
Abstract
Background
Iliac vein compression syndrome (IVCS) diagnosis heavily relies on an imaging test. However, non-invasive and contrast-free imaging test for the diagnosis of IVCS remains a big challenge. To address this issue, this prospective study aimed to assess the image quality and diagnostic performance of a magnetic resonance imaging technique, black-blood venous imaging (BBVI), in detecting IVCS by comparing it with contrast-enhanced computed tomography venography (CTV) and using invasive digital subtraction angiography (DSA) as the reference.
Methods
We enrolled 105 patients, and all patients underwent BBVI, CTV, and DSA examinations. We compared the consistency of CTV and BBVI image quality and their consistency in diagnosing the rate of iliac vein stenosis in IVCS patients. Using the consensus DSA as a reference, the sensitivity, specificity, positive and negative predictive values, and accuracy of BBVI and CTV and their diagnostic agreement with DSA were calculated.
Results
BBVI demonstrated high sensitivity, specificity, and accuracy for the diagnosis of IVCS, without contrast agents. BBVI and CTV are quite in diagnosis IVCS. Quite SE (67.8% vs 68.3%), SP (94.8% vs 94.8%), PPV (98.0% vs 98.0%), NPV (46.2% vs 46.9%) and ACC (75.3% vs 75.7%) were obtained by BBVI in comparison with CTV.
Conclusion
BBVI has comparable diagnostic performance with CTV. It may be a viable alternative to CTV techniques in screening the IVCS without contrast agents and free of ionizing radiation.
Background
Iliac vein compression syndrome (IVCS) is also known as the May-Thurner syndrome or Cockett syndrome. 1 The right common iliac artery (RICA) mechanically compresses the left common iliac vein (LCIV) against the vertebral body and repetitively contacts it due to arterial pulsation. 2 Both the regular pulsations and chronic mechanical compression can result in endothelial damage in some individuals. Induction of elastin and collagen deposition and intimal fibrosis can cause intraluminal webs, channels, and spurs, resulting in a vascular gradient and slow flow distally. 3 Additionally, chronic venous stasis can lead to venous insufficiency, varicose veins, and pelvic congestion syndrome, even in the presence of the deep vein thrombosis (DVT). 4 The overall prevalence of symptomatic IVCS ranges from 18% to 49% among patients with left-sided lower extremity DVT.5,6
Several modalities have been used for the diagnosis of IVCS. Ultrasound with color Doppler and Doppler waveform imaging is typically the first-line technique in evaluating IVCS. 7 However, the evaluation is impossible in 20–50% of exams because the iliac veins are located deeply within the pelvis and overlying bowel gas, exacerbated by large body habitus and variation in sonographer expertise. 8 Computed Tomography Venography (CTV) is a fast and ubiquitous examination for diagnosing IVCS. 9 CTV can provide excellent detailed anatomy and images that can be interpreted easily. The main disadvantage of CTV is the high level of radiation which is around 5.2 mSv for the pelvis and 0.6 mSv for the lower limbs. 10 Moreover, contrast-induced nephropathy is another drawback of CTV. 11 As a gold standard for IVCS diagnosis, Digital Subtraction Angiography (DSA) is invasive and has more ionizing radiation than CTV 3 ; Intravascular Ultrasound (IVUS) is the current gold standard for the diagnosis of IVCS, but its invasiveness and high cost limits its clinical application. 7 Therefore, noninvasive and contrast-free imaging test for the diagnosis of IVCS remains a big challenge.
Magnetic resonance imaging (MRI) is an effective way of diagnosing iliac vein lesions. Several MRI techniques have been developed for analyzing IVCS in recent decades. These techniques include time-of-flight (TOF), bSSFP, and contrast-enhanced MR venography (CE-MRV). However, all these techniques are based on venography, making the venous lumen brighten on the acquired images. An obvious advantage of MRI is that there is no ionizing radiation in MRI examination compared to CTV. However, both CTV and MRV can see neither collagen deposition nor intimal fibrosis.
