
Abstract
Background
Direct oral anticoagulants (DOACs) are commonly used to prevent stroke and systemic embolism in patients with atrial fibrillation (AF). However, studies into their effectiveness and safety in the Thai population have so far been limited.
Objectives
To study the effectiveness and safety of warfarin and DOACs among Thai AF patients
Methods
A retrospective cohort study was conducted on AF patients at Ramathibodi Hospital from 2013 to 2018. All patients were followed for at least 1 year. Relevant clinical information was collected and compared between AF patient groups receiving warfarin, dabigatran, rivaroxaban, and apixaban. The primary outcome was a composite of major bleeding, ischemic stroke, and systemic thromboembolism. The secondary outcomes were all-cause mortality and disease-specific mortality caused by major bleeding, ischemic stroke, and systemic thromboembolism.
Results
A total of 1680 AF patients were enrolled in the study (warfarin 1193, apixaban 140, dabigatran 193, rivaroxaban 114). The estimated incidence of composite outcome was 16% [95% CI, 14−18%] and 12.4% [95% CI, 9.4−15.3%] in the warfarin and DOAC group, respectively, given a number needed to treat of 28 [95% CI, 3−52]. Compared with warfarin, DOACs were associated with both lower rate of all-cause mortality (4.9% [22/447] vs 8% [98/1193]) and lower disease-specific mortality (0.4% [2/447] and 1% [12/1193]).
Conclusions
This study suggests DOACs were associated with a lower risk of major bleeding, ischemic stroke, and systemic thromboembolism compared to warfarin in Thai patients with AF. Patients receiving DOAC also had a lower rate of all-cause mortality and disease-specific mortality.
Keywords
Introduction
Direct oral anticoagulants (DOACs) are widely used in atrial fibrillation (AF) patients to prevent stroke and systemic embolism. Several randomized controlled trials1–4 (RCTs) have demonstrated that DOACs are not inferior to warfarin in terms of systemic embolism and stroke prevention and have an equal or less incidence of major bleeding. 5 DOACs are recommended over warfarin 6 because of their fixed-dose effect, less frequent laboratory monitoring, fewer food and drug interactions, and could convey better patient compliance.
In the Asian population, the risk of ischemic stroke is high, particularly stroke in the young. 7 In addition, lower body weight could lead to a different pharmacokinetic profile 8 resulting in a higher rate of major bleeding. 9 Considering that most RCTs were conducted in the Caucasian population, there exists a significant gap in the data on the efficacy and safety of DOACs in Asians. From the meta-analysis of RCTs comparing DOACs to warfarin in AF patients, the subgroup of the Asian population who received DOACs had less stroke or systemic thromboembolism compared with warfarin. 10 Another retrospective cohort study in Taiwan found that rivaroxaban and dabigatran were associated with a reduced risk for ischemic stroke or systemic embolism, intracranial hemorrhage, and all-cause mortality. 11
From the aforementioned studies, DOACs appeared to be effective and safe in the Asian population. DOACs have become more commonly used in Thailand since 2013. A retrospective study in Thai patients on real-world comparison between DOACs and warfarin revealed prominent effectiveness and safety of DOACs over warfarin in patients with poor time in therapeutic range (TTR). 12 In our study, we aimed to further consolidate the evidence of the effectiveness and safety of DOACs in the Thai population, which could provide further insights for clinicians on the rationale of anticoagulant selection.
Methods
Study Design
A list of AF patients who received anticoagulant therapy from January 2013 to December 2018 was retrieved from the hospital database. The first day of an anticoagulant prescription was defined as an index date. Relevant clinical data were collected from the electronic medical records for at least one year afterward. The inclusion criteria were: 1) patients over 18 years of age, 2) confirmed atrial fibrillation, 3) prescription of either warfarin, dabigatran, rivaroxaban, or apixaban, and 4) over one year of follow-up. The exclusion criteria were patients with mechanical heart valve or had moderate to severe mitral stenosis. The primary outcome was the composite of major bleeding defined by ISTH criteria, 13 ischemic stroke, and systemic thromboembolism. The secondary outcomes were all-cause mortality and disease-specific mortality caused by major bleeding, ischemic stroke, and systemic thromboembolism.
