
Abstract
Background
Thrombotic events can increase the COVID-19 associated disease mortality. The administration of prophylactic anticoagulants had been shown to decrease the incidence of thrombosis, mortality, and ICU admission rates in COVID-19 patients.
Aims
The present study investigates the rate of thrombosis with early anticoagulation prophylaxis, the various risk factors for thrombotic events, and the overall survival rate in hospitalized COVID-19 cases.
Methods
In this prospective observational study, 425 patients aged ≥14 years were included in the study who were hospitalized with COVID-19 related symptoms from March to October 2020 at two tertiary care hospitals in the Kingdom of Saudi Arabia. Venous thromboembolism (VTE) score was evaluated, and VTE prophylaxis was administered according to the hospital guidelines. Patients’ demographics, comorbidities, disease presentation, and sequential hematological profiles were also recorded. Samples were collected at different time points to determine the hematological profiles.
Results
Out of 425 with positive COVID-19 subjects, eight (1.9%) patients developed thrombosis during admission, with pulmonary embolism being the most common type. VTE prophylaxis was administered to 394 (92.7%) patients. These anticoagulants included enoxaparin (86.3%), heparin (12.7%), warfarin (0.8%) and apixaban (0.3%). Comorbid conditions were recorded in 253 (59.5%) patients. ICU admission rate was 28% (n = 119), with a median time to transfer to ICU of 1 day (r: 0-33 days). A trend of high VTE score (5.0) with ICU admission and mortality (P = <.001) was observed. The observed mortality rate for our cohort was 5.9% (25 events out of 425); however, for patients admitted in ICU, it was 16% (19 events out of 119 admissions).
Conclusion
We are reporting a low incidence of thrombosis in COVID-19 patients. We have demonstrated that the early administration of prophylactic anticoagulants might reduce the risk of thrombotic events and the associated mortality. We observed a higher VTE score and thrombosis in patients admitted to the ICU.
Introduction
In Wuhan, China, a novel human coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) outbreak became a global pandemic in early 2020. The World Health Organization (WHO) named the disease Coronavirus disease of 2019 (COVID-19).1–7 Some 280 million confirmed cases of COVID-19 have been reported globally to date, causing close to 5.4 million deaths. 8 Several vaccines have been designed to combat the pandemic, with countries racing towards achieving vaccination targets. 8
Although COVID-19 is primarily a respiratory disease that can lead to pneumonia or acute respiratory distress syndrome, various non-respiratory manifestations have also been reported, including venous and thromboembolic events.9–12 COVID-19 induced thrombosis affects various, organs including the vasculature of lungs, 9 legs, 11 spleen, 10 heart, 13 and brain. 14 The thrombotic events can lead to high mortality in severe COVID-19 cases. 15 The clinical data reported to date indicates that the most frequently reported thrombotic events among COVID-19 patients are pulmonary embolism (PE) and deep vein thrombosis (DVT). 12 However, in hospitalized patients, the risk of venous thromboembolism (VTE) remains the highest.16–19 There are conflicting reports on the rate of VTEs in hospitalized patients with an estimated incidence of 12–28%. 20 In a multicenter Saudi study conducted on 636 COVID-19 patients, the rate of VTE was reported as 0.19% in the non-ICU group and 10.3% in ICU patients. The rate of arterial events was 0.94 % in non-ICU patients compared to 8.4 % in ICU groups. 21
The administration of prophylactic anticoagulants had been shown to decrease VTE incidence, mortality, and admission to the ICU in severe COVID-19 patients.22,23 In the earlier days of the pandemic, conflicting data were reported on the dose of anticoagulation, making a case for prophylactic versus intermediate or full dose. 21
Several mechanisms have been proposed to be associated with SARS-CoV2 infection that may cause thrombosis. 24 The levels of various markers in COVID-19 patients are altered, including leucocyte count, lymphocyte count, and platelet count. 25 The levels of coagulation markers have also been reported to differ among COVID-19 patients and non-COVID-19 patients, especially with ARDS. 26 Various preclinical probability scores like DIC & VTE have shown value in predicting the clinical severity and thrombosis. The present study investigates the rate of thrombosis, the various risk factors for thrombotic events, and the overall survival rate in hospitalized COVID-19 cases.