Recently, a three-dimensional (3D) T1-weighted black blood venous imaging (BBVI) technology has been developed to diagnose DVT without the use of contrast agents. 12 As the venous blood is suppressed, the thrombus can be directly visualized within the dark venous lumen.13,14 In addition, as the technique can realize 3D isotropic resolution imaging, we can freely reformat the acquired images from any plane. Thus, we hypothesized that the anatomical structure of the iliac vein and the lesion within the venous lumen could be well displayed by using BBVI for the diagnosis of IVCS.
This prospective study aimed to assess the image quality and diagnostic performance of BBVI in detecting IVCS by comparing it with CTV and using DSA as the reference standard.
Methods
Subjects
This study was approved by the local institutional review board, and written informed consent was obtained from all participants. A total of 109 patients were enrolled consecutively in a hospital from October 2019 to March 2021.
The inclusion criteria included:
Patients over 18 years old; The patients are suspected of MTS by anterograde lower extremity venography; The patients agree to sign an informed consent form to participate in the study; Patients who are participating in other clinical trials; Patients with acute deep vein thrombosis or post-thrombotic syndrome; Patients with iodine allergy; Women who are pregnant or breastfeeding; Patients with claustrophobia; Patients who do not agree to sign a written informed consent form.
The exclusion criteria included:
The symptoms of each patient, including the presence of edema, telangiectasia, reticular veins, varicose veins, hyperpigmentation, eczema, lipodermatosclerosis, and ulceration, were recorded according to the Clinical, Etiological, Anatomical, and Pathophysiological (CEAP) classification system for classifying venous disease severity.
15
Imaging Protocols
All patients with suspicious IVCS undergo CTV and BBVI. Specifically, we performed direct CTV, wherein a contrast agent is injected in the dorsal vein of both feet, with a tourniquet applied to the ankle to allow preferential contrast flow into the deep veins. We performed MR imaging on a 3.0 T scanner (Prisma, Siemens Healthineers, Erlangen, Germany) with two 18-channel abdominal phased array coils and a combined 32-channel spine coil. Scanning sequences include BBVI that uses a black-blood preparation combined with a T1-weighted 3D variable flip angle fast spin-echo. The scan parameters included: TR = 800 ms, TE = 11 ms, parallel acceleration factor = 4, turbo factor = 44, bandwidth = 1202 Hz/pixel, field of view = 380mm × 380mm, acquisition matrix = 320 × 320, isotropic spatial resolution = 1.2 mm × 1.2 mm × 1.2 mm which reconstructed to 0.6 mm × 0.6 mm × 0.6 mm.
Image Analysis
All CTV, BBVI, and DSA images were loaded onto a Syngo workstation for post-processing tasks such as multiplanar reconstruction (MPR), maximum intensity projection (MIP), and curved planar reformation (CPR).
Quantitative measurements of iliac vein compression were based on CTV and BBVI, respectively. The method proposed by Narayan et al was used for the measurement. 16 Specifically, the measurement is defined as the minor diameter of the left common iliac vein (LCIV) at the LCIV bifurcation or point of maximum compression divided by the minor diameter of the right common iliac vein (RCIV) before the RCIV bifurcation. If the patient was suspected of right side IVCS, the measurement is defined as the minor diameter of the RCIV at the RCIV bifurcation or point of maximum compression divided by the minor diameter of the LCIV before the LCIV bifurcation. The percentage of common iliac vein compression was also evaluated using the equation (1−the shortest diameter of the maximum compression point of the common iliac vein / the shortest diameter of the distal end of the contralateral common iliac vein) × 100%.
To analysis the image quality acquired by BBVI, a 4-level visual scoring method is adopted according to whether the image artifacts, image noises, and the boundaries of veins and blood vessels are apparent 12 : 4 -no obvious artifacts, no obvious noise, and very clear edges of veins; 3 - mild artifacts, mild noise, the edges of blood vessels are clear; 2 - more artifacts, more significant noise, and unclear edges; 1 - severe artifacts, obvious noise, and the edges of blood vessels are not visible.
Statistics
SPSS (v.22.0, SPSS Inc, Chicago, IL) was used for the statistical analysis. Normality test of measurement data adopts the skewness and kurtosis test. If the data obey normal distribution, the data is then expressed as
Results
A total of 109 patients were included. Two were swollen due to the lower limbs, which IVs could not be embedded, causing the CTV examination to fail. The BBVI examination was failed in another two patients because of the patients” dysphoria. Finally, we enrolled 105 patients. Example images of BBVI, CTV, and DSA were shown in Figure 1, respectively.

