
Abstract
We examined whether resting levels and exercise-induced changes during exercise ECG stress test (EST) of cardiac Troponin T (cTnT), NT-proBNP and prothrombotic markers were affected by revascularization in patients with coronary artery disease (CAD).
EST1 was performed before coronary angiography and revascularization, and patients (n = 20) with confirmed CAD, performed another EST (EST2) 9 weeks later. Blood samples were drawn at rest and within five min after termination of ESTs.
cTnT and NT-proBNP increased during exercise at both ESTs (p < 0.001, all). Resting cTnT levels at EST2 versus EST1 were significantly higher (p = 0.02) whereas NT-proBNP did not differ. At both visits, increased D-dimer (p = 0.008 and <0.001), pro-thrombin fragment 1 + 2 (p = 0.009 and 0.001) and tissue factor pathway inhibitor (TFPI) (p < 0.001 and 0.001) during exercise were demonstrated. Resting levels of endogenous thrombin potential (ETP) and TFPI were reduced at EST2 versus EST1 (p < 0.01).
Revascularization did not affect exercise-induced release of cardiac and prothrombotic biomarkers and did not reduce resting levels of cTnT or NT-proBNP, suggesting revascularization per se not to prevent secretion of biomarkers. The lower resting levels of ETP and TFPI after revascularization may however, be indicative of reduced thrombin generation and endothelial activation.
Clinicaltrials.gov, CADENCE, NCT01495091 https://clinicaltrials.gov/ct2/show/NCT01495091?term = 01495091&draw = 2&rank = 1.
Keywords
Introduction
The main underlying mechanism of coronary artery disease (CAD) is atherosclerosis, and may manifest different clinical conditions, from chronic CAD with chest pain to acute coronary syndrome (ACS) or an acute myocardial infarction (AMI). The latter often occurs by plaque rupture, initiated by endothelial dysfunction and injury, and activation of the haemostatic system with thrombus formation and potential coronary vessel occlusion. 1 The haemostatic activation is thus more prominent in the acute phase. 2
High-sensitive cardiac troponin T (cTnT) measures are used for the clinical diagnosis of ACS. In patients with chest pain and known stable CAD, hs-cTnT has been shown to be of prognostic importance,3-5 and studies have also reported troponin levels to be increased in patients with stable CAD compared to those without.6,7 Another potential biomarker of CAD is the well known N-terminal pro B-type natriuretic peptide (NT-proBNP), 8 and in patients with stable CAD NT-pro-BNP is known to have prognostic value.9-11
The main contributors to plaque rupture are still not known. It is however, well recognized that strenuous physical exercise may provoke symptoms of angina pectoris or an ACS. Exercise-induced release of cardiac biomarkers like troponins and NT-proBNP in healthy individuals has been reported,12,13 indicating cardiomyocyte activation and potential myocardial injury during exercise. Also, a transient increase of prothrombotic biomarkers have been shown during exercise in subjects with and without CAD, especially those being physically inactive.14-16
We have previously shown levels of cTnT, 17 troponin I (TnI), 18 NT-proBNP 19 as well as in haemostatic biomarkers 20 to increase during strenuous physical exercise in patients with symptoms of chronic CAD. We also observed that the changes during exercise did not differ between patients with or without CAD verified by angiography. However, resting levels were higher in CAD patients before they were revascularized compared to those without CAD. 20
In the present investigation we aimed to explore whether revascularization of patients with verified CAD would influence resting levels and exercise-induced changes in cTnT, NT-proBNP and the thrombotic markers prothrombin fragment (F) 1 + 2, D-dimer, tissue factor pathway inhibitor (TFPI) and endogenous thrombin potential (ETP). We hypothesized that resting and exercise-induced levels of the biomarkers would be reduced after revascularization.
