
Abstract
Background
The Prognostic Nutritional Index (PNI) has been reported to be correlated with long-term outcomes after gastrointestinal tumor surgery. However, to our knowledge, only a few studies have shown that the PNI is related to cardiovascular diseases. Therefore, we aimed to assess the association between the PNI and long-term outcomes in patients with coronary artery disease (CAD) undergoing percutaneous coronary intervention (PCI).
Methods
This was retrospective observational study. A total of 3561 patients with CAD after PCI were retrospectively enrolled in the CORFCHD-ZZ study from January 2013 to December 2017. The patients (3519) were divided into three groups according to PNI tertiles: the first tertile (PNI < 47.12, n = 1173), the second tertile (47.12 ≤ PNI < 51.50, n = 1185), and the third tertile (PNI ≥ 51.50, n = 1161). The mean follow-up time was 37.59 ± 22.24 months. The primary endpoint long-term mortality, including all-cause mortality (ACM) and cardiac mortality (CM).Secondary endpoints were major adverse cardiovascular events (MACEs) and major adverse cardiovascular and cerebrovascular events (MACCEs).
Result
In our study, the incidences of ACM in the first, second, and third tertiles were 3.8%, 1.8% and 1.4%, respectively (P < 0.001). The incidences of CM occurring in the first, second, and third tertiles were 1.7%, 3.1% and 2.1%, respectively (P < 0.001).There was statistically significant different in primary endpoints incidence. MACEs occurred in 139 patients (11.8%) in the first tertile, 121 patients(11.1%) in the second tertile and 123 patients(10.8%) in the third tertile(P = 0.691). MACCEs occurred in 183 patients (15.6%) in the first tertile, 174 patients(14.7%) in the second tertile and 160 patients(13.85%) in the third tertile(P = 0.463).There was no statistically significant different in secondary endpoints incidence. Kaplan–Meier analyses showed that elevated PNI was significantly related to long-term CM (log rank, P < 0.001) and long-term ACM (log-rank, P < 0.001). Cox regression analyses suggested that compared with the patients in the first tertile, the risk of ACM was decreased to 60.9% (HR = 0.609, 95% CI: 0.398–0.932, P = 0.029) in the second tertile and 40.3%(HR = 0.403, 95% CI: 0.279–0.766, P = 0.003) in the third tertile, while the risk of CM was decreased to 58.8%(HR = 0.588, 95% CI: 0.321–0.969, P = 0.038) in the second tertile and 46.6%(HR = 0.466, 95% CI: 0.250–0.870, P = 0.017) in the third tertile. Multivariate Cox regression analyses showed that the PNI was an independent predictor of long-term ACM and CM.
Conclusion
Our finding shown that PNI is an independent predictor in CAD patients after PCI,the higher the PNI, the less occurring adverse event. Therefore,PNI may be an new biomarker to predict long-term outcome of CAD patients after PCI.
Keywords
Background
Coronary artery disease (CAD) is a heart disease affecting millions of individuals worldwide, which is one of the leading cause of death in chronic diseases throughout the world.It has been the leading cause of death from chronic diseases worldwide. 1 CAD is a disease with multiple mechanisms.These mechanisms are oxidative stress, 2 thrombosis, 3 estrogen deficiency 4 and lipid metabolism 5 which have been well recognized in the past. In addition, increasing evidence has recently suggested that inflammation plays an important role in the progression of coronary disease.6, 7
Percutaneous coronary intervention (PCI) is a treatment method that improves myocardial perfusion by unblocking the lumen of narrowed or even occluded coronary arteries. Cardiac catheterization technique is an effective treatment for CAD.8, 9 However, cardiovascular adverse events can still occur in some patients undergoing PCI. Therefore, it is particularly important to analyze the prediction of long-term adverse outcomes in patients with CAD after PCI.
