
Abstract
Background
The association between coronavirus infection 2019 (COVID-19) and thrombosis has been explicitly shown through numerous reports that demonstrate high rates of thrombotic complications in infected patients. Recently, much evidence has shown that patients who survived COVID-19 might have a high thrombotic risk after hospital discharge. This current systematic review and meta-analysis was conducted to better understand the incidence of thrombosis, bleeding, and mortality rates among patients discharged after COVID-19 hospitalization.
Methods
Using a search strategy that included terms for postdischarge, thrombosis, and COVID-19, 2 investigators independently searched for published articles indexed in the MEDLINE, Embase, and Scopus databases that were published before August 2021. Pooled incidences and 95% confidence intervals were calculated using the DerSimonian-Laird random-effects model with a double arcsine transformation.
Results
Twenty articles were included in the meta-analysis. They provided a total of 19 461 patients discharged after COVID-19 hospitalization. The weighted pooled incidence of overall thrombosis among the patients was 1.3% (95 CI, 0. 6-2; I2 90.5), with a pooled incidence of venous thrombosis of 0.7% (95 CI, 0. 4-1; I2 73.9) and a pooled incidence of arterial thrombosis of 0.6% (95 CI, 0. 2-1; I2 88.1). The weighted pooled incidences of bleeding and mortality were 0.9% (95 CI, 0. 1-1.9; I2 95.1) and 2.8% (95 CI, 0. 6-5; I2 98.2
Conclusions
The incidences of thrombosis and bleeding in patients discharged after COVID-19 hospitalization are comparable to those of medically ill patients.
Background
Hospitalization for medical illness is one of the strongest risk factors for venous thromboembolism (VTE), 1 and the risk of developing this condition may persist after discharge from the hospital. 2 Risk factors consist of determinants related to the patients and their acquired medical problems. 3 All patients who undergo total knee or hip replacement and general surgery are at risk of VTE, not only during the admission period but also after discharge.4,5 Therefore, standard recommendations for post-discharge VTE prophylaxis have been established for these patients.6,7 However, acutely ill medical patients have a variety of risks of VTE, and the use of an inpatient VTE prophylaxis is often considered for patients with moderate to high-risk features. 8 Evidence demonstrated that the high risk of VTE continued into the post-discharge period.2,9 Therefore, several studies were conducted to establish the benefits of using extended thromboprophylaxis. Although the efficacy endpoint showed promising results, a net benefit was not achieved due to an increase in the number of major bleeding events.10-13
After the outbreak of coronavirus disease 2019 (COVID-19) in December 2019, it soon became apparent that thrombotic complications were clearly associated with patients infected with COVID-19, especially those admitted to intensive care units (ICUs). 14 Nopp et al. showed that the prevalence of overall VTE in 33 970 Covid-19 patients was 14.1% (95% CI, 11.6-16.9). 15 The prevalence of VTE was markedly more common in the ICU than in the non-ICU settings, with a rate of 22.7% (95% CI, 18.1-27.6) and 7.9% (95% CI, 5.1-11.2), respectively. 15 Several mechanisms have been postulated to explain the prothrombotic states found in these patients. 16 Endothelial activation, immune thrombosis, complement pathway activation, and decreased fibrinolytic activity are considered to be partly responsible for the high tendency for Covid-19 patients to develop VTE.17-20 Regarding the high risk of VTE in COVID-19 patients, many guidelines recommend the implementation of a thromboprophylaxis protocol for hospitalized patients.21-24 Furthermore, there is evidence that patients who survived COVID-19 might have persistent symptoms or long-term complications involving many organ systems.25,26 The term “post-COVID-19 syndrome” has been introduced to describe persistent symptoms or abnormalities that occur more than 4 weeks after a patient developed a COVID-19 infection. 27 The hematological consequences are thrombotic complications, which have been demonstrated by case reports describing pulmonary embolism after hospital discharge of infected patients.28-30 Although patients with COVID-19 may have a postdischarge thrombotic risk, there is currently no definitive recommendation for the administration of postdischarge VTE prophylaxis.22-24 A factor in support of using an extended phase of anticoagulants after discharge is the scarcity of reports of postdischarge thrombotic events. Another critical issue with regard to thromboprophylaxis is the uncertain incidence of bleeding complications arising from an extended duration of prophylaxis. Many recent studies from a large number of countries have reported a range of rates of venous and arterial thromboembolism after hospitalization for COVID-19.31-50 Furthermore, these studies employed a wide array of thrombo-prophylactic strategies.31-50 The present systematic review and meta-analysis was conducted to gather all published incidences of postdischarge thrombotic and bleeding events, as well as all-cause mortality, after hospital discharge of COVID-19 patients.