Material and Methods
Study Population
This is a sub-study of the CADENCE-study in which patients presenting with symptoms of CAD and referred for an exercise stress test (EST) followed by coronary angiography were included at the Department of Cardiology, Oslo University Hospital Ullevaal, Oslo, Norway . The main study protocol has previously been described in details. 17 Of the 111 patients with confirmed CAD, 20 patients were randomly invited to a follow-up EST. A thorough physical examination including blood pressure, weight and waist circumference was performed prior to the EST at both occasions. The Regional Ethics Committee in South Eastern Health Region in Norway approved the protocol, and the study was conducted in accordance with the Declaration of Helsinki. All participants gave written informed consent. The study is registered at clinicaltrials.gov, NCT01495091.
Methods
Both in the main CADENCE study and in the present substudy a resting 12-lead electrocardiogram (ECG) and a maximal exercise ECG stress test (EST1 and EST2) were performed using an electrical bicycle ergometer and monitored by a computerized ECG. The initial workload was 30 watts (W) for women and 50 W for men, with a gradual increase of 10 W per min with participants maintaining a pedaling rate of about 65 rpm. Every third min patients were monitored by Borg scale, 21 and blood pressure was measured every third min of the test. Patients were exercised to exhaustion if no clinical signs of ischemia developed. A positive test was defined as having horizontal or down-sloping ST-segment > 1.0 mm (0.1 mV) at 60 millisec after the J point and/or chest pain or discomfort.
All patients in the CADENCE study underwent coronary angiography, independent of the EST1 result, performed by the standard Seldinger technique. 17
For this follow-up study, patients with confirmed CAD and fully revascularized with percutaneous coronary intervention (PCI) were randomly included and re-examined with a second EST (EST2), at median 9 weeks after revascularization. Of these patients, 15 were treated with PCI on stenosis located on LAD and 5 patients with stenosis located on RCA. All were without any symptoms of angina pectoris in the follow-up period. Importantly, the EST2 test was performed at the same individual workload as EST1.
Blood Sampling and Laboratory Methods
Blood samples were collected prior to exercise (at rest) and within 5 min after termination of the EST at both examinations. Serum and citrated plasma were prepared within one hour by centrifugation 2000 × g for 10 min at room temperature and 2500xg for 20 min, respectively, and kept at − 80 °C until analyzed in batches. Conventional laboratory methods were used for routine analyses. cTnT was determined by electrochemical luminescence immunoassays Eleusis Troponin T hs STAT (Roche Diagnostics, Switzerland). In patients with levels below the lower limit of detection (3 ng/L), levels were set at 1.5 ng/L for purpose of statistical analyses. Inter assay coefficient of variation (CV) in our routine laboratory was 6% at the level of 13 ng/L. NT-proBNP was performed by electrochemical luminescence immunoassays Elecsys proBNP II (Roche Diagnostics, Switzerland). Lower detection level was 5 ng/L and the inter assay CV was ≤ 6%. The following commercially available enzyme immunoassays were used to determine levels of F1 + 2, D-dimer and TFPI: Enzygnost® F1 + 2 (monoclonal) (Siemens, Marburg, Germany), Asserachrom D-dimer (Stago Diagnostica Asniere, France), Asserachrom total TFPI antigen, recognizing full-length and truncated TFPI molecules (Stago Diagnostica), respectively. The inter assay CVs in our laboratory were 1.8, 1.2 and 3.6%, respectively. Endogenous thrombin potential (ETP) was determined by the Calibrated Automated Thrombogram (CAT) (Thrombinoscope BV, Maastricht, The Netherlands), and analyzed on the Fluoroscan Ascent fluorometer (Thermo Fisher Scientific OY, Vantaa, Finland). Final concentrations of 5 pM rTF, 4 μM phospholipids and 2.5 mM thrombin-specific fluorogenic substrate were used. To calculate the final results plasma samples were measured along with a thrombin calibrator. The software (Thrombinoscope BV, version 3.0.0.29) enabled calculation of the lag time (min), peak thrombin generation (PeakTG), ETP (nM·min) represented by area under the curve and time to peak (ttPeak) (min). Velocity Index (PeakTG/ttPeak-Lagtime) (nM/min), indicates the average net rate of prothrombin activation during the propagation phase. The inter assay CVs for the different CAT variables were 17.6%, 4.5%, 3.2% and 4.5%, respectively.