Methods
Study Design and Participants
After appropriate approval by the Institutional Review Board of both centers, a prospective observational study was carried out. We included 425 adolescent and adult (age ≥14 years) patients who were hospitalized mainly with COVID-19 related symptoms from March to October 2020 at two tertiary care hospitals in the Kingdom of Saudi Arabia (KSA),
Data Collection
According to the hospital guidelines, each admitted patient underwent evaluation for a VTE score 27 and received VTE prophylaxis (Table 1). Patients’ data were measured upon admission on demographics, details on symptoms, COVID-19 stage, sequential hematological profiles, VTE prophylaxis, and score, treatment, and outcome were recorded throughout their stay at the hospital. Comorbidities, including cancer, hyperlipidemia, hypertension, and diabetes, were defined according to the medical history, body mass index (BMI), and mortality rate at day-30. Samples for special coagulation tests were collected on admission to the hospital.
Hospital guidelines for VTE prophylaxis

Laboratory Analysis
Samples were collected at admission, days 3, 7, and 14 for those staying up to 14 days. All our patients had 10 cc of EDTA, 10 cc of Citrated blood (at 3.2%), and 5 cc sodium heparin collected. CBC was tested from the EDTA samples using an automated SYSMEX XN-10 instrument (Sysmex Corporation, Kobe, Japan), while automated chemistry analyzer COBAS 601 (Roche Diagnostics, Basel, Switzerland) was used to measure serum creatinine and C reactive protein.
The samples for coagulation tests were centrifuged within two hours and aliquoted for testing different coagulation markers, including PT / INR, aPTT, D-dimer, and fibrinogen (FIB) done at all four time-points, while antithrombin (AT), protein C (PC), protein S (PS), von Willebrand factor antigen (vWFAg) and factor VIII (FVIII) activity were done at admission to hospital using STAR Max® (Diagnostica Stago, Marseille, France).
COVID-19 Stages
To explore the correlation between disease severity and coagulation markers, we used a hospital-based clinical staging system for COVID-19 to assess disease severity. The system divides patients into stages A to D, as summarized in Table 2.
Hospital based clinical staging system for COVID-19 to assess disease severity

Statistical Analysis
After performing quality checks on the dataset, descriptive statistics were calculated using developed algorithms for missing and abnormal values. Measures on continuous variables were provided as median with range for data not conforming to normality assumptions and categorical variables as number and percentage. Chi-square test or Fisher's exact test were used to analyze the association between the categorical variables. Independent-samples Mann-Whitney U Test and Kruskal-Wallis Test were used to test for the significance of the difference between two and more categories of continuous variables. Cut-off values of the parameters were calculated using Youden's criterion. All statistical analysis was performed using IBM-SPSS (version 20.0) and R (version 4.0.5) with R Studio (version 1.1.456). P–value threshold of less than .05 was considered statistically significant. No imputation for missing data
Results
The median age in our cohort was 52 years (range “r’: 14-92 years). Out of 425 patients admitted to the hospital with positive COVID-19 diagnosis, 227 male patients accounted for 53.4%, with the male to female ratio of 1:0.9. Only 34 (8%) were asymptomatic at presentation admitted for observation due to various medical reasons. Respiratory-related symptoms were the most common (n = 293, 68.9%), followed by fever (n = 266, 62.6%), and GIT symptoms (n = 120, 28.2%). Co-morbid conditions were recorded in 253 (59.5%) patients, with hypertension being the commonest (n = 171, 40.2%). Twenty-nine (6.8%) of our patients had cancer. COVID-19 stage B was the most common stage at the presentation time (n = 200, 47.1%). ICU admission rate was 28% (n = 119), with a median time to transfer to the ICU of one day (r: 0-33 days). The median ICU stay was 9 days (r: 1-115 days). Patients’ demographic, clinical characteristics and prophylaxis incidence of thrombosis, and survival outcome are presented in Table 3. The overall mortality rate for our cohort was 5.9% (25 events out of 425); however, for patients admitted to the ICU, it was 16% (19 events out of 119 admissions).