Methods
Data Sources and Searches
Two investigators (T.R.1 and N.S.) independently searched for published articles in the databases of MEDLINE, Embase, and Scopus using a search strategy employing the terms postdischarge, thromboembolism, bleeding, and COVID-19. The search strategy is available as
Supplementary Data 1
. The references of the selected studies were manually reviewed by the 2 investigators to identify any additional eligible studies. The systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guideline
Selection Criteria and Data Extraction
To be eligible for inclusion, a study could be a cohort (either retrospective or prospective) or case-control study. The primary outcome of this meta-analysis was the incidence of postdischarge thrombotic events after hospitalization for COVID-19. Secondary outcomes were bleeding events and mortality rates after hospital discharge. The inclusion criteria did not specify the thrombotic rates of the subgroups (patients with anticoagulant prophylaxis, patients without anticoagulant prophylaxis, patients recently admitted to an ICU, and patients admitted to non-ICU settings). However, if available, these data were extracted from the included studies for additional analyses. The venous and arterial sites of the thromboses were also collected. Both investigators (T.R.1 and N.S.) separately evaluated the included studies. If there was a disagreement about the eligibility of an article, it was jointly reviewed with a third investigator (W.O. ) until consensus was achieved. The Newcastle-Ottawa Scale was used to assess the quality of the included studies. 52
The two investigators (T.R.1 and N.S.) also separately examined the baseline characteristics and outcomes of the included studies using a standardized data extraction form. The extracted data were cross-checked to endorse the accuracy of the information.
Statistical Analysis
This meta-analysis was performed with OpenMetaAnalyst for Windows 8 and Review Manager 5.4 software from the Cochrane Collaboration (London, UK). 53 The main analysis was the pooled incidence and the associated 95 confidence interval (CI) of thrombosis among COVID-19 patients after discharge. The incidence was calculated using the Dersimonian-Laird random-effects model with double arcsine transformation. 54 Secondary outcomes were calculated with the same technique, including the pooled bleeding and mortality rates of the patients with COVID-19 after discharge. Comparative analyses of the odds of thrombosis among specific groups of postdischarge COVID-19 patients were also performed using the Mantel–Haenszel method. 55 The specific groups were patients receiving anticoagulant prophylaxis, patients without anticoagulant prophylaxis, and patients admitted to the ICU and non-ICU settings. The random-effects model was utilized. This was because heterogeneity between the studies was suspected to be high due to noticeable differences in their background characteristics. The Cochran Q test was calculated, and the I2 statistic was used to estimate the level of heterogeneity between the studies. I2 values were classified as follows: 0-25 indicated insignificant heterogeneity; 26-50, low heterogeneity; 51-75, moderate heterogeneity; and greater than 75, high heterogeneity. 56 Meta-Essentials is used for the calculation of Egger regression and Begg's test to detect publication bias. 57
Results
The detailed process of the search strategy and the screening process is depicted in Figure 1. A total of 1025 articles (518 from EMBASE, 378 from MEDLINE, and 129 from SCOPUS) were identified. Initially, 248 duplicated articles were excluded. The titles and abstracts of the remaining 777 articles were reviewed, resulting in the further exclusion of 746 articles for the following reasons: (1) ineligible article type (case report, review, meta-analysis, or comments); (2) the studies did not report the primary outcome of postdischarge thrombotic events; and (3) the studies contained insufficient data. The remaining 31 articles underwent a full review, and 11 were excluded for the same reasons as in the first round. Finally, a total of 20 studies (7 prospective cohort studies, 12 retrospective cohort studies, and 1 case-control study) were enrolled.31-50

Flowchart of literature review process.
