The measurement of df uses whole blood and can be performed in a near patient setting thus providing a rapid assessment of coagulation. 8 It has been shown that patients with atherosclerosis are associated with rapidly forming, denser, and more compact clots and that clot quality can be modified by anti-thrombotic and antiplatelet therapy.9,10
In this study we aimed to investigate the effect of comorbidities and treatment on clot microstructure in a cohort of STEMI patients using the novel biomarker df.
Patients and Methods
Study Design and Population Group
This study complied with the declaration of Helsinki and was approved by a local Research Ethics Committee (Wales Research Ethics Committee 6; REC reference number 13/WA/0366). Adult (≥18 years) patients who had suffered a STEMI and received primary PCI (PPCI) were recruited at a tertiary centre. Informed written consent was obtained for all participants the morning after (12 h) admission of PPCI. Exclusion criteria included any known malignancy, blood dyscrasia, anticoagulation use prior to hospital admission or requirement for prolonged anticoagulation or GP IIb/IIIa antagonist use following PPCI.
Prior to PPCI all patients received 300 mg of aspirin and a dose of P2Y12 inhibitor (either 600 mg of Clopidogrel for the initial 157 patients then following a change in departmental policy 30 patients received 180 mg of Ticagrelor). During PCI, anticoagulation was achieved via a bolus of Bivalirudin (0.75 mg/kg) followed by an infusion (1.75 mg/kg/hr) or unfractionated heparin given as a weight adjusted dose (80-100 mcg/kg) depending on the operator's preference. All patients continued to receive 75 mg of aspirin and either 75 mg of Clopidogrel or 90 mg of Ticagrelor commencing 12 h after the procedure. Routinely prescribed venous thromboprophylaxis was withheld until after blood sampling.
Demographic Variables
Demographics data was collected for each patient, including presence of diabetes, hypertension, smoking status, previous myocardial infarction, family history of ischaemic heart disease, statin usage and low-density lipoprotein level (LDL). In addition, ischaemic time (time from symptoms onset to restoration of coronary flow) was recorded. All cause mortality was obtained for all patients out to 2 years from the index PPCI.
Blood Sampling
Twenty ml of blood was drawn on the day following the PCI procedure (at least 12 h following the end of the PPCI) to allow effects of peri-procedural anticoagulation to have worn off and after the prophylactic dose of the P2Y12 inhibitor had been administered. Each blood sample was divided into several aliquots. One aliquot of whole venous blood was used immediately for viscoelastic measurements. The remaining aliquots were used to perform standard coagulation screens and full blood count (FBC). The maximum troponin T value during admission was also recorded.
Laboratory Markers
A 4 ml aliquot of blood was used for FBC analysis, samples being collected into plastic, full-draw dipotassium EDTA Vacuettes (Greiner Bio-One, Stonehouse, UK Ref: 454286). FBC was analyzed using a Sysmex XE 2100 (Sysmex UK, Milton Keynes, UK) automated haematology analyser within 2 h of collection.
An additional 4.5 ml was used for routine coagulation studies, being transferred immediately into citrated silicone glass Vacutainers (0.109M) (Becton-Dickinson, Plymouth, UK Ref: 367691). Prothrombin Time (PT), activated partial thromboplastin time (APTT) and Clauss fibrinogen were measured using a Sysmex CA1500 analyser within 2 h of collection. Fibrinogen calibration was verified against the second International Fibrinogen Standard Version 4 (NIBSC code 96/612). All reagents were obtained from Siemens, (Frimley, UK). All testing was performed within 2 h of sample collection.
Rheometric Measurements: the Gel Point
In this study a 6.6 ml aliquot of whole unadulterated venous blood was loaded into a double-gap concentric cylinder measuring geometry of a TA Instruments AR-G2 (TA Instruments, New Castle, DE, USA) controlled-stress rheometer (at 37°C ± 0.1°C) in a near patient setting. Sequential frequency sweep tests were performed to obtain the Gel Point (GP), which identifies the transition of the blood from a visco-elastic liquid to a visco-elastic solid. 8 The instant where the phase angle becomes frequency independent (identified by crossover of phase angle at the 4 frequencies) is the GP and marks where the blood's fibrin network first becomes a sample spanning haematological stable clot ie capable of performing haemostatic functionality. The phase angle at the GP is synonymous with how the fibrin microstructure of the clot is organised and can be quantified using fractal dimension (df). 8 Full details of the technique are available as described in previous publications.8–10
Statistical Analysis
Statistical analysis was performed using Graph Pad Prism 9.0. Descriptive statistics of tests were calculated as mean and standard deviation (SD). Association between variables was explored using two-sample comparisons undertaken using the two-sample t-test to investigate differences in df. Pearson's correlation analysis was used to investigate significant relationships between df and continuous variables that were normally distributed. Multiple Regression was used to investigate significant relationships between df and the continuous predictors investigated and factors demonstrating significant association with df. Results were deemed significant when p < .05 and the absence of multicollinearity was confirmed using Variance Inflation.
