
Abstract
Introduction
Predicting blood loss after cardiac surgery can allow clinicians to appropriately manage patients at high risk of mortality, because post-operative blood loss is related to the high risk mortality after cardiac surgery. 1 Re-operation due to defective hemostasis is another critical complication of cardiac surgery and is an independent risk factor for mortality. 2
Conventional coagulation parameters, including activated partial thromboplastin time (aPTT) and activated clotting time (ACT), are conventionally measured peri-operatively to assess the patients’ hemostatic status. Since rotational thromboelastometry (ROTEM) was introduced, its rapid assessment of clot formation made it a routine process to monitor coagulation parameters in operating rooms. However, the clinical utility of conventional coagulation tests such as aPTT and ACT as well as ROTEM for prediction of post-operative bleeding or re-operation after cardiac surgery is controversial.3–5
Thrombin generation assay (TGA) measures thrombin amount, which inversely correlates with bleeding tendency. TGA gives a global assessment of hemostasis of the hemostasis of the initial, amplification and propagation phases. Low thrombin generation more robustly reflects the hemorrhagic phenotype than conventional coagulation tests. 6 A few studies demonstrated significant TGA parameters for prediction of blood loss after cardiac surgery.7,8
Here we comprehensively investigated the hemostatic status of 65 patients who underwent cardiopulmonary bypass (CPB) at 4 different time points using TGA, ROTEM and conventional coagulation assays (aPTT and ACT) to identify useful parameters for identification of patients at high risk of post-operative bleeding and re-operation.
Methods
Patients
A total of 65 patients who underwent cardiac surgery with CPB were enrolled in this study. The median age of the patients was 65 years (interquartile range (IQR), 57–73) and the male-to-female ratio was 1.24. The median value of BMI was 21.8 kg/m2 (IQR, 18.9-23.4). Types of heart surgery were as follows: heart valve replacement only (n = 36), aorta replacement only (n = 6), coronary artery bypass graft surgery (CABG) only (n = 7), heart valve and aorta replacement (n = 7), heart valve replacement and CABG (n = 1), heart valve and aorta replacement with CABG (n = 2) and others (n = 6). This study complied with the Declaration of Helsinki and was approved by the Institutional Review Board of Seoul National University College of Medicine (IRB number 2112-001-1278).
The data on blood loss within 24 h after the surgery and on the patients who had a re-operation were retrieved from the chest tube output data in electronic medical records. Five patients underwent a re-exploration within 48 h after surgery. Among them, 4 patients received a re-operation due to bleeding (cardiac tamponade, n = 3; hematoma, n = 1) and one patient had a re-operation to remove a foreign body.
Anesthesia was induced using intravenous midazolam, sufentanil and vecuronium, and was maintained with continuous infusions of remifentanil and propofol. A non-pulsatile CPB technique was used with a membrane oxygenator and cardiotomy suction. Heparin was administered before CPB targeting ACT values of more than 500 s and was neutralized with protamine after discontinuing CPB.
Conventional coagulation assays (aPTT and ACT), ROTEM and TGA were performed at 4 time points: before skin incision (T1), after heparin injection (T2), after protamine reversal (T3) and before skin closure (T4).
Conventional Coagulation Assays
Peripheral whole blood was collected in 3.2% sodium citrate tubes (Becton Dickinson, San Jose, CA, USA). Plasma was separated by centrifugation at 1550 × g for 15 min within 1.5 h after blood sampling and was stored at − 80 °C. aPTT was measured on an ACL 3000 (Instrumentation Laboratory SpA, Milan, Italy) while ACT was measured using HemochronTM Signature Elite (Werfen, Barcelona, Spain).
ROTEM
ROTEM measurements were performed in operating rooms on a ROTEM Delta device (TEM International, Munich, Germany) using whole blood following the manufacturer's instructions. The following modes were used: coagulation induced by tissue factor (TF) (EXTEM), coagulation induced by phospholipid and ellagic acid (INTEM), inhibition of platelet function using cytochalasin D (FIBTEM) and heparin neutralization by heparinase (HEPTEM). The following ROTEM variables were measured: clotting time (CT, sec), maximum clot firmness (MCF, mm), clot formation time (CFT, sec) and alpha angle (°).