Statistical Analysis
Data was analyzed using IBM SPSS Statistics version 26.0. Laboratory values were mainly not normally distributed and are presented with median value, 25th and 75th percentiles. Continuous data are otherwise presented as mean and standard deviation, and categorical data are presented as numbers (%). Depending on distribution of the continuous data either Student T-test or Mann–Whitney U test were used for comparisons between groups, while Wilcoxon signed rank test was used for pairwise comparisons of continuous data within the groups. For assessment of categorical variables Chi-square test was used. P-value ≤ 0.05 was considered statistically significant.
Results
Table 1 shows the baseline characteristics of the study population (n = 20) at both examinations. The 20 included patients did not differ from the total population presenting with CAD in the main CADENCE study. 17 Median age was 62 years and 19 were male. EST2 was performed at a median of 66 days after revascularization. One patient used clopidogrel at EST1, and all patients at EST2. The exercise stress test results are shown in Table 2. At both tests median workload was 145 W and median exercise duration was 9:53 min:sec.
Characteristics of the Study Population (n = 20) at Both Examinations (visits)

Number (proportions) or median (25,75 percentiles) are given.
Abbreviations: PCI = Percutaneous Coronary Intervention, MI = Myocardial Infarction, ACE/ARB = angiotensin-converting enzyme inhibitor/angiotensin receptor blocker
Exercise Stress Test Results at Both Examinations (n = 20)
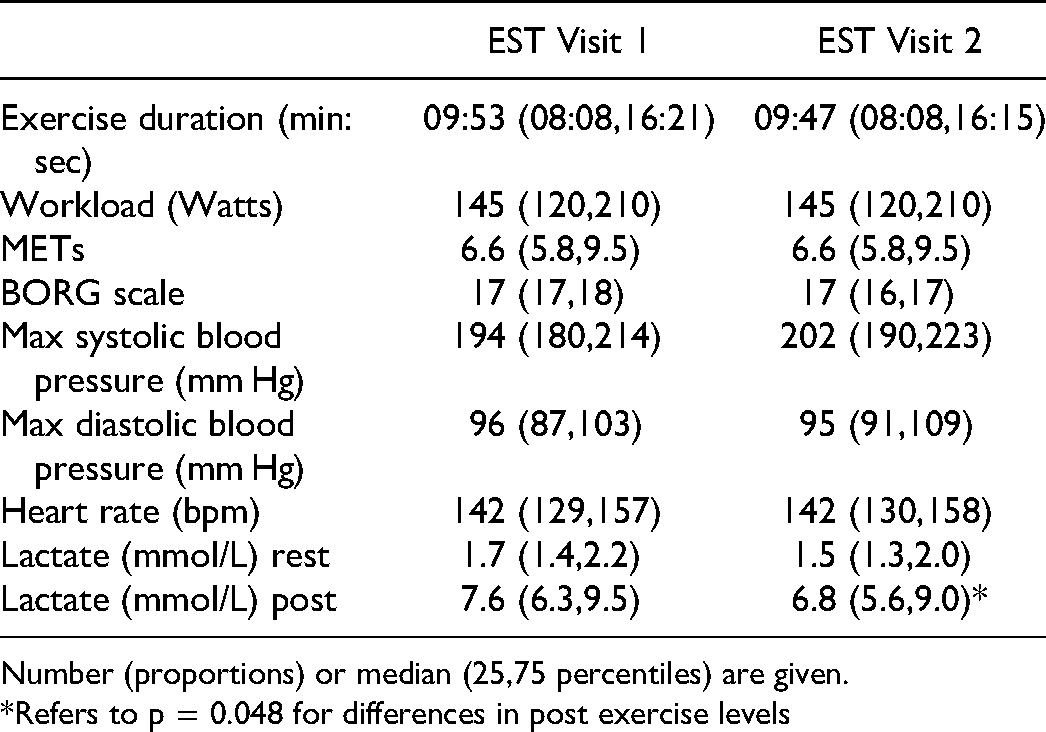
Number (proportions) or median (25,75 percentiles) are given.