Representative images obtained by black blood venous imaging (A), computed tomography venography (B), and digital subtraction angiography (C) from a patient with IVCS.
Baseline Clinical Characteristics of Patients
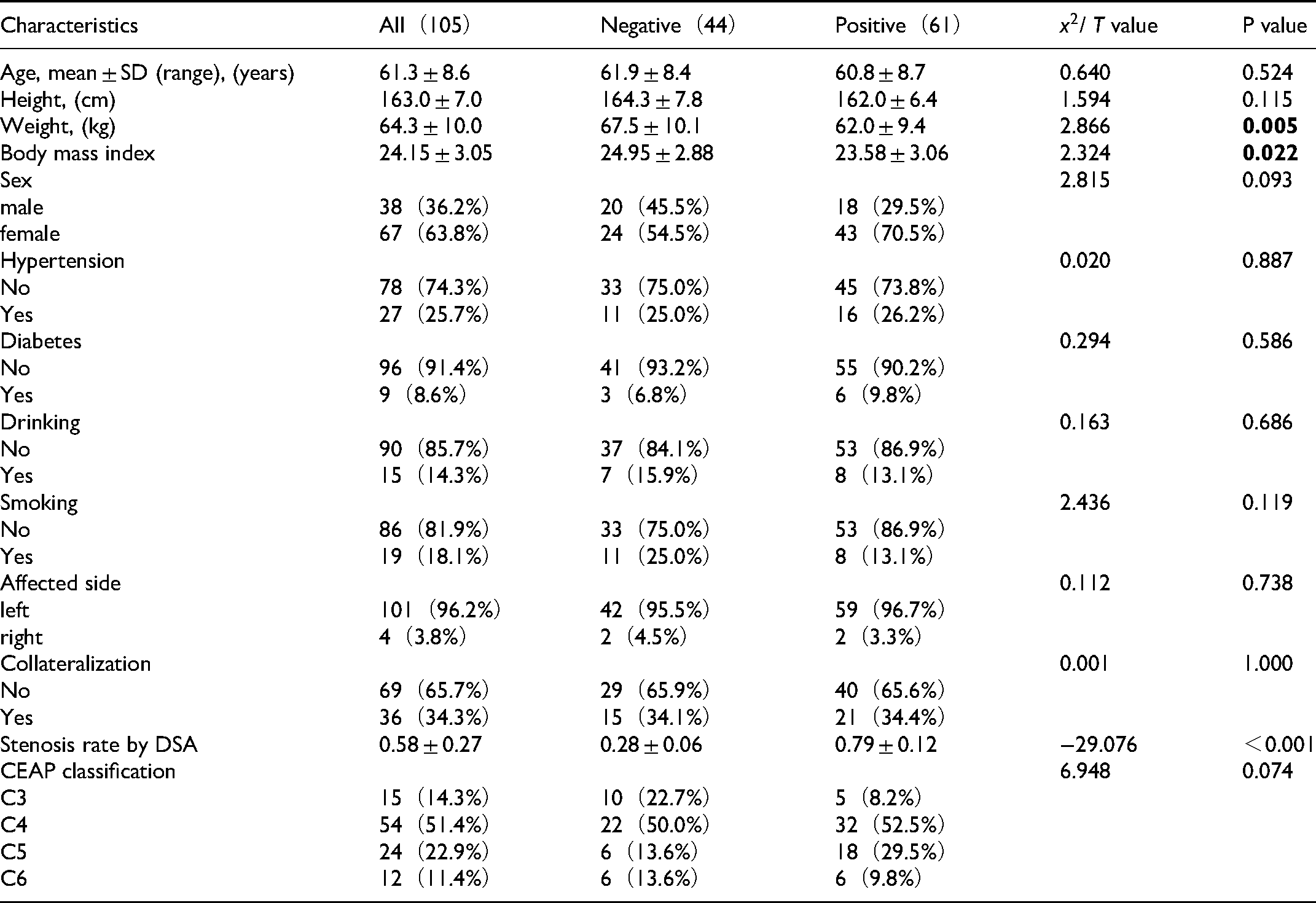
According to the stenosis rate measured by DSA, >50% was regarded as positive for IVCS diagnosis, and the data were divided into positive and negative IVCS groups. The primary data and compared results between the two groups are shown in Table 1. ① A total of 105 cases were collected in this study. Among them, women (63.8%) are more prominent than men (36.2%), with an average age of 61.3 ± 8.6 years, BMI of 24.15 ± 3.05; the highest proportion of chronic diseases is hypertension (25.7%), and the lowest diabetes (8.6%); the left side of the affected side is the central part (96.2%), and 34.3% of patients have collateral circulation; in terms of CEAP classification, C4 has the highest proportion (51.4%), and the lowest ratio is C6 (11.4%); ② All continuous variables conform to normal distribution; ③ The weight and BMI value of positive IVCS group are significantly lower than those of negative IVCS group (P < 0.05); The stenosis rate of positive IVCS group is significantly higher than that of negative IVCS group (P < 0.05); ④ There were no statistically significant differences in age, height, gender, hypertension, diabetes, drinking history, smoking history, affected limbs, collaterals, and CEAP grade distribution between the two groups (P > 0.05).