The prognostic nutritional index (PNI) is calculated by the serum albumin concentration and total lymphocyte count in peripheral blood. This indicator quantifies nutritional and immunological status. 10 It was initially designed to evaluate the long-term outcomes and prognoses in patients with gastrointestinal cancers. 11 Since then, the significance of the PNI as a prognostic predictor has been revealed in various types of human cancers.12–14
However, only a few studies have shown that the PNI is associated with cardiovascular disease. Therefore, we conducted a study with a larger sample size and aimed to investigate the correlation between PNI and clinical outcomes in patients with CAD who underwent PCI.
Methods
Study Design and Population
This is a large, single-center, retrospective cohort study. From 2013 to 2017, 3561 CAD patients hospitalized at the First Affiliated Hospital of Zhengzhou University were initially enrolled in the Clinical Outcomes and Risk Factors of Patients with Coronary Heart Disease after PCI (CORFCHD-ZZ, identifier: ChiCTR1800019699) study; 42 patients were subsequently eliminated due to unavailable baseline Alb or TLC data. Finally, there were 3519 patients who were enrolled in the present study. All of the aforementioned results are shown in Figure 1.
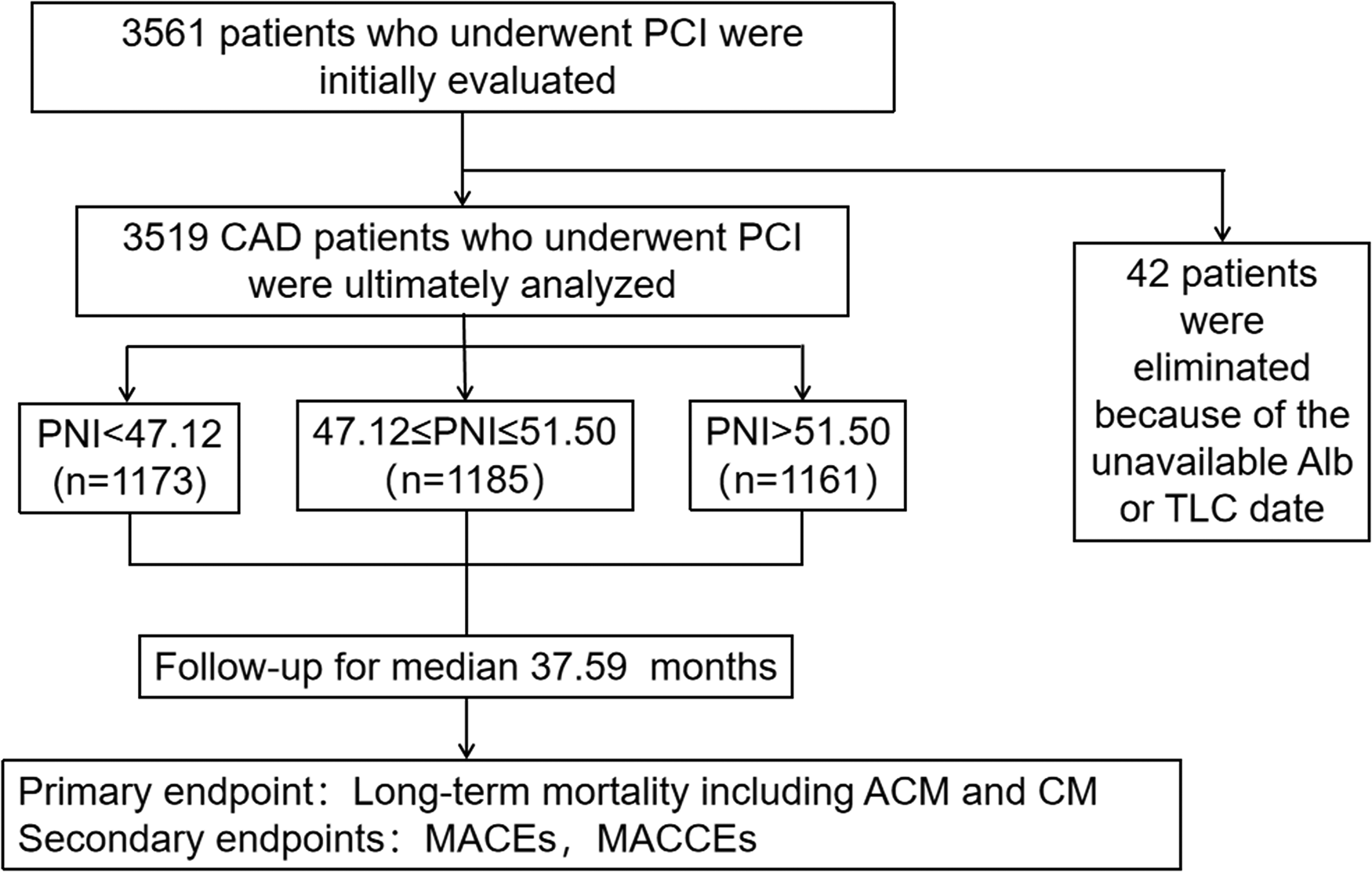
The flowchart of patient’s enrollment.