Demographics, treatment, and outcome parameters of COVID-19 infected patients.

Note: Data are presented as median (minimum-maximum) for continuous variables and number (percentage) for discrete measurements.
Abbreviations: DIC, disseminate intravascular coagulopathy.
VTE Score, Anticoagulation Prophylaxis and Thrombosis
VTE score was calculated for all admitted patients on admission, days 3, 7 and 14. A trend of high VTE score (5.0) with thrombosis (P = .051), ICU admission, and mortality (P < .001, respectively) was observed (Supplement Table-B). Eight (1.9%) patients developed thrombosis during admission. The type of thrombosis was pulmonary embolism in 4 patients, while others had thrombosis in the inferior vena cava, internal jugular, and portal vein, with one patient having a stroke. Three out of five patients with thrombosis who were admitted to the ICU, the thrombotic event was documented 7 days after ICU admission, while for one patient it occured within 3 days of admission and for the other it was on the same day. According to hospital guidelines, VTE prophylaxis was administered to 394 (92.7%) patients: enoxaparin to 340 (86.3%), heparin to 50 (12.7%), warfarin to 3 (0.8%), and apixaban was given to 1 (0.3%) patient.
Incidence of thrombosis was significantly associated with ICU admission and high DIC and VTE scores (Supp B). Factors like elevated d-dimer, higher BMI, platelets >450 × 109/L, advanced age with comorbid conditions, and being symptomatic at admission were significantly associated with ICU admission during hospital stay (Table 3).
Hematological parameters, including platelet count, prothrombin time (PT), antithrombin levels, protein S level, protein C levels, d-dimer, soluble fibrinogen (FIB), factor VIII (FVIII) levels, and von Willebrand factor (VWF) antigen levels at the time of hospital are listed in Table 4.
Hematological and coagulation related parameters at admission of COVID-19 infected patients
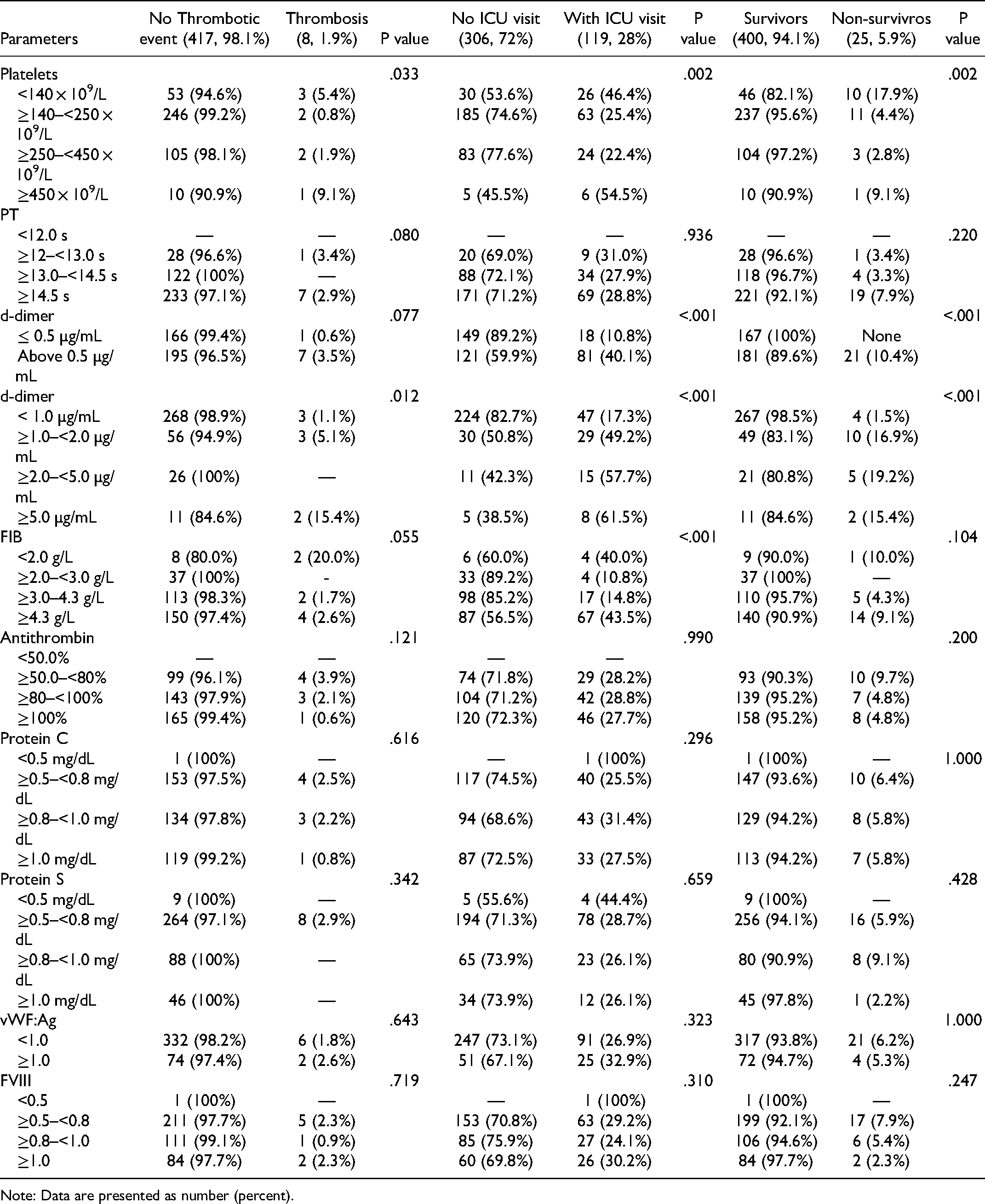
Note: Data are presented as number (percent).
Overall Outcome
Besides older age and having an ICU visit, patients presenting with comorbid conditions, especially diabetes and malignancy, higher COVID-19 stage, having DIC score of 4 or above, higher VTE score, d-dimer and fibrinogen, and platelets below 140 × 109/L were significantly associated with mortality (Tables 3 and 4).