Baseline Patient Characteristics
A total of 19 461 patients who were discharged after COVID-19 hospitalization from 20 articles were included in this systematic review and meta-analysis. Of these, 5323 were female and 6833 were male.31,32,34,37-39,41-46,49,50 In total, 1354 patients were admitted to an ICU while 11 083 were admitted to non-ICU settings.32-37,41-43,46,47,50 A total of 659 of 9424 patients (7%) received thromboprophylaxis after hospitalization.31-37,40,42,47,50 However, not all studies provided the details of their enrolled participants. The incidence of thrombosis was reported by 20 studies,31-50 while the incidence of bleeding was reported by 5.34,36,37,40,46 In addition, 5 studies reported mortality rates.36,40,42,46,47 Table 1 summarizes the characteristics and participants of the included studies.
Baseline patient characteristics of the included studies.

Study provided two admitted cohorts.
Abbreviations: C, comparability; Ca, case control study; CRNMB, clinically relevant non-major bleeding; E, exposure; F, female; M, male; N/A, not available; O, outcome; P, prospective cohort study; R, retrospective cohort study; S, selection; UK, United Kingdom; USA, United States of America
Overall Thrombotic Incidence in Patients with COVID-19 After Discharge
The pooled weighted incidence of overall thrombosis (either arterial or venous) among the discharged patients was 1.3% (95 CI, 0. 6-2; I2 90.5; Figure 2).31-50 The respective pooled weighted incidences of venous and arterial thromboses (Figure 3) were 0.7% (95 CI, 0. 4-1; I2 73.9)31-50 and 0.6% (95 CI, 0. 2-1; I2 88.1).31-34,37,38-40,42-44,46,47,49 The sites of the thromboses are detailed in Table 2.

Forest plot of pooled incidence and 95 confidence interval of overall thrombosis in patients after discharge from COVID-19.
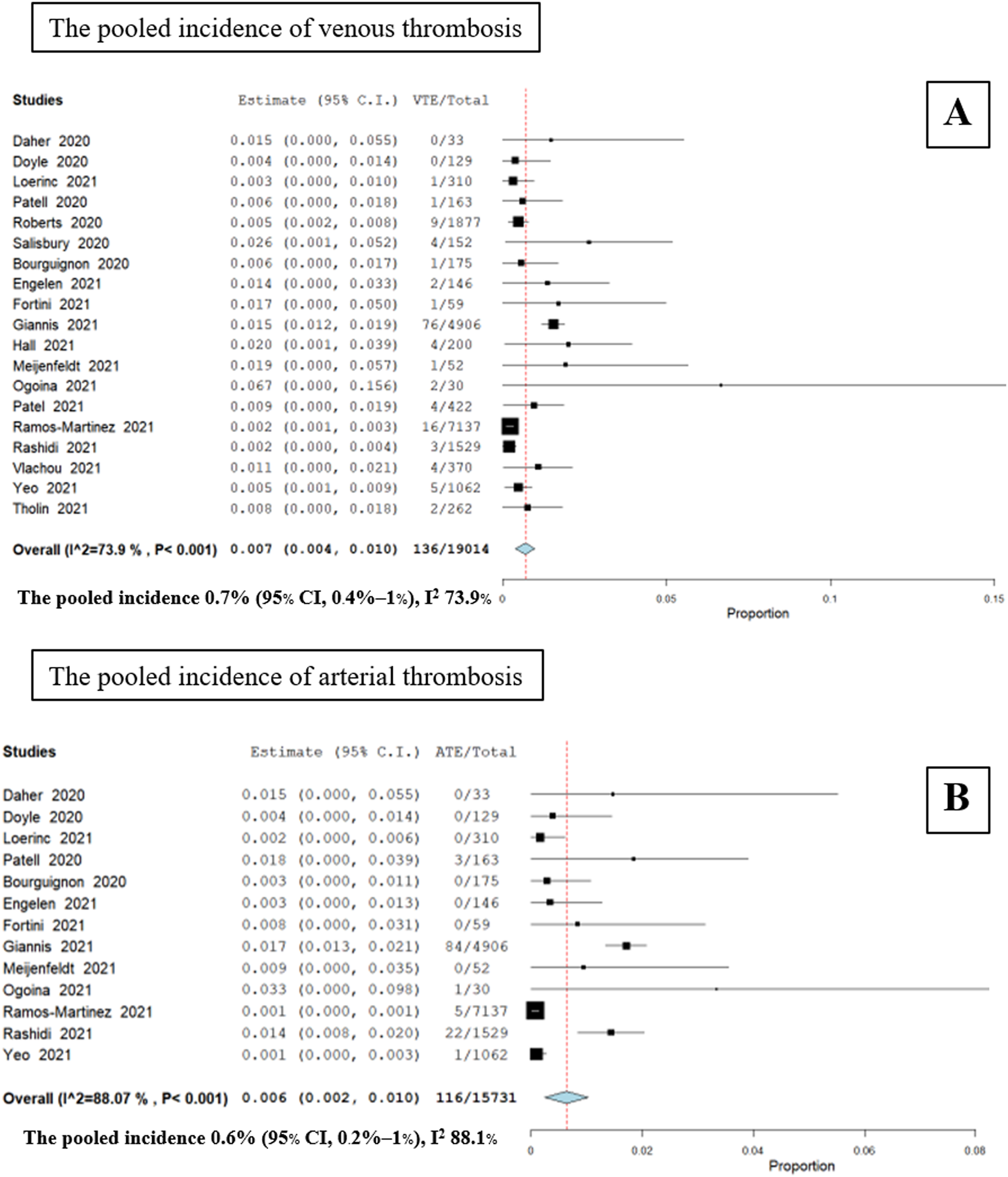
Forest plot of pooled incidence and 95 confidence interval of A) venous thrombosis and B) arterial thrombosis in patients after discharge from COVID-19.
Site of thrombosis and bleeding in each study.

Abbreviations: CRAO, central retinal arterial occlusion; N/A, not available.
The pooled weighted incidences of thrombotic outcomes in COVID-19 patients after discharge without thromboprophylaxis (Figure 4) were as follows: overall thrombosis, 1.1% (95 CI, 0. 4-1.7; I2 26.3);31-33,43,47 venous thrombosis, 0.3% (95 CI, 0. 1-0.5; I2 0);31-33,35,43,47 and arterial thrombosis, 0.8% (95 CI, 0. 2-1.5; I2 38.1)

Forest plot of pooled incidence and 95 confidence interval of A) overall thrombosis, B) venous thrombosis, and C) arterial thrombosis in patients after discharge from COVID-19 without extended thromboprophylaxis.