The inclusion criteria for the study population were as follows: (1) patients older than 18 years old and younger than 80 years old; (2) at least one coronary artery with ≥50% stenosis confirmed by coronary angiography; (3) at least one clinical phenotype of CAD -- stable angina or acute coronary syndrome; (4) an objective test with evidence of myocardial ischemia -- positive plate test, FFR <0.8, OCT or IVUS suggestive of unstable plaque; and (5) treatment with percutaneous coronary intervention (PCI) in our hospital.
The exclusion criteria for the study population were as follows: (1) younger than 18 years of age or older than 80 years of age; (2) combined with severe valvular heart disease; (3) combined with severe congenital heart disease; (4) combined with hyperthyroidism, anemia or hyperdynamic heart disease; (5) combined with pulmonary heart disease; (6) combined with hypertrophic obstructive cardiomyopathy; (7) combined with hepatic insufficiency (defined as alanine aminotransferase or total bilirubin more than 3 times the upper limit of normal); (8) combined with renal insufficiency (defined as serum creatinine exceeding 1.5 times the upper limit of normal); (9) not infected 2 weeks prior to onset; and (10) combined hematologic disorders, such as various types of anemia, leukemia, lymphoma and other diseases.
Definitions
Hypertension was defined as a previous definitive diagnosis that referred to systolic blood pressure (SBP) of ≥140 mm Hg and/or a diastolic blood pressure (DBP) of ≥90 mm Hg on at least three resting measurements at no fewer than two separate health care visits according to the American Heart Association (AHA) recommendations. 15 Diabetes was defined as a previous definitive diagnosis that referred to fasting plasma glucose (FPG) ≥ 7.0 mmol/L or two-hour postprandial glucose (2-h PG) ≥ 11.1 mmol/L during an oral glucose tolerance test (OGTT) according to the American Diabetes Association (ADA) recommendations. 16 MACEs were defined as cardiac death, heart failure, bleeding events and readmission. MACCEs were defined as MACEs combined with stroke.
Clinical and Demographic Characteristics Collection
Data on clinical and demographic characteristics, including age, sex, history of hypertension and diabetes, family history of CAD, and smoking and drinking status, were collected from the medical records of inpatients at the First Affiliated Hospital of Zhengzhou University.
The laboratory data included plasma and biochemical parameters, such as the levels of serum albumin (Alb), total lymphocyte count (TLC), absolute neutrophil count (ANC), platelet count (PLT), red blood count (RBC), globulin (Glb), triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), blood urea nitrogen (BUN), creatinine (Cr), uric acid (UA), glomerular filtration rate (GFR), glucose (GLU), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transferase (GGT).
Patients were advised to fast for at least 12 h before blood samples were collected.
Measurement of blood parameters was performed using a standard method in accordance with the central laboratory standard of the First Affiliated Hospital of Zhengzhou University.