Patient's Characteristic.
The Consistency of the Judgments of the two Readers
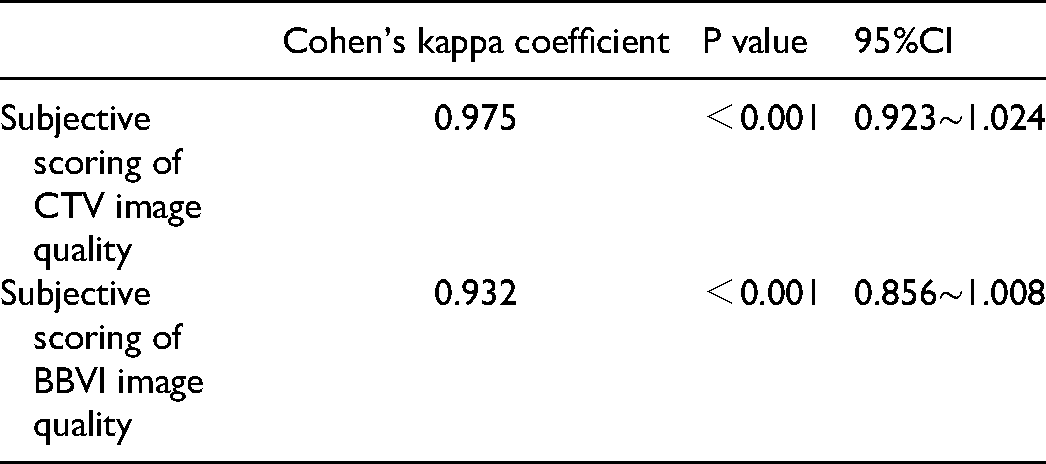
In this study, ①the Cohen's kappa coefficient was used to analyze the consistency of the judgments of the two readers on the subjective scoring of 105 subjects” BBVI and CTV image quality. The results showed that the Cohen's kappa coefficients of the two readers” judgments were 0.932 for BBVI image quality and 0.975 for CTV image quality separately, with excellent consistency; ② Using ICC coefficient to analyze the consistency of the interpretation of CTV and BBVI images of 105 subjects by two readers. It showed that the ICC coefficients were 0.778−0.938, which were all greater than the standard of 0.75, and the P values were all less than 0.05. It demonstrates that the two readers have a good understanding of both the CTV image and BBVI image. The shortest diameter of the most compressed part of the affected side common vein, the shortest diameter of the distal end of the contralateral common iliac vein, and the stenosis rate are consistent.
The consistency of the judgments of the two readers was shown in Tables 2 to 4.
The Consistency of the Image Quality of the Two Reade.

The Consistency of the Image Quality of the Two Reade.
The Consistency of the Judgments of the Two Reader.