Thrombin Generation Assay
Thrombin generation assay was performed using a Thrombinoscope (Thrombinoscope BV, Maastricht, The Netherlands). TF with a final concentration of 5 pmol/L (PPP Reagent High, Thrombinoscope BV) or 1 pmol/L (PPP Reagent Low, Thrombinoscope BV) was used to stimulate thrombin generation. A total of 20 µL of reagent containing TF and phospholipid was mixed with 80 μL of platelet-poor plasma. Then, 20 µL of fluorogenic substrate in buffer containing Hepes and calcium chloride (FluCa-Kit, Thrombinoscope BV) was added to the mixture. The fluorescent signals were detected in a Fluoroskan Ascent fluorometer (Thermo Labsystems OY, Helsinki, Finland). Finally, thrombin generation curves were analyzed using Thrombinoscope software (Diagnostica Stago, Asnières-sur-Seine, France). The endogenous thrombin potential (ETP), peak thrombin, lag time and time to peak thrombin were measured.
Statistical Analyses
Data were compared between two groups using the Student t-test or Mann–Whitney U-test for continuous variables. For significantly different parameters between patients with ≥800 mL post-operative blood loss and those with < 800 mL blood loss, univariate linear regression analysis was performed to calculate the odds ratio and 95% confidence interval for the risk of high post-operative blood loss. Changes in coagulation parameters over 4 time points were visualized for comparison between patients who had a re-operation and those who did not, and two-way analysis of variance with a mixed-effect model was performed to compare the trends of data at 4 time points between the two groups. All statistical analyses were carried out using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). The level of significance was set at P < 0.05. For data visualization, GraphPad Prism 8.0.2 was used.
Results
Post-Operative Blood Loss
The median value of post-operative blood loss for 24 h after surgery was 803 (IQR, 560-1539) mL (Supplementary Figure S1). According to this median value, patients were divided into two groups: those with ≥ 800 mL (high) blood loss (n = 33) and those with < 800 mL (low) blood loss (n = 32).
Changes in Coagulation Parameters During CPB
Coagulation test results at the 4 time points during CPB are described in Table 1. The values of aPTT, ACT, CT-EXTEM, CT-INTEM, CT-FIBTEM, CT-HEPTEM, CFT-EXTEM, CFT-INTEM and CFT-HEPTEM at T2, T3 and T4 showed significant prolongation compared to T1. On the other hand, the values of MCF-EXTEM, MCF-INTEM, MCF-FIBTEM, MCF-HEPTEM, alpha angle-EXTEM, alpha angle-INTEM, alpha angle-FIBTEM and alpha angle-HEPTEM levels were significantly lower at T2, T3 and T4 than at T1. In TGA, ETP and peak thrombin levels (induced by both 5 and 1 pM TF) at T2, T3 and T4 were significantly lower than those at T1. The lag time and time to peak values (at both TF concentrations) were significantly lower at T2 (but not at T3 or T4) than at T1.
Coagulation Parameters Measured at 4 Different Time Points.

Data are expressed as median (interquartile range) for continuous variables. Four time points are as follows: T1, before skin incision; T2, after heparin injection; T3, after protamine reversal; T4, before skin closure. *Statistically significant (P < 0.05) compared to values measured at T1.
Abbreviations: aPTT, activated partial thromboplastin time; ACT, activated clotting time; CT, clotting time; CFT, clotting firmness time; ETP, endogenous thrombin potential; MCF, maximal clotting firmness; NA, not assessed; ROTEM, rotational thromboelastometry; TF, tissue factor; TGA, thrombin generation assay.
Coagulation Parameters for Prediction of High Post-Operative Blood Loss
APTT and ACT levels were not significantly different between high blood loss and low blood loss at all time points (Supplementary Table S1). However, ETP (at both 5 and 1 pM TF) and peak thrombin at 1 pM TF at T1 were significantly lower in the high blood loss group than in the low blood loss group (Figure 1). CT-INTEM at T3, CT-FIBTEM at T3, CFT-EXTEM at T2, T3 and T4, CFT-INTEM at T4 and CFT-HEPTEM at T2 were significantly higher in patients with high blood loss than in those with low blood loss. Conversely, patients with high blood loss showed significantly lower values of MCF-EXTEM at T2 and T4, MCF-INTEM at T4, MCF-FIBTEM at T3, MCF-HEPTEM at T2, alpha angle-EXTEM at T3 and T4 and alpha angle-INTEM at T4 than the low blood loss group (Figure 2).