We also noted the angiographic results of the patients, including lesion extent, lesion location, lesion stenosis, stent implantation site and number, preoperative TIMI grading, etc, which were obtained in the cardiac catheterization operating rooms in the First Affiliated Hospital of Zhengzhou University.
Endpoints and Follow-up
The primary endpoint was long-term mortality, including all-cause mortality (ACM) and cardiac mortality (CM). The secondary endpoints were major adverse cardiovascular events (MACEs) and the composite of major adverse cardiovascular and cerebrovascular events (MACCEs). The follow-up time ranged from 15 to 50 months, and the mean value was 37.59 ± 22.24 months. During the follow-up, compliance with drugs and adverse events were carefully assessed by well-trained clinical physicians.
Statistical Analysis
All data were analyzed using SPSS software, version 22.0. We divided the PNI into three groups according to derived PNI tertiles: the first tertile (PNI < 47.12, n = 1173), the second tertile (47.12 ≤ PNI < 51.50, n = 1185) and the third tertile (PNI ≥ 51.50, n = 1161). This classification indicates the nutritional status of the population: the first tertile (PNI1) represents the population of patients who are malnourished, the second tertile (PNI2) represents the population of patients who are nutritionally eligible, and the third tertile (PNI3) represents the population of patients who are well nourished. Continuous variables are expressed as the mean ± standard deviation (normally distributed) and the median and interquartile range (not normally distributed). They were compared using ANOVA. Categorical variables are expressed as frequencies and percentages. They were compared using the chi-square test. The Kaplan-Meier method and the log-rank test were used to estimate the cumulative incidence of long-term adverse outcomes. A multivariate Cox proportional risk regression model was used to assess the independent predictive value of the PNI for long-term adverse outcomes. A P value <0.05 indicated that the data differences were statistically significant.
Results
Baseline Characteristics
In our study, the critical values of the baseline PNI were 47.12 and 51.50 according to the basic status of the population. A total of 3519 patients with CAD after PCI were divided into three groups according to the derived PNI tertile: the first tertile (PNI < 47.12, n = 1173), the second tertile (47.12 ≤ PNI < 51.50, n = 1185) and the third tertile (PNI ≥ 51.50, n = 1161). As shown in Table 1, we found that there were significant differences in several variables among the three groups, such as age, Cr, UA, TC, TG, HDL-C and LDL-C (all P < 0.05). However, the following variables were not significantly different among the three groups: sex, hypertension, diabetes, HR, smoking and drinking (all P ≥ 0.05).
Baseline Characteristics of Patients.

Data presented as mean ± SD, median and interquartile range or n (%).
Abbreviation: PNI Prognostic nutritional index, HR Heart rate, BUN Blood urea nitrogen, Cr Creatinine, UA Uric acid, TG Triglyceride, TC Total cholesterol, HDL-C High-density lipoprotein cholesterol, LDL-C Low-density lipoprotein cholesterol.
Note: The boldfaced P-Values are statistically different.
Outcomes
As shown in Table 2, for the primary end point, the incidences of ACM (3.8% vs 1.8% vs 1.4%, P < 0.001) and CM (5.9% vs 3.1% vs 2.1%, P < 0.001) were significantly different among the three groups, but for the secondary end points, we found that there were no significant differences among the three groups in the incidence of MACEs (11.8% vs 11.1% vs 10.8%, P = 0.691) and MACCEs (15.6% vs 14.7% vs 13.85%, P = 0.463).
Outcomes Comparison Between Groups.

Abbreviation: ACM All-cause mortality, CM Cardiac mortality, MACEs Major adverse cardiovascular events, MACCEs Major adverse cardiovascular and cerebrovascular events.
Note: The boldfaced P-Values are statistically different.
Furthermore, as shown in Table 3, Figure 2 and Figure 3, the Kaplan-Meier analyses showed that an elevated PNI was significantly related to long-term ACM (log-rank, P < 0.001) and CM (log-rank, P < 0.001).