Data Collection
The following information was retrieved from the electronic medical records: patient identifications; age; sex; body weight; height; underlying disease(s); CHA₂DS₂-VASc score; HAS-BLED score; history of antiplatelet and NSAID use; type of anticoagulant used; event of major bleeding, stroke, and systemic embolism; death and documented cause. The CHA₂DS₂-VASc and HAS-BLED scores are risk-stratification tools used to identify AF patients at high risk of thromboembolism and major bleeding, respectively. 14
Statistical Analyses
Continuous variables with normal distribution were presented as means and standard deviations. Continuous variables with non-normal distribution were presented as medians and interquartile ranges. Mann-Whitney U test and Student's t-test were employed to compare continuous variables. Categorical variables were presented as percentages and analyzed by Chi-square or Fisher's exact tests.
To balance the confounders between two groups of prescribed anticoagulants (warfarin and DOACs), multiple logistic regression analysis between independent variables (eg, age, gender, CHA₂DS₂-VASc Score, and HAS-BLED Score) and dependent variables (warfarin or DOACs) was performed. The significant variables were put into inverse probability weighting with regression adjustment treatment model. The maximum absolute standardized difference (ASD) of 0.1 (10%) was considered a trivial difference in baseline characteristics. We checked the balance of factors associated with anticoagulant prescription, ie, age, diabetes, and HAS-BLED score, and then estimated the conditional probability by applying the measured weights to each of the anticoagulant group (warfarin and DOACs), resulting in potential outcomes means (PO means). Regarding the PO means, the number needed to treat (NTT) and risk ratio (RR) were calculated. In addition, we performed the analyses for patients with TTR < 65 and TTR ≥ 65 in the warfarin group compared to patients with DOACs. A p-value of < 0.05 was defined as statistically significant. All statistical analyses were performed using the STATA software, version 16.0.
Results
A total of 1640 AF patients were included in the study (warfarin 1,193, apixaban 140, dabigatran 193, rivaroxaban 114) (Figure 1). The median age across all anticoagulant groups was 72 years. The patients were similarly distributed between male and female. The prevalence of most underlying diseases (hypertension, congestive heart failure, history of stroke, history of transient ischemic attack, history of bleeding, peripheral vascular disease, abnormal liver function) were similar in both groups. Diabetes and abnormal renal function were more common in the warfarin group compared to the DOACs group (39.7% vs 31.3% and 6.1% vs 2.2%, respectively). There was no significant difference in the CHA₂DS₂-VASc score (mean [SD]: warfarin 4.0 [1.9], DOACs 3.9 [2.0]) between the two groups. The mean HAS-BLED score was significantly higher in the warfarin group (mean [SD]: warfarin 3.4 [1.5], DOACs 3.1 [1.6]). In the warfarin group, 23.7% (227/1168) of the patients achieved time in therapeutic range (TTR) ≥ 65%. The average TTR (SD) was 40.6% (30.4). Other baseline characteristics are shown in table 1.