Bleeding Incidence and Mortality Rate in Patients with COVID-19 After Discharge
The pooled weighted incidence of overall bleeding (either major or clinically relevant nonmajor bleeding) among the patients was 0.9% (95 CI, 0. 1-1.9; I2 95.1; Figure 5A).34,36,37,40,46 The bleeding sites are listed in Table 2. The pooled weighted incidence of mortality in the patients was 2.8% (95 CI, 0. 6-5; I2 98.2; Figure 5B).36,40,42,46,47
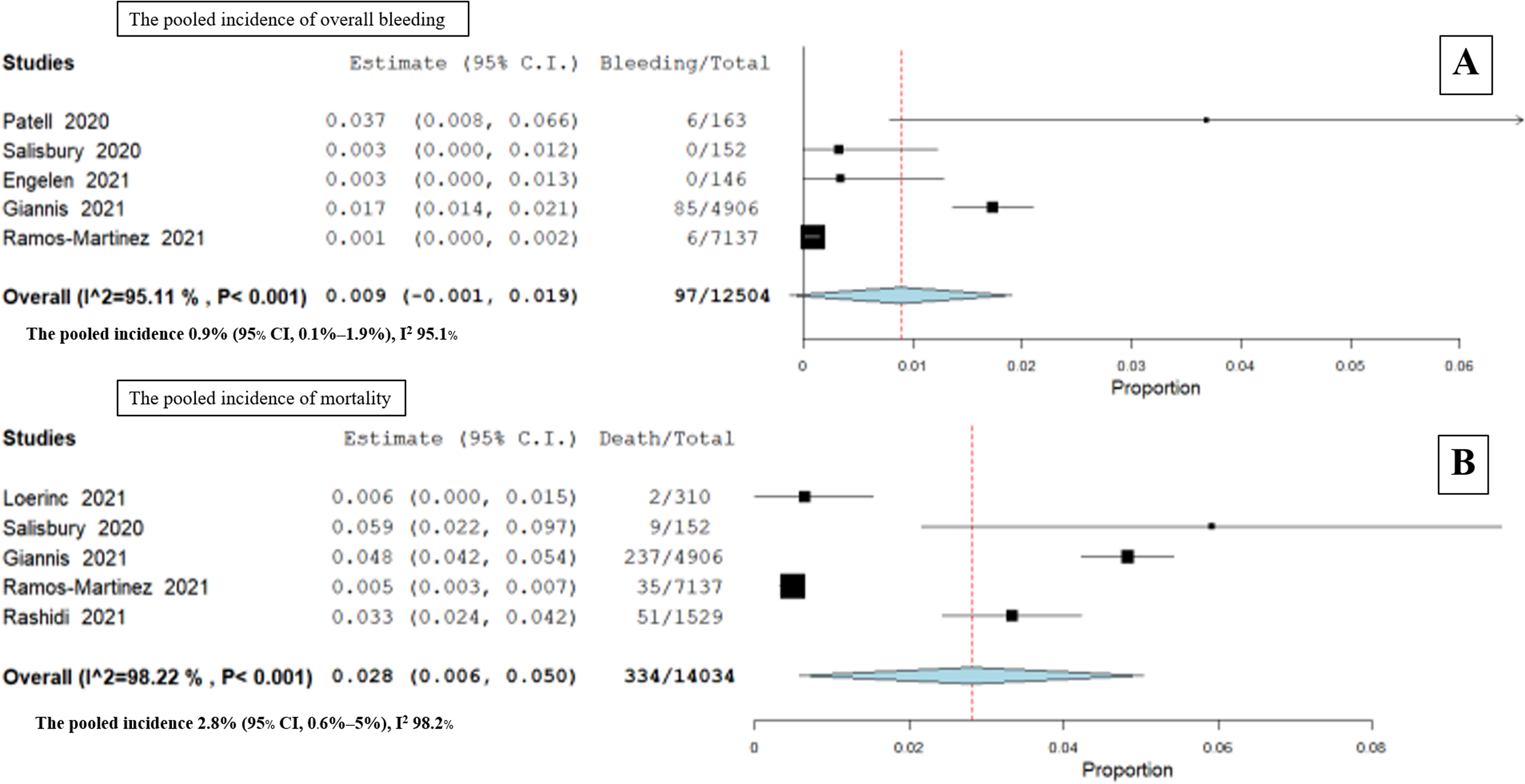
Forest plot of pooled incidence and 95 confidence interval of A) bleeding, B) all-cause mortality in patients after discharge from COVID-19.
Tables 3 and 4, respectively, show the pooled unweighted and weighted incidences of all outcomes related to the overall population and to the patients who did not undergo thromboprophylaxis after discharge.