Cumulative Kaplan–Meier estimates of the time to the first adjudicated occurrence of ACM. The X axis represents the follow-up time, and the Y axis represents the cumulative incidence of ACM. The yellow line indicates the first tertile (PNI1),the green line indicates the second tertile (PNI2) and the blue line indicates the third tertile (PNI3).

Cumulative Kaplan–Meier estimates of the time to the first adjudicated occurrence of CM. The X axis represents the follow-up time, and the Y axis represents the cumulative incidence of CM. The yellow line indicates the first tertile (PNI1),the green line indicates the second tertile (PNI2) and the blue line indicates the third tertile (PNI3).
Incidence of Outcomes on Multivariate Cox Proportional Hazards Regression Models and log-Rank Test.

Abbreviation: ACM All-cause mortality, CM Cardiac mortality, MACEs Major adverse cardiovascular events, MACCEs Major adverse cardiovascular and cerebrovascular events.
Note: The boldfaced P-Values are statistically different.
Adjusted for age, creatinine, uric acid, triglyceride, total cholesterol, high-density lipoprotein cholesterol and low-density lipoprotein cholesterol.
Multivariate Cox regression analyses showed that the PNI was an independent predictor of long-term ACM and CM.
Multivariate Cox proportional hazards regression models were conducted to evaluate the correlation between the PNI and outcomes; the models were adjusted for confounding factors, including age, sex, hypertension, diabetes, smoking, drinking, Cr, UA, TG, TC, HDL-C and LDL-C. The results suggested that, compared with the patients in the first tertile, the risk of ACM was decreased to 60.9% (HR = 0.609, 95% CI: 0.398–0.932, P = 0.029) in the second tertile and 40.3% (HR = 0.403, 95% CI: 0.279–0.766, P = 0.003) in the third tertile, while the risk of CM was decreased to 58.8% (HR = 0.588, 95% CI: 0.321–0.969, P = 0.038) in the second tertile and 46.6% (HR = 0.466, 95% CI: 0.250–0.870, P = 0.017) in the third tertile. Therefore, an increased PNI was an independent predictor of long-term ACM and CM. In addition, confounding variables of long-term ACM and CM are shown in Table 4 and Table 5.
Cox Regression Analysis Results for Long-Term ACM.

Abbreviation: ACM All-cause mortality, Cr Creatinine, UA Uric acid, TC Total cholesterol, TG Triglyceride, HDL-C High-density lipoprotein cholesterol, LDL-C Low-density lipoprotein cholesterol, PNI Prognostic nutritional index.
Note: The boldfaced P-Values are statistically different.
Cox Regression Analysis Results for Long-Term CM.

Abbreviation: CM Cardiac mortality, Cr Creatinine, UA Uric acid, TC Total cholesterol, TG Triglyceride, HDL-C High-density lipoprotein cholesterol, LDL-C Low-density lipoprotein cholesterol, PNI Prognostic nutritional index.
Note: The boldfaced P-Values are statistically different.
Discussion
In our study, we found that the PNI was independently associated with the prognosis of CAD patients who underwent PCI and found that a lower prognostic nutritional index (PNI1) was independently associated with adverse outcomes. Besides, there were differences in age, Cr, UA, TG, TC, HDL-C and LDL-C among the three groups of patients. Patients with younger age had a higher nutritional index and a good prognosis. HDL-C is a protective factor for patients with CAD, we found that patients in the higher PNI group had higher HDL-C. But the patients in the higher PNI group had higher TG,TC and LDL-C, these may indicated why PNI was not significant associated with secondary endpoints.
The most representative of these researchers is Wada H, who found that the PNI had a significant relationship with long-term outcomes in patients with stable CAD in a Japanese population. 17 Nevertheless, compared to our study, the analysis method for determining the PNI cutoff value was different, and their study had a smaller sample size. Furthermore, our research is the first study to investigate the relationship between the PNI and outcomes in CAD patients after PCI in China, the nation with the largest population worldwide.