Results
Influence of Patient Parameters on Fractal Dimension (df) of the Incipient Clot
In total, 187 patients with STEMI undergoing PPCI were included. The baseline demographic details are included in Table 1. The 2-year mortality for all patients was 4.8%. There was no difference in mortality in patients taking Clopidogrel (5.1%) and Ticagrelor (3.3%), p > .99. Our data (Table 2) demonstrated that df was significantly higher in male patients than females (1.755 ± 0.068 vs 1.719 ± 0.061, p = .001) and in those with diabetes compared with those without diabetes (Figures 1 and 2) (1.786 ± 0.067 vs 1.743 ± 0.046. p < .001). It was also higher in those with hypertension compared to without (1.760 ± 0.065 vs 1.738 ± 0.069, p = .03) and in those with a history of previous MI compared to without (1.787 ± 0.073 vs 1.744 ± 0.066, p = 0.011). No significant difference in df was observed between smokers and non-smokers, those receiving and not receiving statin therapy and those with and without a family history of ischaemic heart disease. Ischaemia time was separated into <12 h and prolonged ischaemic time (>12 h) and there was no difference in df between these two groups. Importantly, patients receiving the P2Y12 platelet inhibitor Ticagrelor had a significantly lower df than those receiving Clopidogrel (1.708 ± 0.060 vs 1.755 ± 0.067, p < .001).

Comparison of mean df of patients with diabetes (1.79 ± 0.07) and without (1.74 ± 0.05) p < .001, following treatment with ticagrelor (1.71 ± 0.06) and clopidogrel (1.76 ± 0.07) p < .001, hypertension (1.76 ± 0.07) and no hypertension (1.74 ± 0.07) p = .03 and male (1.76 ± 0.07) with female (1.72 ± 0.06) p = .001.

Correlation with df of LDL (r = 0.16, p = .046), hct (r = 0.33, p <.001) and fibrinogen (r = 0.18, p = .014).
Baseline Demographics with Mean Values of the Total Population.

Differences in df in Subjects following PPCI for STEMI Acute Coronary Syndrome. All Comparisons Involved the Two-Sample T-Test as All the Data was Shown to be Normally Distributed.

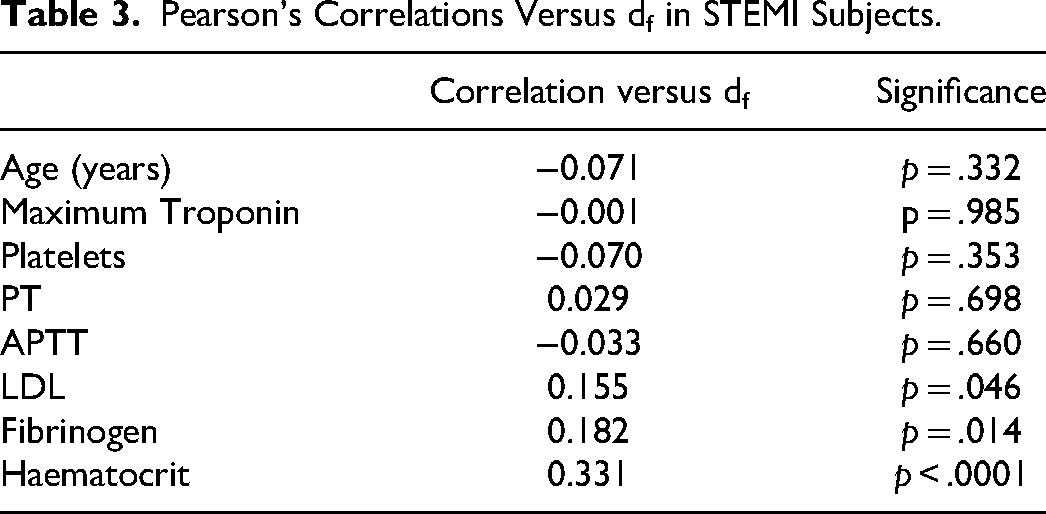
Correlation of continuous variables are shown in Table 3. The strongest correlation with df was with haematocrit (Hct) (r = 0.331, p < .0001). Significant associations with df were also seen with increasing low density lipoprotein (LDL) (r = 0.155, p = .046) and plasma fibrinogen (r = 0.182, p = .014). No significant association was observed with age, platelet count, maximum troponin T or standard coagulation assays (PT and APTT) in our patients.