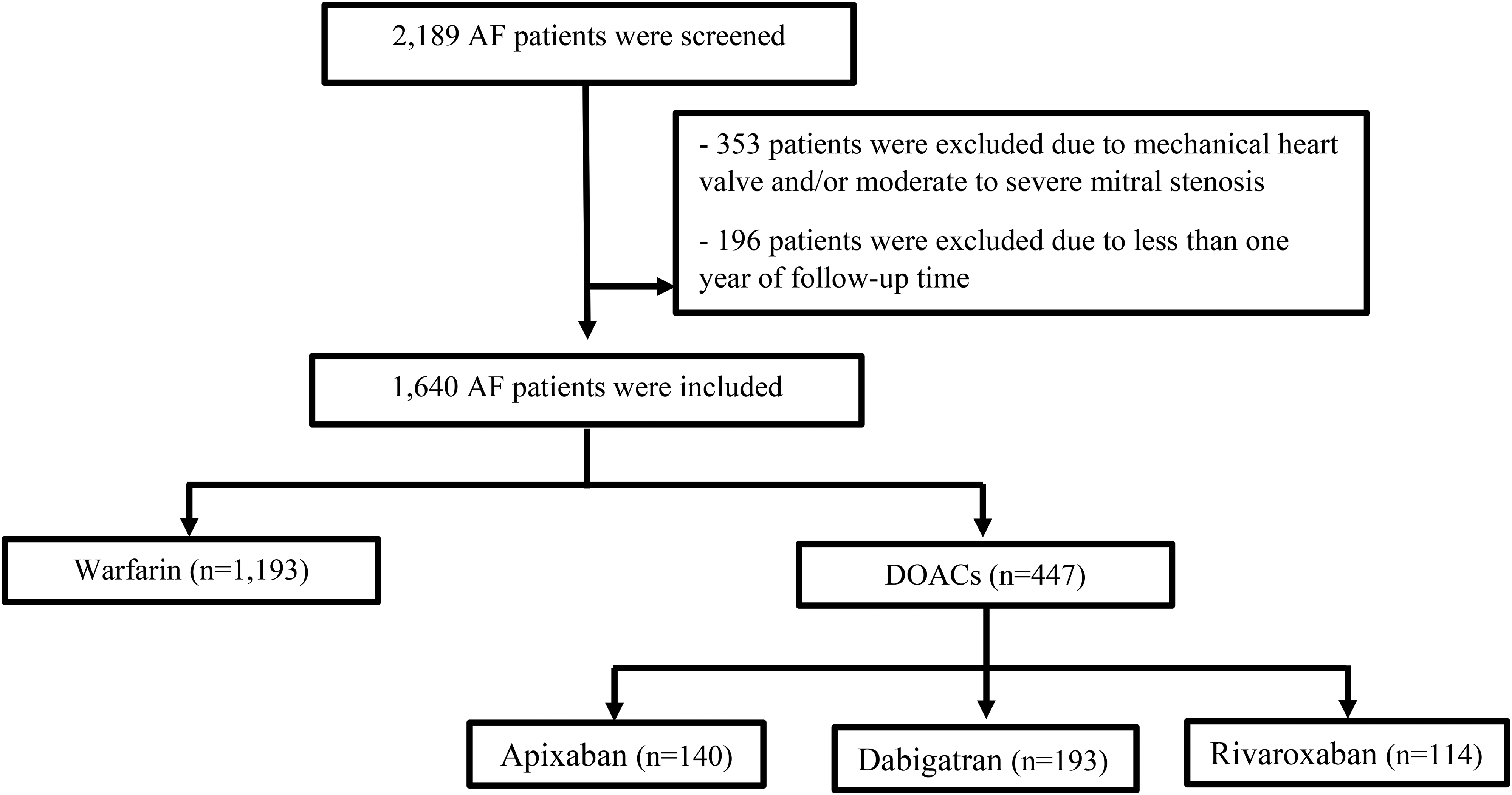
Protocol flow chart.
Baseline Characteristics Between Warfarin, Combined and Separated DOACs Groups.

* Significant difference between the warfarin group and the combined DOACs group.
The composite outcome (major bleeding, ischemic stroke, and systemic thromboembolism combined) occurred in 197 out of 1193 (16.5%) in the warfarin group, and 49 out of 447 (11%) in the combined DOACs group. Separately, the adverse outcome occurred in 27 out of 140 (19.3%) in the apixaban group, 18 out of 193 (9.3%) in the dabigatran group, and 4 out of 114 (3.5%) in the rivaroxaban group.