400 (94.1%) patients in our cohort survived. Of the 425 patients, 306 did not require ICU admission, while 417 did not report any thrombotic events. The median BMI of our cohort was 28.4, with an elevated BMI of 38.4 in patients reporting thrombosis. The comorbidities observed in our cohort were hypertension (40.2%), diabetes (36.5), hyperlipidemia (18.1%), malignancy (6.8%), previous VTE (1.6%), and bleeding (0.5%). Pre-existing comorbidities were a significant risk factor for mortality (P–value .036), with diabetes (P–value .050) and malignancy (P–value .021) being the most significant risk factors. Stage B was the most common disease presentation. However, in patients with thrombosis, the most common presentation was stage D. Stage of the disease, ICU admission, and DIC score were associated with determining the risk of a fatal outcome (P–value <0.001). We found that the cut-off value of 1.2 for INR, 4 for DIC, and 5 for VTE score had higher sensitivity & specificity to predict mortality. Enoxaparin was observed to be the most effective prophylactic treatment to prevent death (P–value <.001).
Laboratory Changes
Platelet count was ≥140 × 109/L–<250 × 109/L for most of our cohort with no thrombotic event. In 3 out of 8 patients with thrombosis, the platelet count was <140 × 109/L. D-dimer level was >0.5–<1.0 µg/mL in 3 patients with thrombosis, ≥1.0–<2.0 µg/mL in another 3 patients, while 2 patients had level >5 µg/mL. The details of hematological markers are presented in Table 4. Platelet count was significantly associated with thrombosis risk (P–value .033), ICU admission (P–value .002), and mortality (P–value .002). FIB level was associated with ICU admission (P–value <.001) and thrombosis risk
WBC count, neutrophil count, lymphocytes count did not change significantly from the time of admission to day-7 but increased significantly from day 7 to 14. Platelet count increased gradually from the time of admission to day-14. There was a significant increase in the levels of C reactive protein, creatinine, monocyte count, PT, and PTT from the time of admission to day-14. Fibrinogen level declined during the hospital stay. HgB count and INR didn't change significantly throughout the study. The trends observed in hematological markers are summarized in Supplement table A.