Pearson's Correlations Versus df in STEMI Subjects.
Multiple Regression Analysis
We further examined the data using Multiple Regression Analysis (Table 4). Only the variables showing significant difference or correlation were fitted in the regression model. This confirmed that df in these STEMI patients was significantly determined after multiple regression analysis from the plasma LDL level, fibrinogen and Hct. Presence of diabetes also significantly influencing df but not the presence of hypertension or a history of previous MI. Male patients had demonstrated significantly higher df than females on univariate analysis but following multiple regression analysis (accounting for the higher haematocrit levels in males, 0.43 ± 0.04 than females, 0.39 ± 0.05, p = .014) gender became non-significant. Treatment with Ticagrelor remained associated with a lower df than Clopidogrel after multiple regression analysis. No multicollinearity was observed in this model, as confirmed by the Variance Inflation values. In addition, the adjusted R-square was explored to determine the explanatory power of the model in determining df for this model the value was 29%
Multiple Regression to Determine the Variables and Factors Related to df in Patients with STEMI. VIF Refers to Variance Inflation and was Used to Determine the Absence of Multicollinearity in the Model.

Discussion
Clot Microstructure in Myocardial Infarction
The mechanical structure of the clot and its development plays an important part in the treatment and outcome of myocardial infarction. 7 To date, studies have not investigated clot microstructure using a dynamic technique that measures clot microstructure and mechanical properties in a real time whole blood bedside test. We have shown previously that the df of the incipient clot is higher in patients with coronary artery disease both in stable and acute presentations, reflecting denser clots with abnormal morphology that are mechanically stronger and harder to break down. 9 This present study determined the effect of demographic factors such as gender and age, risk factors such as diabetes and elevated LDL and antiplatelet treatment on the clot microstructure of patients following acute myocardial infarction.
Anti-Platelet Treatment and Clot Microstructure Following Acute Myocardial Infarction
Platelet activation and aggregation plays a key role in acute myocardial infarction and the routine addition of Clopidogrel to Aspirin treatment reduces adverse vascular events and mortality. 11 However, the use of dual anti-platelet therapy does come with an increased risk of bleeding. 12 A significant proportion of patients (up to 25%) undergoing treatment with coronary stenting during acute myocardial infarction do not respond to Clopidogrel and this is associated with adverse outcomes. 13 The P2Y12 inhibitor Ticagrelor has been shown more effective at reducing ischemic events than Clopidogrel. 14 Previously, in healthy subjects we have shown that df could differentiate between different antiplatelet drugs in either mono or dual therapy. 15 In that previous study, Aspirin created a negligible alteration in df, in comparison to P2Y12 inhibitors, which caused more significant reductions in df and clot mass. This study adds to that in showing that patients receiving the combination of Aspirin and Clopidogrel had a higher df than those patients receiving Aspirin and Ticagrelor. The effect on thrombus microstructure that corresponds to the difference in df between the anti-platelet regimes is illustrated in Figure 3. The nonlinear relationship between df and mass means that although a thrombus with a df of 1.71 (mean df in patients treated with Ticagrelor) is numerically only slightly lower than a thrombus with a df of 1.76 (mean df in patients treated with Clopidogrel), the latter incorporates approximately twice the amount of mass. This results in a thrombus with denser microstructure, more likely to be resistant to degradation.

Difference in the amount of normalised mass incorperated into the incipient clot at square (mean df of ticagrelor treatment) and triangle (mean df of clopidgrel treatment).