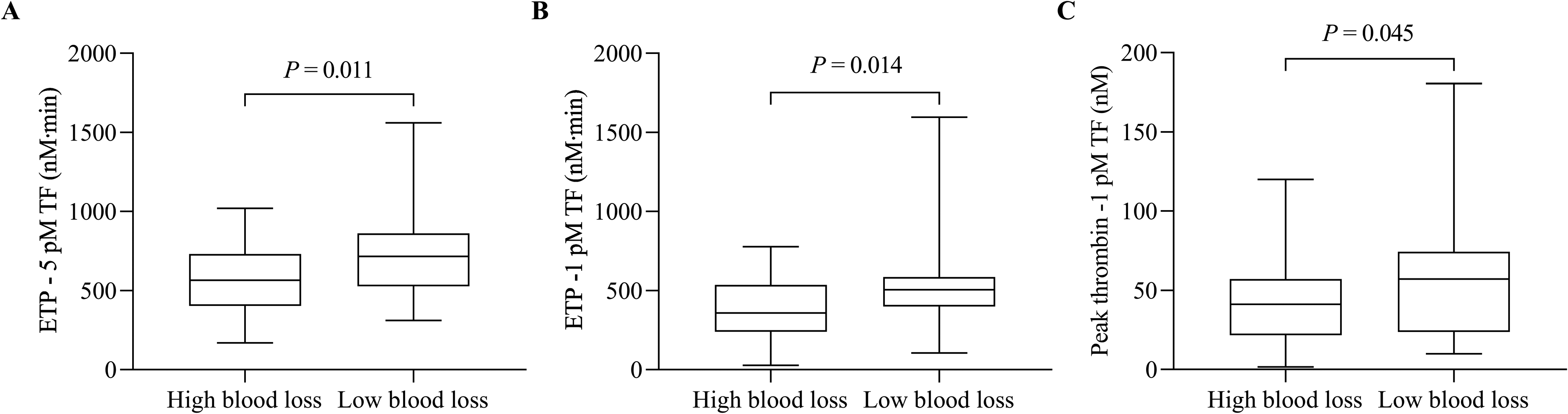
Thrombin generation assay parameters significantly different between patients with high blood loss (≥ 800 mL) and low blood loss (< 800 mL) within 24 h after cardiac surgery. (A) Endogenous thrombin potential (ETP) induced by 5 pM tissue factor (TF), (B) ETP induced by 1 pM TF, (C) Peak thrombin stimulated by 1 pM TF.

ROTEM parameters significantly different between patients with high blood loss (≥ 800 mL) and low blood loss (< 800 mL) within 24 h after cardiac surgery. (A-D) MCF-EXTEM, MCF-HEPTEM, CFT-HEPTEM and CFT-EXTEM measured at T2, (E-I) CT-INTEM, CT-FIBTEM, MCF-FIBTEM, CFT-EXTEM and alpha angle-EXTEM measured at T3, (J-O) MCF-EXTEM, MCF-INTEM, CFT-EXTEM, CFT-INTEM, alpha angle-EXTEM and alpha angle-INTEM. Abbreviations: CFT, clot formation time; CT, clotting time; MCF, maximum clot firmness; T1, before skin incision; T2, after heparin injection; T3, after protamine reversal; T4, before skin closure.
For the parameters showing significant differences between high and low blood loss, the cut-off values were determined as the values which yield best discrimination between high and low blood loss by using receiver operating characteristic analysis. At T1, patients with low ETP - 5 pM TF (≤ 486.0 nM·min) or low ETP - 1 pM TF (≤ 459.0 nM·min) showed significant odds ratios for prediction of high post-operative blood loss (Table 2). Patients with high peak thrombin - 1 pM TF (>54.04 nM) also showed a significant odds ratio. Significant odds ratios were detected at T2 for MCF and CFT of EXTEM and HEPTEM, at T3 for CT of INTEM and FIBTEM, MCF of FIBTEM, CFT of EXTEM and alpha angle of EXTEM and at T4 for MCF, CFT and alpha angle of EXTEM and INTEM.
Post-Operative Bleeding Risk of Coagulation Parameters.