*Refers to p = 0.048 for differences in post exercise levels
Cardiac Biomarkers
The results of resting and exercise induced cTnT and NT-proBNP at both examinations are shown in Figure 1. There was significant increase in cTnT and NT-proBNP from resting to post exercise levels at EST1, as expected (p < 0.01, both). Also at EST2, increased levels were observed (p < 0.01, both). However, the changes did not differ between EST1 and EST2 (p = 0.73 and p = 0.60, respectively). Resting levels of cTnT at EST2 were significantly higher compared to EST1 (median 8.1 vs 7.1 ng/L, p = 0.02), whereas resting levels of NT-proBNP did not differ (p = 0.68) between the examinations.

Resting (dark grey) and exercise induced (light grey) Troponin T (upper panel) and NT-proBNP (lower panel) levels at both examinations.
Prothrombotic Biomarkers
The resting and exercise induced levels of prothrombotic markers are shown in Table 3. Significant increase in D-dimer (p = 0.008 and <0.001), F1 + 2 (p = 0.009 and <0.001) and TFPI (p < 0.001 and 0.001) during exercise at both visits were demonstrated, with no differences in these changes. Resting levels of TFPI were lower at EST2 (p < 0.01) compared to EST1. There were no significant changes in ETP during exercise at any visit, but resting levels were lower at EST2 compared to EST1 (p < 0.01). Other specific variables from the CAT assay are shown in Supplementary Table 1. PeakTG and the velocity index did not change during the ESTs, but both were lower in resting state at EST2. Lagtime and ttPeak increased at both EST1 and EST2, with no differences in changes. Higher resting level of ttPeak was observed at EST2.
Resting and Exercise Induced Prothrombotic Markers at Both Examinations (visits)

Median (25,75 percentiles) are given.
p1: change during exercise at visit 1. p2: change during exercise at visit 2. Δ p: difference in exercise induced changes between the examinations.
*refers to p < 0.01 for difference between resting values.
Discussion
In this cohort of patients with CAD, we found that exercise induced release of cTnT and NT-proBNP was still significant 9 weeks after revascularization, as was also the increase in F1 + 2, D-dimer and TFPI. Resting levels of NT-proBNP were unchanged after revascularization, whereas cTnT levels were higher and ETP and TFPI levels were lower.
We have previously shown that resting levels of cTnT was significantly higher in the patients with confirmed CAD, 17 and the present results showing higher levels after revascularization, suggest this to be a perpetual condition in this subset of patients. To our knowledge, this has previously not been reported. Whether the rather small, although significantly increased, resting levels after revascularization have any clinical impact can be discussed. It may just be a sign of an ongoing disease as all patients had verified CAD. Nevertheless, previous findings have shown hs-cTnT above 5.7 pg/mL to reflect the severity of CAD22,23 and levels above 6 pg/mL to be predictive of CAD. 24 Somewhat in line with our results, Williams et al showed significant increase in resting TnT after revascularization in patients with stable angina pectoris, however, the blood samples were drawn only 18-24 hours after PCI. 25
Moreover, the exercise induced release of cTnT was found to be at the same magnitude 9 weeks after revascularization, which also can be discussed to be due to an ongoing disease development. Exercise induced release of cTnT in CAD patients has been shown in other studies, including our basis for the present investigation, 17 but somewhat dependent on the TnT assay used.2627 Increased levels several hours after an EST have also been shown.2829
The unchanged resting levels of NT-proBNP after revascularization support the suggestion that the CAD disease per se is present, although the stenosis has been treated. As ischemia in itself has been suggested to induce an increase in natriuretic peptides,30-32 our hypothesis was levels to be reduced after revascularization. NT-proBNP is stored in granules of cardiomyocytes only in a small amount, and upregulated genes with protein synthesis are therefore needed before a significant release. 33 Presumably patients with significant chronic CAD, revascularized or not, will have upregulated genes, implying sustained release in stable condition.