Comparison of the Diagnostic Efficiency of the two Methods
Comparison of the diagnostic efficiency of BBVI and CTV was shown in Table 5. Using DSA as the reference, BBVI and CTV have comparable diagnostic performance in detecting IVCS interms of ROC area (average two readers: 0.813 vs 0.817), sensitivity (average two readers: 67.8% vs 68.3%), specificity (average two readers: 94.9% vs94.9%), positive predictive value (average two readers: 98.0% vs98.1%), negative predictive value (average two readers: 46.2% vs 46.9%), and accuracy (average two readers: 75.3% vs 75.7%).
The Qualitative and Statistical Analysis Results of BBVI and CTV for the Diagnosis of IVCS Using Consensus DSA as the Reference Standard.

Note: BBVI black-blood magnetic resonance venous imaging; CTV computed tomography venography.
Bland-Altman analysis results demonstrated that well agreements between CTV and BBVI were achieved for both two readers (Figure 2). Specifically, 3.81% (4/105) of Reader 1 points are outside the 95% LoA; Compared with the measured value of CTV and BBVI, within the consistency limit, the maximum absolute value of the difference is 0.25 (the uppermost point in the figure), and the average value of the difference is −0.01.
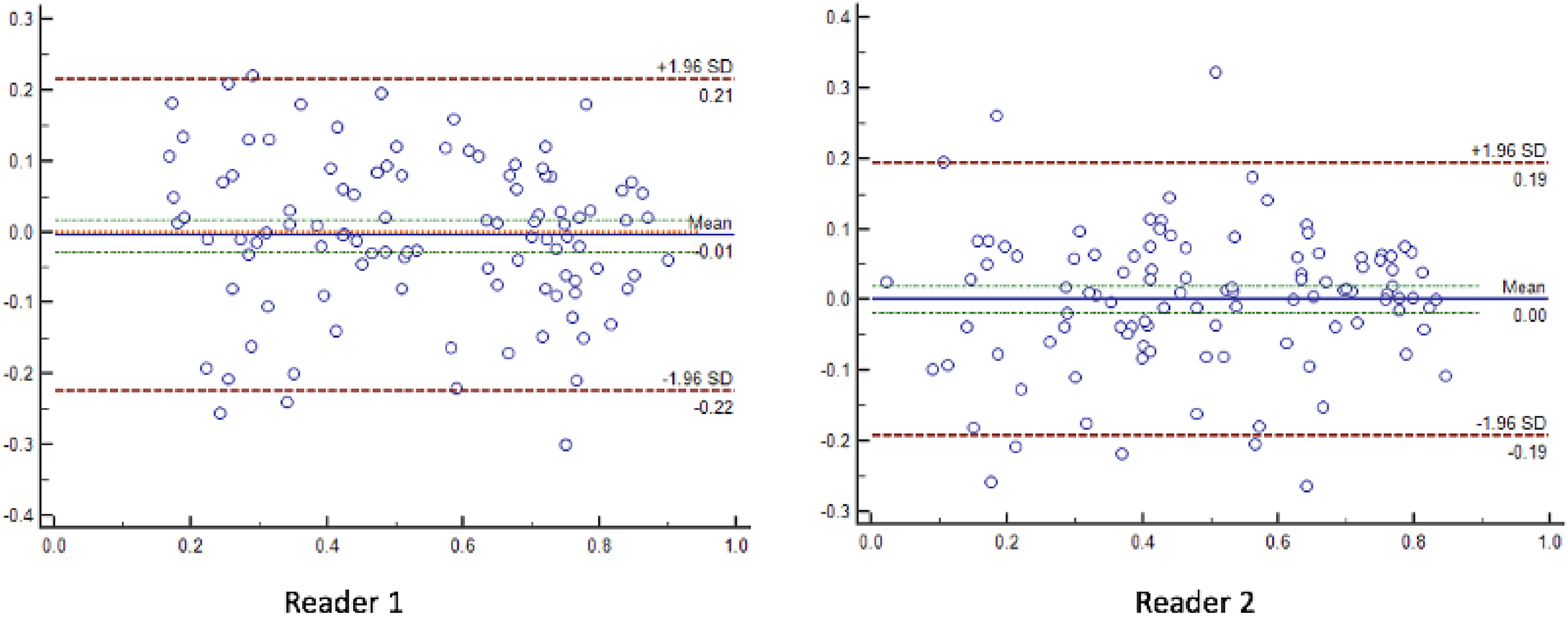
Well agreement between CTV and BBVI based on the bland-altman analysis.