Four time points are as follows: T1, before skin incision; T2, after heparin injection; T3, after protamine reversal; T4, before skin closure. Patients were categorized into two groups: high blood loss for those who had ≥ 800 mL post-operative blood loss within 24 h and low blood low for those who had < 800 mL blood loss. *The cutoff levels were determined as the values which can discriminate patients who had a blood loss of more than 800 mL and those with less than 800 mL post-operatively.
Abbreviations: aPTT, activated partial thromboplastin time; CFT, clotting firmness time; CI, confidence interval; ETP, endogenous thrombin potential; MCF, maximal clotting firmness; OR, odds ratio.
The T4/T1 or T1/T4 ratios were calculated for the above significant parameters, and the cut-off values of the ratios that showed best discrimination of post-operative blood loss were 0.8 for MCF-EXTEM and 0.4 for CFT-EXTEM (Figure 3). Patients with a T4/T1 ratio ≤ 0.8 for MCF-EXTEM showed significantly higher blood loss (median, 1280 mL; IQR, 735-1805) than those with a T4/T1 ratio > 0.8 (median, 697 mL; IQR, 508-895) (P = 0.034). Patients with a T1/T4 ratio ≤ 0.4 for CFT-EXTEM had significantly more post-operative bleeding (median, 1310 mL; IQR, 723-2377) than those with a T1/T4 ratio > 0.4 (median, 737 mL; IQR, 508-1300) (P = 0.030).

Difference in post-operative blood loss volume according to the ratios (T4/T1 or T1/T4) of MCF-EXTEM and CFT-EXTEM. (A) The T4/T1 ratio of MCF-EXTEM with a cutoff of 0.8, (B) The T1/T4 ratio of CFT-EXTEM with a cutoff of 0.4. Abbreviations: CFT, clot formation time; MCF, maximum clot firmness; T1, before skin incision; T4, before skin closure.
Temporal Changes of Coagulation Parameters Characteristic for re-Operation
Among 5 patients who underwent a re-operation, 4 patients who showed bleeding complication within 48 h after surgery were included in the re-operation group and 1 patient who did not show bleeding was excluded. The changes in coagulation parameters across 4 time points were compared between the re-operation group (n = 4) and no re-operation group (n = 60). CT-EXTEM gradually increased in patients who underwent a re-operation, but not in those without re-operation (P = 0.016), although CT-EXTEM values at each time point were not significantly different between the two groups (Figure 4). Among other parameters, there were no significant difference between the two groups.

Temporal changes in CT-EXTEM. CT-EXTEM showed an increase over 4 time points in patients who had a re-operation within 48 h due to bleeding (n = 4), which was significantly different by two-way analysis of variance with a mixed-effect model from CT-EXTEM in 60 patients who did not undergo re-operation (P = 0.016). Abbreviations: CT, clotting time; T1, before skin incision; T2, after heparin injection; T3, after protamine reversal; T4, before skin closure.
Discussion
We demonstrated that pre-operative ETP levels were significant predictors of high post-operative blood loss within 24 h after cardiac surgery. However, the results of conventional coagulation tests (aPTT and ACT) did not show any significant association with post-operative blood loss. These data indicate that routine testing by conventional coagulation assays is not useful and instead TGA should be recommended for prediction of post-operative blood loss. Since TGA can assess the whole coagulation process, reflecting in vivo coagulation status, whereas aPTT or ACT measure only the initiation stage of clotting, TGA is considered superior to aPTT or ACT in predicting post-operative bleeding. 6
In this study, we performed TGA at 4 time points, but only at the pre-operative time point ETP was revealed as a significant predictor of post-operative bleeding. This finding indicates that regardless of thrombin generation changes during operation, thrombin generation level measured pre-operatively can provide information about post-operative blood loss. Since the high level of heparin used during operation obscures the thrombin generation level, the intra-operative thrombin generation level may not represent the real in vivo coagulation status. Similar to our result, other reports also suggested that pre-operative thrombin generation is associated with post-operative bleeding.7,8
In TGA, we used 2 levels of TF. The usual level of TF level is 5 pM, while 1 pM TF is used to increase sensitivity to coagulation factors VIII, IX and XI. 9 In our results, ETP levels induced by both TF concentrations were significant predictors of post-operative bleeding, suggesting that not only factors VIII, IX and XI, but other coagulation factors also affected post-operative bleeding tendency.