Discussion
There is reported male preponderance reflecting more severe disease and an increased tendency for coagulopathy among males.28–30 Likewise, we observed male preponderance in our cohort with 53.4% males. Initial reports on COVID-19 have shown male preponderance, 31 increased risk of mortality due to COVID-19,28,32 and increased prevalence of comorbidities such as cardiopulmonary diseases. Male patients, especially from advanced age groups, are also at increased risk of extended hospital stays and a slower recovery. 33 ACE-2 expression differences have been proposed to mediate the risk and severity of COVID-19 based on gender, 34 however, further studies are required to confirm this proposition. Another molecular factor that has been proposed to mediate the disease severity of COVID-19 among elderly males is testosterone. 35 However, the precise mechanisms that control the gender-based risk and severity of COVID-19 have yet to be deciphered.
There are varied reports on the incidence of thrombosis among hospitalized COVID-19 patients, as high as 28%. 20 The incidence of thromboembolism was 31% in a Dutch ICU-admitted population. 36 However, we found a much lower incidence of VTE (n = 8, 1.9%) in our cohort. Our study further investigated the incidence of thrombosis and overall survival for hospitalized patients with COVID-19. The risk of VTE events remains the highest in hospitalized patients,16–19 with VTE incidence in those patients ranging between 12–28%. 20 In a multicenter Saudi study conducted on 636 COVID-19 patients, the risk of VTEs was higher in ICU patients (10.3%) than non-ICU group (0.19%). In the same study, the rate of arterial thrombotic events was 0.94 % in non-ICU patients compared to 8.4 % in the ICU group. 21 Tang et al has reported that only 0.6% of survivors met the criteria of disseminated intravascular coagulation (DIC) compared to 71.4% of non-survivors. 22 In a retrospective study that included 6153 patients, the risk of VTE was 7.2% in patients requiring mechanical ventilation, <1% in hospital-discharged patients, and 0.14% after a single ER visit. 37 Likewise, our cohort also showed higher trends of VTEs and associated mortalities in hospitalized patients. In total, eight (1.9%) patients developed thrombosis during admission, with four events of pulmonary embolism. The remaining four thrombotic events were observed in the inferior vena cava, internal jugular, and portal vein, with one patient having a stroke. We observed that the incidence of thrombosis was associated with the ICU admission, higher DIC and VTE score, d-dimer, BMI, COVID-19 stage, platelet count of >450 × 109/L, age, comorbid conditions, and being symptomatic at the time of hospital admission. This contrasts with a previous study that reported a lack of association between clinical pulmonary thromboembolism in patients at the ICU with D-dimer, CRP, and ferritin levels. 38
The administration of prophylactic anticoagulants had been shown to decrease the VTE incidence, mortality, and admission to the ICU in severe COVID-19 patients who have met the sepsis-induced coagulopathy (SIC) criteria or have markedly elevated D-dimers. 22 In another study conducted on the Caucasian population, the risk of thrombosis was significantly reduced by thromboprophylaxis. 39 The American Society of Hematology (ASH) guideline panel has suggested the use of prophylactic-intensity for critically ill and acutely infected COVID-19 patients without any suspected or confirmed VTE. 40 According to the hospital guidelines, the VTE prophylaxis was administered to 394 (92.7%) patients in our cohort. Using these anticoagulant agents was probably associated with reduced thrombotic events and mortality rates in our cohort compared to previous studies reporting thrombotic events and mortality rates in patients visiting hospitals due to COVID-19. Previously reported studies suggested that using these anticoagulants can significantly improve the disease prognosis and reduce COVID-19 mortality. Administration of therapeutic-dose anticoagulation with heparin or usual care pharmacological thromboprophylaxis in 2219 patients showed an increased probability of survival to hospital discharge with reduced use of organ support. 41 In another multicenter study conducted worldwide, similar results were replicated. Three clinical trial platforms spanning five continents in more than 300 hospitals observed the effects of full doses of heparin in 1000 moderately ill COVID-19 patients. 42 The use of doses other than standard-dose prophylactic anticoagulant did not show any significant differences in the primary outcome of a composite of adjudicated venous or arterial thrombosis, treatment with extracorporeal membrane oxygenation, or mortality within 30 days. 43 Race and ethnicity have major effects on thrombotic risk.44,45 However, the studies published for evaluating the role of thromboprophylaxis in reducing the risk of thrombosis in COVID-19 from around the globe have shown promising results for all populations. Considering these studies and our findings, we propose using thromboprophylaxis in all hospitalized COVID-19 patients.