Patient Characteristics and Fractal Dimension
Consistent with previous work on patients with stable coronary disease, we found age had no effect on df. 10 The standard coagulation screen (PT and APTT) were not correlated with df in this study, however the majority of PT and APTT values were within the normal range as patients still on anticoagulation when the sample was taken were excluded. Components of clot formation and physiological markers haematocrit and fibrinogen were associated with a higher value of df indicating altered mechanical clot properties. Interestingly, increased haematocrit and fibrinogen have been associated with a poor clot contraction process and poorer outcome. 16 Long Ischaemic time before presentation was not associated with increased df. That is in contrast to a previous study that demonstrated the in-situ thrombus become more dense over longer ischaemic times. 6 Our study implies that while formed thrombus becomes more organised over longer ischaemic times, this does not affect the structure of subsequent de-novo thrombus. 17
Risk Factors for Abnormal Clot Microstructure in Myocardial Infarction
Following multi variable regression analysis the established cardiovascular risk factors smoking and hypertension had no effect on df. The effect of smoking is surprising given smoke exposure has previously been shown to increase thrombogenicity if examined immediately. 18 It is worth noting that we analysed df in patients the day following their acute MI when they would have abstained from smoking for at least 12 h. We did find that df was significantly higher in patients with diabetes and correlated significantly with LDL. Thrombus formation is effected by inflammation and oxidative stress. 19 Diabetes is a pro inflammatory and pro thrombotic state. 20 Patients with diabetes are recognised to have higher rates of MI, greater recurrence of MI and stent occlusions and poorer outcomes. 21 Diabetes is known to be associated with thrombus having altered mechanical properties and being more resistant to lysis. 22 This is consistent with the results of the present study, which shows that diabetes was significantly associated with an increased df, and indicates that people with diabetes form larger clots with more incorporated mass. The more potent oral P2Y12 receptor inhibitor, Ticagrelor, has shown increased relative benefits with higher absolute risk reductions in patients with diabetes as compared with Clopidogrel. 23 The near bedside capability of df testing might have potential to be exploited to tailor anti ischaemic therapy in future studies.
In addition to diabetes, abnormal blood lipids are also known to be associated with a higher incidence and recurrence of MI. 24 Hyperlipidaemia is also known to effect coagulation with oxidised LDL causing platelet activation 25 and stimulating tissue factor expression. 26 Targeted LDL reduction with PCSK9 inhibitor has been shown to reduce cardiovascular events. 27 This was corroborated in our study by the significant association between LDL levels and higher df.
Limitations
This study has some limitations that may affect its interpretation. Firstly, no baseline measurement of df was obtained prior to intervention. Due to this, the effect of a patients underlying df on the subsequent response to treatment is not known. Secondly, in this study patients were not randomised to their antiplatelet strategy, rather they were recruited sequentially receiving initially Clopidogrel then Ticagrelor following a change in clinical practice. Although we attempted to adjust for possible confounding factors with multiple regression analysis, in the absence of randomisation, some form of selection bias cannot be ruled out. It is reassuring however that our findings confirmed a lower value of df with Ticagrelor, which is corroborated by our previous work in healthy subjects. 15 Thirdly, df values are known to be influenced acutely by therapeutic anticoagulation in the catheter laboratory. 10 To account for this df values were taken at least 12 h after the last administration of heparin or Bivalirudin to allow any effect to wear off. Finally, this is a single centre study so caution should be employed before generalising any findings. While we found no difference in mortality between Clopidogrel and Ticagrelor usage the study contained relatively small numbers and individual bleeding events were not recorded which should be considered during interpretation given Ticagrelor has been associated with more bleeding than Clopidogrel. 28
Conclusions
In this study, we investigated the role of patient characteristics and the effect of antiplatelet treatment on clot microstructure as determined by the fractal dimension (df) in STEMI patients. Patients with diabetes mellitus and elevated LDL had higher df indicating denser clot. Treatment with Ticagrelor as compared to Clopidogrel resulted in a reduction in df value linked to a looser, less compact clot. This novel biomarker is unique in that it evaluates the overall effect and endpoint of a complex interaction between different drugs and underlying disease states on the clot at a microstructural level. Further randomised controlled studies to investigate the effect of df on subsequent clinical outcomes are required.
Footnotes
Acknowledgements
We would like to acknowledge and thank staff working in the Welsh Centre for Emergency Medicine Research and Morriston Regional Heart Centre, Swansea Bay University Health Board, UK for all for their help in this study.
Author Contributions
PAE conceived, designed and coordinated the study. MJL contributed to concept and design, collected data, performed rheological analysis and critical writing. DRO contributed to concept and design, analysed data and critical writing. AS, RQ, SP and JW recruited the patients, collected blood samples and data. DRO and RHKM performed the statistical analyses and interpreted the data. PRW and KH provided rheological advice. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
This study complied with the declaration of Helsinki and was approved by a local Research Ethics Committee (Wales Research Ethics Committee 6; REC reference number 13/WA/0366). Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Funding
This work was supported by the National Institute for Social Care and Health Research (NISCHR) (grant number BR01)