The incidence of each item forming the composite outcome in warfarin and DOAC groups was as follows: major bleeding 118/1193 (9.9%) versus 25/447 (5.6%) [apixaban 14/140 (10%), dabigatran 8/193 (4.1%), rivaroxaban 3/114 (2.6%)]; ischemic stroke, 116/1193 (9.7%) versus 30/447 (6.7%) [apixaban 19/140 (13.6%), dabigatran 11/193 (5.7%), rivaroxaban 0/114 (0%)]; systemic thromboembolism 24/1193 (2%) versus 4/447 (0.9%) [apixaban 1/140 (0.7%), dabigatran 1/193 (0.5%), rivaroxaban 2/114 (1.8%)].
The all-cause mortality of the study was 98 out of 1193 (8%) in the warfarin group and 22 out of 447 (4.9%) in the DOACs group. The disease-specific mortality was 12 out of 1193 (1%) in the warfarin group and 2 out of 447 (0.4%) in the DOACs group. Death from other causes was 83 out of 1193 (7%) in the warfarin group and 10 out of 447 (7.1%) in the DOACs group (table 2).
Outcomes Between Warfarin, Combined and Separated DOACs Groups.
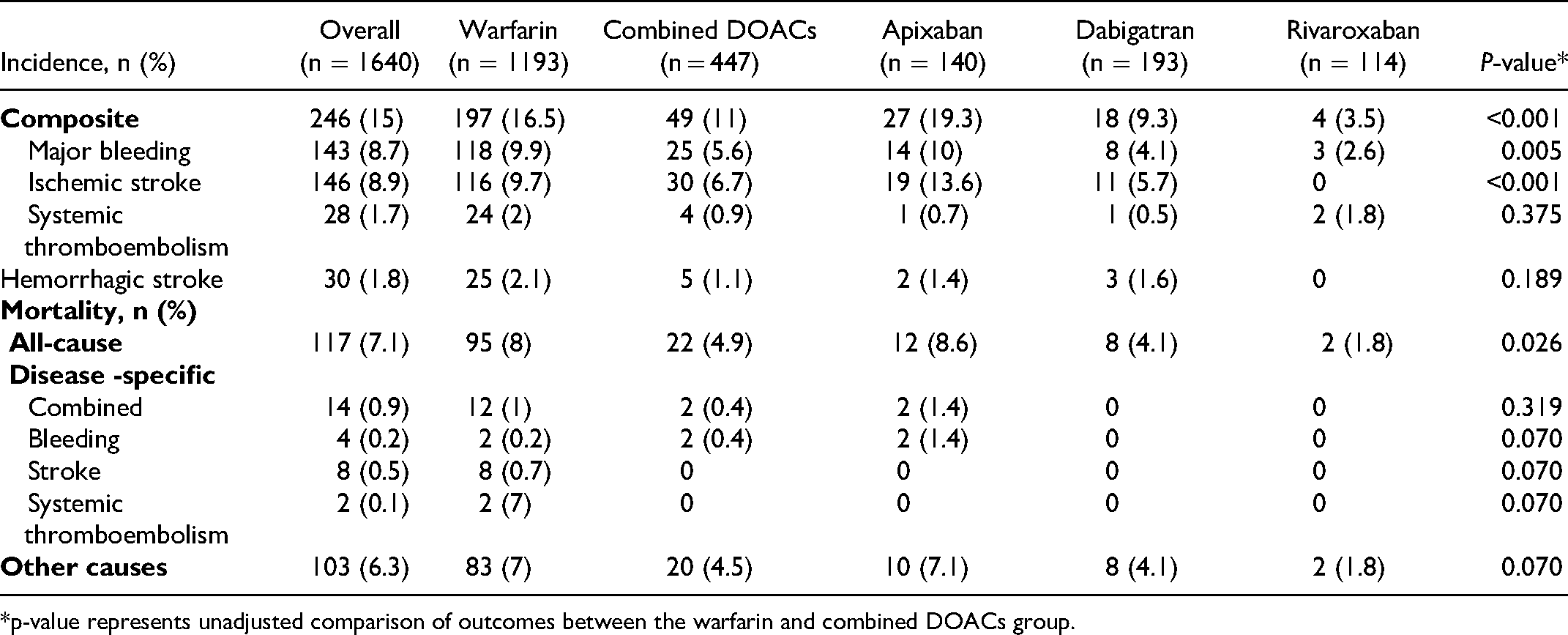
*p-value represents unadjusted comparison of outcomes between the warfarin and combined DOACs group.