The pooled incidence of outcomes among COVID-19 patients after discharge
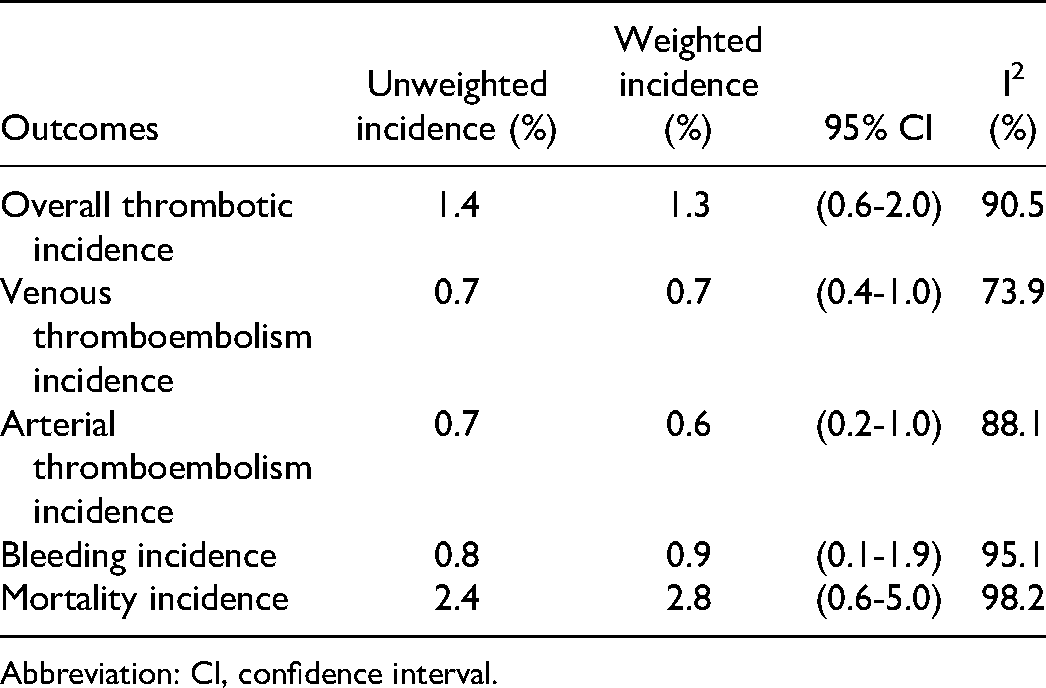
Abbreviation: CI, confidence interval.
The pooled incidence of outcomes among COVID-19 patients after discharge without thromboprophylaxis.

Abbreviation: CI, confidence interval.
Meta-Regression of Other Factors That may Affect Outcomes
Because conducting meta-regression using OpenMeta does not yield the correlation coefficient, Meta-Essentials was used for the calculation of the correlation coefficient.
57
The meta-regression was shown in
Supplementary data 3
Comparing VTE Incidences in Patients Based on Special Conditions
We compared the thrombotic events of patients with and without thromboprophylaxis after discharge. Pooled incidence thrombosis did not differ between the 2 groups, with a pooled OR of 0.84 (95% CI, 0.26-2.70; P = .76; I2 = 0%; Figure 6A).34,37,38,42

Forest plot of studies that compared (A) thrombosis in patients with and without post-discharge thromboprophylaxis, (B) thrombosis in patients in ICU and non-ICU hospitalization settings.