Most of our patients presented with mild to moderate symptoms, however, the ICU admission rate was 28%, much higher than pooled ICU admission rates of 10.9%. 46 The global mortality rates have been reported to be around 3.4% in a media briefing on COIVD-19 on March 3, 2021. 47 The pooled mortality rate from 23 studies was reported to be 4.3 (95% CI: 1.0-9.1). The overall mortality rate for our cohort of patients was 5.9%, slightly higher than the reported data. However, we were examining only patients with hospital visits, and therefore the mortality rate is only for the hospitalized patients. Grasselli et al 48 reported the mortality rates in hospital and ICU-admitted patients of 12 (95% CI: 11-12) and 27 (95% CI: 26-29) per 1000 patient-days, respectively, with 53.4% deaths in the ICU-admitted patients.
Conclusion
COVID-19 patients, especially those admitted to ICU, are at higher risk of thrombosis, leading to increased mortality. The administration of prophylactic anticoagulants can reduce the risk of thrombotic events and the associated mortality. Various trials are being conducted worldwide to further explore therapeutic options that can help determine an optimal dose. Patient-specific dose determination can also be employed for further reducing the risk of any thrombotic event in patients with comorbidities.
Supplemental Material
sj-docx-1-cath-10.1177_10760296221086286 - Supplemental material for Report of Low Incidence of Thrombosis with Early Prophylaxis in Hospitalized Patients with COVID-19 from Two Saudi Tertiary Centers
Supplemental material, sj-docx-1-cath-10.1177_10760296221086286 for Report of Low Incidence of Thrombosis with Early Prophylaxis in Hospitalized Patients with COVID-19 from Two Saudi Tertiary Centers by Tarek Owaidah, Khalid Maghrabi and Feras Alfraih, Alfadil Haroon, Khawar Siddiqui, Randa Alnounou, Hadeel AlOtair, Fatmah S Alqahtany, Mohannad Maghrabi, Mustafa Owaidah, Khalid AlSaleh in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-pdf-2-cath-10.1177_10760296221086286 - Supplemental material for Report of Low Incidence of Thrombosis with Early Prophylaxis in Hospitalized Patients with COVID-19 from Two Saudi Tertiary Centers
Supplemental material, sj-pdf-2-cath-10.1177_10760296221086286 for Report of Low Incidence of Thrombosis with Early Prophylaxis in Hospitalized Patients with COVID-19 from Two Saudi Tertiary Centers by Tarek Owaidah, Khalid Maghrabi and Feras Alfraih, Alfadil Haroon, Khawar Siddiqui, Randa Alnounou, Hadeel AlOtair, Fatmah S Alqahtany, Mohannad Maghrabi, Mustafa Owaidah, Khalid AlSaleh in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Authors’ Contribution
TO & MS designed & developed the study. Both authors were responsible for content & authenticity. AMA, AA, KM, MO oversaw data collection, data entry. KS, KA & RA carried out a final review of data and analysis. All authors were responsible for the direction of the study team and the facilitation of the project plan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review Board of King Faisal Specialist Hospital and Research Centre, Kingdom of Saudi Arabia, under approval # RAC KFSHRC (2201086).
Informed Consent
All authors consent for publication.
Trial Registration
Availability of Data and Materials
Furnished upon request.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.