Treatment effects estimation using inverse probability weighting with regression adjustment were presented in the form of potential outcome means and average treatment effect. Univariate logistic regression using the prescription of DOACs versus warfarin as a dependent variable revealed that age, diabetes, abnormal renal function, and the HASBLED score were the significant independent variables. However, a multivariate logistic regression demonstrated that only age, diabetes, and the HASBLED score were significant covariates. The balance of covariates affecting anticoagulant prescription is shown in table 3. The potential outcome means represented the estimated incidence rate of the composite outcome. Warfarin group had the potential outcome means (estimated incidence rate of composite outcome) of 16.0% (95% confidence interval [CI], 14.0–18.0%), compared to 12.4% (95% CI 9.4–15.3%) of the DOACs group. The average treatment effect was the subtraction of potential outcome means of DOACs from potential outcome means of warfarin. Patients who received DOACs would have the probability of composite outcome incidence lower than those who received warfarin by 3.7% (95% CI, 0.3–7.1%) (Table 4). The number needed to treat (NTT) in the DOACs group was 28 (95% CI, 3–52). The risk ratio (RR) comparing between the DOACs and warfarin groups was 0.77 (95% CI, 0.57 −0.97), p = 0.02 (table 5).
Balance of Factors Associated with Anticoagulant Prescription (DOACs or Warfarin).

Estimation of Effects of Anticoagulant Prescription Applying Treatment Effect Model by Inverse Probability Weighting with Regression Adjustment.

The Number Needed to Treat (NTT) for DOACs and Risk Ratio (RR) Comparing between the DOACs and Warfarin Groups.

Comparing the composite outcome of DOACs and warfarin with TTR < 65%, there was a significantly lower potential outcome mean in the DOACs group. The estimated incidence rate of the composite outcome was 16.9% [95% CI, 14.6−19.2%] in the warfarin group versus 12.4% [95% CI, 9.4 −15.4%] in the DOACs group. Patients who received DOACs had the probability of composite outcome incidence lower than those who received warfarin at 4.5% [95% CI, 0.9−8.1%] (NNT = 23 [95% CI, 5−41]). The RR between DOACs and warfarin groups was 0.74 [95% CI, 0.54−0.93; p = 0.008]. However, in warfarin patients with TTR ≥ 65, there was no significant difference in the estimated incidence rate of the composite outcome (warfarin 13.7% [95% CI, 10.1−17.2%], DOACs 11.7% [95% CI, 8.8−14.6%], p = 0.38).
Discussion
We conducted a retrospective cohort study on the effectiveness and safety of DOACs compared to warfarin among Thai AF patients in a real-world setting. Our study differs from previous RCTs in that many Thai AF patients switched from warfarin to DOACs, rather than receiving DOACs as the initial anticoagulant therapy. We found a consistent result that DOACs have a preferable effectiveness and safety profile compared to warfarin, especially if the TTR was less than 65%.
From the baseline characteristics, the populations in both warfarin and DOACs groups were at high risk for thromboembolic events. The mean CHA₂DS₂-VASc score in our study was 4.0 (The score ≥ 2 is considered high risk, suggesting that anticoagulants should be administered). The average score in our study was higher than the studies of the Thailand-AF registry 15 (mean 3.3) and Taiwan's National Health Insurance Research Database 16 (mean 3.6). This was likely affected by the case severity of enrolled in-patients since the Thailand-AF study excluded hospitalized patients. There was no mention of in-patients in the latter study.