In addition, the thrombotic incidences of patients admitted to ICU and non-ICU settings were also performed. The pooled incidence of postdischarge thrombosis was not significantly higher among patients who had been admitted to an ICU during their hospitalization for COVID-19, with a pooled OR of 1.87 (95% CI, 0.63-5.61; P = .26; I2 = 0%; Figure 6B)
Subgroup Analysis Thrombotic Incidences Based on Rates of ICU Admission among Studies
To search for the thrombosis events influenced by ICU admission, we analyzed the incidence of thrombosis by stratifying studies based on the number of patients who were not admitted to ICU. The studies that had non-ICU patients below 20% was 1 study,
33
20 to 80% were 5 studies,34,37,38,41,42 and more than 80% were 4 studies.32,43,46,47 The thrombotic outcomes of subgroup analysis were shown in
Supplementary data 4
Publication Bias
The calculation of Egger regression and Begg's test showed no publication bias in this study. The P-value was 0.440 and 0.857, respectively. The funnel plot was shown in
Supplementary data 5
Discussion
The emerging consequences for patients who survive a COVID-19 infection are increasingly being recognized and have the potential to become a global health burden in the near future. 58 Survivors of this pandemic generally have persistent symptoms, such as fatigue, breathlessness, and myalgia.26,59 The term post-COVID-19 syndrome has been introduced to describe the late complications experienced by patients after their recovery from infection. 27 Direct viral toxicity and immune dysregulation can cause different sequelae in different organ systems. 60 Postdischarge thromboembolism is the hematological manifestation, of which hypercoagulability is the crucial pathogenesis of venous and arterial thromboses. 27 Von Meijenfeldt et al. demonstrated that Factor VIII and plasminogen activator inhibitor levels in COVID-19 patients 4 months after discharge were statistically higher than those of normal volunteers. 43 Furthermore, a global hemostatic test demonstrated that both the endogenous thrombin potential and the maximum value of thrombin generation assays performed 4 months after discharge were constantly higher than those of patients during admission and healthy controls. 43 During active infection, a high level of D-dimer represents the prothrombotic state in COVID-19 patients and correlates with the severity of the disease.61,62 Furthermore, a study found persistently elevated d-dimer levels (more than 500 ng/mL) for up to 4 months in patients recovering from COVID-19, while other coagulation and inflammatory markers had returned to normal levels during the convalescent phase. 63
Our pooled analysis revealed that the overall, venous, and arterial thrombotic incidence rates were 1.3%, 0.7%, and 0.6%, respectively. However, the overall incidence rate of individual studies varied considerably, ranging from 0.6% to 2.0%. The variation in overall rates can be explained by differences in follow-up periods, initial symptoms of thrombosis, and protocols of thromboprophylaxis employed by the included studies. Giannis et al. reported a protective effect of extended thromboprophylaxis, with an OR of 0.54 (95% CI, 0.47-0.81). 40 However, our work found comparable incidences of thrombosis among the patients with and without extended thromboprophylaxis, with an OR of 0.84 (95% CI, 0.26-2.70; P = .76). Furthermore, Giannis and colleagues found that patients admitted to the ICU had a higher incidence of thrombosis, with an OR of 2.22 (95% CI, 1.78-2.93). 40 In contrast, while our data showed a trend towards a higher proportion of VTE events, there was no statistically significant difference between the ICU and non-ICU patient groups.
Moving on to the rate of VTE, a previous study reported an incidence rate of 1% for overall symptomatic VTE among medically ill patients after discharge. 64 Although the study found that the incidence rate of VTE during the admission period of COVID-19 patients was higher than that of other medically ill patients, our analysis showed that these 2 groups had similar post-discharge VTE rates (Figure 7). In contrast, the incidences of postdischarge VTE reported by Shaikh and Sobieraj were higher for post-major-orthopedic and non-orthopedic surgery compared to our data (Figure 7).65,66 Therefore, several guidelines for VTE prophylaxis suggest the use of an extended duration of thromboprophylaxis in these 2 high-risk settings.6,7,67

Incidence of postdischarge venous thromboembolism of each patient condition.
In terms of bleeding, our study demonstrated that the incidence was 0.9%, while that of patients without COVID-19 was previously reported to be 0.5%. 64 Incidences ranging from 0.2% to 1.1% were found for major hemorrhage among medically ill patients who received extended thromboprophylaxis with enoxaparin or direct anticoagulants.10,11,13 Unfortunately, there were insufficient articles to determine the incidence of major bleeding among patients who received extended prophylaxis. The overall mortality rate of COVID-19 patients after discharge from our study was 2.8%.