Several mechanistic pathways could connect the PNI to adverse prognosis in patients with CAD after PCI. Below are explanations for the association between the PNI and patients from the mechanistic point of view.
First, previous studies have suggested that the PNI can reflect systemic inflammation and nutritional status to accurately predict cancer patient prognosis.18, 19 Furthermore, Alparslan Kurtul et al(2021) recently found that the PNI also reflected the immunonutritional-inflammatory status in cardiovascular diseases. 20 Therefore, we strongly believe that adverse cardiovascular events are associated with a reduction in the PNI through the inflammatory response. Moreover, relevant research has stated that serum albumin is a negative acute phase reactant. It has also been reported that a decrease in serum albumin synthesis associated with inflammation is followed by an increase in catabolism.21, 22 While serum albumin levels are reduced, proinflammatory cytokines (eg, TNF-α, NF-kB, etc) are activated, thereby promoting the development, formation, and rupture of atherosclerotic lesions in coronary arteries. 23 Therefore, decreased serum albumin levels are considered a risk factor for CAD. Last but not least, an increasing number of studies have shown that a decrease in blood lymphocyte count is strongly correlated with the development of premature CAD. 24 The redistribution of T cells from the circulation to lymphoid tissue could exacerbate lymphocyte growth; it might induce compensatory proliferation of antigen-experienced T cells, which could increase the risk of cardiovascular disease. 25 Therefore, a low lymphocyte count is considered a risk factor for coronary heart disease. In summary, there is much evidence that decreased serum albumin levels and low lymphocyte counts are both risk factors that contribute to the development of coronary atherosclerosis. Based on the PNI being made up of Alb and TLC, we hold the view that the PNI is related to inflammation and immunity.
The significance of our study was that we provide strong support that the inflammatory response plays an important role in the development of CAD. At the same time, we also provide a simple and easy monitoring indicator for patients after PCI to estimate the probability of adverse prognostic outcomes. However, there were also some limitations to our research, which are as follows. First, we only collected the baseline data of Alb and TLC; the influence of dynamic changes in the PNI on mortality was unclear. In addition, our study had a single-center, retrospective cohort design; therefore, a multi-center cohort design is needed in the future. Finally, the follow-up data collection was incomplete in this study, which could have caused selection bias. Therefore, the findings in our study must be further demonstrated in different populations.
Conclusion
In conclusion, we found in the present study that the PNI is a simple, reliable, inexpensive, effective and independent predictor of adverse outcomes in patients with CAD after PCI. However, we require more prospective trials to further demonstrate the prognostic value of the PNI in CAD patients.
Footnotes
Acknowledgements
The authors are grateful to the Department of Cardiology at the First Affiliated Hospital of Zhengzhou University for their help and expertise in conducting this study.
Authors' Contributions
(I) Conception and design: TDL and YYZ; (II) Administrative support: JYZ; (III) Provision of study materials or patients: All authors; (IV) Collection and assembly of data: TDL,XYD, JCZ, QQG,MDC, FHS, ZYL, KW, LF, XTY, YB, ZLZ and RJZ; (V) Data analysis and interpretation: TDL and YYZ; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Data Availability Statement
The data will not be shared, because the identified participant information is included in the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Natural Science Foundation of Henan Province (grant number 212300410072), National Natural Science Foundation of China (grant number 82000238), 2019 Henan Province Medical Science and Technology Research Plan (grant number LHGJ20190119), and CORFCHD-ZZ (grant number ChiCTR1800019699).
Ethics Statement
This study protocol was approved by the ethics committee of the First Affiliated Hospital of Zhengzhou University, and was in line with the Declaration of Helsinki. Due to the retrospective design of the study, the need to obtain informed consent from eligible patients was waived by the ethics committee. The authors were accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Consent for Publication
Written informed consent for publication was obtained from each author, and there are no other persons who satisfy the criteria for authorship but are not listed.