The overall incidence of ischemic stroke, systemic thromboembolism, and major bleeding was significantly higher in the warfarin group, suggesting the desirable benefits of DOACs. Interestingly, among DOACs, apixaban had the highest incidence of major bleeding and ischemic stroke. Although the CHA₂DS₂-VASc and the HAS-BLED scores were not statistically different from those who received other DOACs, the means of both scores were slightly higher. This could explain the higher rates of major bleeding and ischemic stroke in the apixaban group. This was in contrast to the study on Japanese administrative claims data 17 that apixaban harbored the lowest risk of any bleeding. The majority of the patients in the Japanese study (47.2-76.2%) were prescribed reduced doses of DOACs, which could confound the direct comparison of bleeding risk with our study.
In comparison to Korean National Health Insurance Service claims database 18 and Japanese administrative claims data 17 studies, DOACs were related to lower risks of composite outcome among all types of DOACs. Nonetheless, the average TTR of warfarin in the Korean study was 49%. Direct evaluations between each type of DOACs and different TTR range were not reported.
The quality monitoring of warfarin was the TTR, which was essentially suboptimal in Thai patients, ensuing increased risks of ischemic stroke/TIA, major bleeding, ICH, and death. 15 Only 23.7% of the patients in the warfarin group were able to achieve a TTR of ≥ 65%. Compared to the Thailand-AF registry study, 15 its average TTR was 53.6 ± 26.4%, and 35.9% of the patients had TTR ≥ 65%. One of the plausible reasons for lower-than-desirable TTR in Thai patients could stem from the idea that Asian populations are more prone to bleeding 12 and are targeted for lower INR levels. Other reasons could be factors that were not previously mentioned such as food and drug interactions.
Although DOACs are recommended as the first-line treatment in the prevention of stroke in AF patients, 6 warfarin is the mainstay of anticoagulant treatment in Thailand. 19 Warfarin is inexpensive and can be reimbursed under the national universal health coverage scheme. Our study demonstrated that in patients receiving warfarin with TTR of ≥ 65%, the composite outcome was not significantly different from those receiving DOACs. This result was consistent with a previous study on Thai AF patients in which the favorable effects of DOACs were demonstrated when compared to warfarin with poor TTR.
The strength of our study is that it was an application of real-world data and the balancing method by inverse probability weighting propensity score approach. We retrieved a list of all consecutive patients with atrial fibrillation who had been on anticoagulant therapy. All outcomes were reviewed and verified.
The study also has limitations. The data was limited due to its retrospective nature. The sample size was lower than expected, which could result in insufficient power to detect the differences between groups. Despite the statistical adjustment by applying inverse probability weighting with regression adjustment treatment model, the effect of unmeasured confounding factors could remain. The study was limited to one tertiary-level institution and may not represent the majority of the hospitals in Thailand, due to the difference in levels of care. Because this study was completed in the form of as-treated analysis, the patients who switched between different anticoagulants might possess residual effects of prior anticoagulants or could be confounded by the continuing progression of the disease.
Conclusion
DOACs demonstrated a promising result in reducing the composite outcome of major bleeding, ischemic stroke, and systemic thromboembolism compared to warfarin. Further cost-effectiveness analysis should yield more robust data toward optimal anticoagulant decisions among Thai patients with atrial fibrillation.
Footnotes
Acknowledgments
The author would like to acknowledge Professor Ammarin Thakkinstian and Ms. Sukanya Siriyotha of the Department of Clinical Epidemiology and Biostatistics, Faculty of Medicine Ramathibodi Hospital, Mahidol University for their kind support in treatment effect model analyses.
Authors’ Contributions
S.S., K.B, K.L, A.U, P.V, O.P designed the method of study. S.S, K.B led the study, analyzed the data, and wrote the manuscript. P.N, K.B performed the statistical analyses. M.A retrieved data from the hospital database. K.B., P.A critically revised the manuscript.
Availability of Supporting Data
Not applicable
Consent for Publication
The author and co-authors give our consent for publication of the manuscript to be published in the Clinical and Applied Thrombosis/Hemostasis.
Competing Interests
The author and co-authors declared no potential conflicts of interest.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
This study obtained ethical approval from the Ethics Committee of Faculty of Medicine Ramathibodi Hospital, Mahidol University, Thailand.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article