Our systematic review and meta-analysis is the first to demonstrate all incidences of thrombosis, including arterial and venous sites, bleeding, and mortality rate, among postdischarge COVID-19 patients. However, the benefits of administering extended prophylaxis are dubious. The decision to do so should be weighed against the risk of bleeding for individual patients. The ongoing trials addressing this research question are warranted (NCT04640181 and NCT04416048).
There are several limitations to our study. First, the patients included in the study had different baseline characteristics. The number of patients admitted to the ICU, the number of patients receiving postdischarge thromboprophylaxis, and the duration of anticoagulant administration were the significant variable factors. Second, the small number of events in the subgroup analysis could have affected the statistical demonstration of the outcome. Third, not all studies provided baseline information on their enrolled patients. Fourth, despite the results of this study, we are still unable to explain the cause of bleeding and the association with thrombosis and mortality in this group of patients. Fifth, the high degree of heterogeneity in our study was caused by factors such as admission to the ICU and extended thromboprophylaxis, which was demonstrated by meta-regression. Sixth, the possible causes of publication bias displayed by the funnel plot are suspected from a high degree of heterogeneity among eligible studies and lacking data of patients in Asian countries. The previous studies described venous thrombotic incidence in the Asian population had lower rates compared to the western population because of a lower proportion of inherited thrombophilia.
68
Finally, in the absence of patients with other medical diseases as a control group, our study is a descriptive analysis that reveals the incidences of thrombosis, bleeding, and mortality in a single group of patients.
Conclusions
The incidences of thrombosis and bleeding in patients with COVID-19 after discharge were comparable with those of other medical conditions. The benefits of extended thromboprophylaxis during the convalescent phase remain controversial. Until the results of ongoing studies are available, the decision to employ extended thromboprophylaxis should be made by weighing the perceived benefits against the risk of bleeding on a case-by-case basis.
Supplemental Material
sj-docx-1-cath-10.1177_10760296211069082 - Supplemental material for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cath-10.1177_10760296211069082 for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis by Tarinee Rungjirajittranon, Weerapat Owattanapanich, Nattawut Leelakanok, Natthaporn Sasijareonrat, Bundarika Suwanawiboon, Yingyong Chinthammitr and Theera Ruchutrakool in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-2-cath-10.1177_10760296211069082 - Supplemental material for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-cath-10.1177_10760296211069082 for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis by Tarinee Rungjirajittranon, Weerapat Owattanapanich, Nattawut Leelakanok, Natthaporn Sasijareonrat, Bundarika Suwanawiboon, Yingyong Chinthammitr and Theera Ruchutrakool in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-3-cath-10.1177_10760296211069082 - Supplemental material for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-cath-10.1177_10760296211069082 for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis by Tarinee Rungjirajittranon, Weerapat Owattanapanich, Nattawut Leelakanok, Natthaporn Sasijareonrat, Bundarika Suwanawiboon, Yingyong Chinthammitr and Theera Ruchutrakool in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-4-cath-10.1177_10760296211069082 - Supplemental material for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-cath-10.1177_10760296211069082 for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis by Tarinee Rungjirajittranon, Weerapat Owattanapanich, Nattawut Leelakanok, Natthaporn Sasijareonrat, Bundarika Suwanawiboon, Yingyong Chinthammitr and Theera Ruchutrakool in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-5-cath-10.1177_10760296211069082 - Supplemental material for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-5-cath-10.1177_10760296211069082 for Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis by Tarinee Rungjirajittranon, Weerapat Owattanapanich, Nattawut Leelakanok, Natthaporn Sasijareonrat, Bundarika Suwanawiboon, Yingyong Chinthammitr and Theera Ruchutrakool in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Abbreviations
Authors’ Contributions
T.R.1 and W.O. designed the study. T.R.1 and N.S. manually reviewed the potential articles, selected the included studies, and collected the data. T.R.1 and T.R.2 drafted the manuscript. W.O. and N.L. performed the statistical analyses. T.R.2, W.O., B.S., and Y.C. made critical revisions to the manuscript. T. R.1, T.R.2, and N.L. revised the final manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Trial Registration
CRD42021278161
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.