We suggest that the low levels of ETP induced by both 5 pM and 1 pM TF predict a 4–5-fold higher bleeding risk. In the current situation, where the conventional coagulation tests (aPTT and ACT), which do not significantly predict post-operative bleeding, are used in CPB, TGA might help clinicians to manage patients after operation. However, TGA is not currently a point-of-care test and requires more time and a specialized machine to be performed. A development of a point-of-care test for TGA that can be performed near the patient is needed.
In our study, CT, MCF, CFT and alpha angle values of ROTEM measured at T2, T3 or T4 were significant parameters which can predict high blood loss, but at the baseline time point (T1) there was no significant ROTEM parameter. Studies that aimed to find out the ability of ROTEM to predict post-operative blood loss sometimes gave controversial results. Abnormal ROTEM thresholds of CT-EXTEM, CT-INTEM, MCF-EXTEM and MCF-FIBTEM after protamine injection have been reported to be associated with significant peri-operative blood loss in patients who undergo cardiac surgery. 5 In contrast, poor predictive utility for early bleeding after cardiac surgery has been suggested in other studies.3,10 Overall, baseline ROTEM levels seem not to be helpful for prediction of post-operative blood loss. Alternatively, some ROTEM values measured during and after cardiac surgery may imply significant blood loss.
A ratio of 0.2 of ETP measured at post-CPB versus pre-CPB has been shown to be significantly associated with chest drain output. 11 In our study, no significant relationship was found between the post-CPB/pre-CPB ETP ratio and post-operative blood loss. Instead, the T4/T1 ratio of MCF-EXTEM values and the T1/T4 ratio of CFT-EXTEM values differentiated patients with high and low blood loss.
Interestingly, there was a gradual increase in CT-EXTEM in patients who underwent a re-operation due to bleeding but not in those who did not undergo a re-operation. Risk factors for re-operation after cardiac surgery due to bleeding have been described and include low BMI, non-elective surgery, more than 5 grafts and old age at operation, all of which are clinical parameters. 12 Abnormal ROTEM values have been suggested as a significant risk factor for re-operation due to bleeding, although specific parameters have not been documented. 4 Our data suggest that an increase in CT-EXTEM during cardiac surgery may guide clinicians to manage patients who are susceptible to bleeding complication after surgery.
Our study has several limitations. First, we measured TGA in platelet-poor plasma of patients. The use of platelet-rich plasma for TGA would be helpful to reflect coagulation function, including platelet function, which is important for hemostasis. Second, there were only 4 patients who underwent a re-operation due to bleeding in our study. This small number might not be sufficient to reliably identify the risk factors for re-operation. Further study including adequate number of re-operation patients is needed. Nonetheless, this is, to the best of our knowledge, the first study that investigated conventional coagulation assays (aPTT and ACT), ROTEM and TGA at the same time in CPB patients at 4 different time points.
In summary, pre-operative ETP levels can detect patients who are likely to have blood loss of more than 800 mL within 24 h after cardiac surgery. CT, MCF, CFT and alpha angle values measured at T2, T3 or T4 are significant ROTEM parameters that can predict high post-operative blood loss. An increase in CT-EXTEM suggests high risk of re-operation within 48 h due to bleeding. We expect pre-operative ETP measurements to help clinicians to predict the high risk of post-operative blood loss. The ROTEM parameters measured during surgery may also help to predict post-operative blood loss and re-operation risk.
Supplemental Material
sj-docx-1-cat-10.1177_10760296221123310 - Supplemental material for Assessment of Rotational Thromboelastometry and Thrombin Generation Assay to Identify Risk of High Blood Loss and Re-Operation After Cardiac Surgery
Supplemental material, sj-docx-1-cat-10.1177_10760296221123310 for Assessment of Rotational Thromboelastometry and Thrombin Generation Assay to Identify Risk of High Blood Loss and Re-Operation After Cardiac Surgery by Dajeong Jeong, Seon Young Kim and Ja-Yoon Gu, Hyun Kyung Kim in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgements
The authors gratefully acknowledge Prof. Yunseok Jeon for assistance with specimen collection for this study.
Author Contributions
DJ performed the research, analyzed data and wrote the paper; SYK performed the research and analyzed data; J-YG performed the research; HKK designed the research, analyzed data and wrote the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant (2021R1A2C1006302) funded by the Korea Government (MSIT).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.