Discussion
The results of our work suggest that BBVI demonstrated high sensitivity, specificity, and accuracy for the diagnosis of IVCS, without contrast agents.
BBVI has some significant technical advantages for the diagnosis of IVCS. 14 First, BBVI is based on SPACE readout which is a variant of a spin-echo sequence for 3D imaging with an intrinsically high SNR and rapid data acquisition, allowing for the BBVI scan within a reasonable scan duration (ie, less than 15 min for the entire lower limbs). Second, the venous and arterial blood flows can be well suppressed by BBVI. This allows observing the structures of the iliac veins, iliac arteries, as well as the relationship between the iliac veins and iliac arteries. As the anatomy of iliac veins and arteries is clearly observed on BBVI images, an accurate qualitative and quantitative analysis of the iliac vein compression becomes possible. Our experiment results demonstrated that the diagnostic confidence score of BBVI is comparable to that of CTV, and overall high sensitivity, specificity, negative/positive predictive value, and accuracy can be obtained by BBVI for the diagnosis of IVCS, using DSA as the standard reference.
Motion artifacts can be addressed well in the diagnosis of IVCS by using BBVI. As the iliac veins are located in the pelvic cavity, the undulation of the abdominal wall and the peristaltic of the intestine may result in motion artifacts 18,19; In order to reduce the respiratory motion artifacts, we used a respiratory bandage to reduce the breathing movement to reduce the respiratory motion artifacts. In addition, we also used a high receiving bandwidth to shorten the echo spacing. This can help to reduce the motion artifacts due to the peristaltic of the intestine. More importantly, the iliac veins and arteries are nearby the spine which is steel during MR scan. This makes the iliac veins and arteries can be displayed clearly on MR images. Our experiment results demonstrated that the iliac veins and arteries can be observed for qualitative and quantitative analysis, even though there are some motion artifacts on the BBVI images.
Compared to the bright-blood venography techniques, BBVI is a black-blood technique that not only displays the vascular cavity but also the vascular wall. 20 As the blood flows are suppressed by BBVI, there is no need to worry about the signal reduction caused by turbulence for the diagnosis of IVCS. 12 Previous studies have reported that contrast-free bright-blood venography, such as time of flight (TOF), has high sensitivity but low specificity.21,22 This is because accelerated blood flow or turbulence in the compression of the common iliac vein can cause MR signal voids, thereby exaggerating the compression of the iliac vein. 23 In contrast, BBVI suppresses the blood flows and displays the blood vessel wall instead of the vascular cavity. It thus can avoid the overestimation of the compression degree like TOF.
It can be considered that the two readers have the same understanding of CTV images and BBVI images. The shortest diameter of the most compressed part of the affected side common vein, the shortest diameter of the distal end of the contralateral common iliac vein, and the stenosis rate are consistent. From Table 4, we can see whether it is CT or MRI images when DSA images are used as the diagnostic gold standard, the two readers” specificity and positive predictive value are very high, but the sensitivity and accuracy are not very high. It can be seen from the ROC curve that the consistency of CT and MR images is very high in terms of sensitivity and specificity. This study aims not to replace the DSA diagnostic gold standard with MR examination, but the BBVI image can have a high consistency with the CT image. BBVI technology has no side effects of ionizing radiation and contrast agents. In clinical settings, it can reduce patient harm without reducing the consistency of diagnosis.
There were at least two limitations to this study. First, this was a prospective single-center study. However, as a proof-of-principle study, the purpose of this work is to prove the possibility of BBVI technology in the diagnosis of IVCS. Second, intravascular ultrasound (IVUS) is currently replacing DSA as the gold standard for IVCS diagnosis. 24 However, IVUS cannot be used routinely in many institutes, so we still use DSA as the gold standard for diagnosis.
Conclusion
BBVI has comparable diagnostic performance with CTV. It may be a viable alternative to CTV techniques in screening the IVCS without contrast agents and free of ionizing radiation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Fujian Province, (grant number 2021J01396).