We have previously shown higher exercise-induced levels of NT-proBNP in patients with versus not verified CAD, but there are conflicting results from smaller studies. 19 Nevertheless, in the present small study, we could demonstrate significant increase during exercise, and the increase was not affected by revascularization. This may be due to ongoing disease, but also that the exercise induced levels more reflect release of the stored amount. 33
The prothrombotic markers increased significantly during exercise also after revascularization. This result was not quite unexpected, because we previously have shown such increase not to differ between patients with verified CAD versus those without among patients with symptoms of CAD. 20 Increased levels of D-dimer might be discussed to be due to an acute phase response that is independent of the patient condition, as this has also been shown in healthy individuals. 34 Based on the introduced antithrombotic treatment between the two EST measures, ie after revascularization, a reduced prothrombotic state could have been expected. Although the antithrombotic treatment was platelet inhibition, reduced platelet activation may induce a less hypercoagulable state. 35 Resting levels of ex vivo thrombin generation potential, were indeed significantly lower after revascularization, as was also PeakTG and the velocity index, suggesting less thrombin activation in resting state.
TFPI, being a main inhibitor of tissue factor, is released from endothelial cells under different stimuli and may thus be released upon endothelial activation. 20 The increase seen during both ESTs, may therefore be discussed to be exercise induced endothelial activation. This was not affected by the revascularization. In contrast, resting level of TFPI was significantly lower after revascularization, which indicate the endothelium to be less activated. As high levels of TFPI have been associated with high risk of CVD, 36 this may be considered a benefit, either related to the revascularization per se or to the introduced use of medications. 37 It might be speculated whether the increase in lagtime and ttPeak after exercise at both occasions may be a sign of reduced TF availability due to the increased levels of TFPI, although this was not reflected in exercise-induced thrombin generation as measured by ETP, F1 + 2 and D-dimer.
Limitations
A limitation of this study was the small sample size. Single blood sampling prevented us from studying the time-course of the measured markers. We can therefore not be sure to have measured peak values of the variables or transient changes. Accordingly, Axelsson et al who measured TnT immediately after termination and further every hour for 6 hours after termination of the EST, demonstrated the highest value to be 6 hours after the EST in CAD patients. 29
Conclusion
In patients with CAD, there was still significant increase in exercise-induced release of cardiac and prothrombotic biomarkers after revascularization, thus revascularization seems not to affect the ability to release these biomarkers. Also, the higher resting levels of cTnT after revascularization indicate that revascularization per se does not affect secretion of cardiac biomarkers, probably due to the disease state. The lower resting levels of TFPI and ex vivo thrombin generation potential after revascularization may, however, be indicative of less endothelial activation and reduced prothrombotic activity.
Supplemental Material
sj-docx-1-cat-10.1177_10760296221094029 - Supplemental material for Effect of Revascularization on Exercise-Induced Changes in Cardiac and Prothrombotic Biomarkers in Patients with Coronary Artery Disease
Supplemental material, sj-docx-1-cat-10.1177_10760296221094029 for Effect of Revascularization on Exercise-Induced Changes in Cardiac and Prothrombotic Biomarkers in Patients with Coronary Artery Disease by C. H. Hansen, J. Cwikiel, V. Bratseth, H. Arnesen, A. Flaa and I. Seljeflot in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgements
The authors thank medical technologists Sissel Åkra and Jeanette Steen at Center for Clinical Heart Research and Vibeke Kjær at Section of Cardiovascular and Renal Research for excellent assistance and laboratory analyses.
Author Contributions
CCH: Conceptualization, acquisition, statistical analysis, interpretation of data, original draft and editing. JC: Acquisition and interpretation of data, reviewing and editing the manuscriptVB: Laboratory analyses, interpretation of data, reviewing and editing the manuscript HA: Conceptualization, interpretation of data, reviewing and editing the manuscript AF: Conceptualization, interpretation of data, reviewing and editing the manuscript IS: Conceptualization, statistical analysis, interpretation of data, editing and final reviewing of the manuscript.
Availability of Data and Materials
The data sets used are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The authors confirm that all ethical guidelines are followed.
Funding
This work was supported by the Stein Erik Hagen Foundation for Clinical Heart Research, Oslo, Norway.
Informed Consent
All patients have given written, informed consent.
Trial Registration
clinicaltrials.gov, NCT01495091.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.