
Abstract
Objective
The present study aimed to investigate the application safety of bivalirudin combined with ticagrelor in the emergency percutaneous coronary intervention (PCI) in patients with ST-segment elevation myocardial infarction (STEMI).
Methods
From October 1, 2018, to December 30, 2019, 210 patients with STEMI admitted to the Department of Cardiology who underwent emergency PCI were randomly divided into the bivalirudin group (group A, N = 105) and the unfractionated heparin group (group B, N = 105). Before the emergency PCI operation after admission, the loading dose of aspirin (300 mg) was given orally, and then 100 mg/d. At the same time, the loading dose of ticagrelor (180 mg) was administered orally, and then 90 mg/bid. The adverse events and the hemorrhage events 30 days after the operation were observed and recorded.
Results
There were five hemorrhage cases in the bivalirudin group, with one case of secondary hemorrhage and four cases of mild hemorrhage. There were 14 hemorrhages in the unfractionated heparin group with one case of secondary hemorrhage and thirteen cases of mild hemorrhage. In terms of mild hemorrhage, the hemorrhage rate in the bivalirudin group was significantly lower than that in the unfractionated heparin group (3.8% vs. 12.4%, P = 0.040). One patient died in the unfractionated heparin group, while no deaths occurred in the bivalirudin group during the thirty days of follow-up. No myocardial infarction, revascularization, or stroke occurred in the two groups within 30 days after the operation.
Conclusion
Compared with unfractionated heparin combined with ticagrelor in patients with STEMI undergoing emergency PCI treatment, bivalirudin combined with ticagrelor could significantly reduce the occurrence of mild hemorrhage events, and it would not increase the incidence of MACE during the 30 days of follow-up.
Introduction
Percutaneous coronary intervention (PCI) is the most direct and effective treatment method to improve coronary blood flow. Activation the coagulation system and intraoperative balloon expansion and placement of stents extruding the unstable coronary plaque. Effective intraoperative anticoagulation therapy has become important for the success of the operation. For all patients suspected of acute coronary syndrome (ACS), aspirin is recommended, unless it is contraindicated. Currently, almost all patients with acute ST-segment elevation myocardial infarction (STEMI) should take aspirin, 1 together with the administration of another antiplatelet drug (such as ticagrelor). Antiplatelet therapy is also recommended at the same time as anticoagulation therapy. 2 A prospective study showed that compared with clopidogrel, ticagrelor could reduce the mortality in the long term and the incidence of major cardiovascular adverse events (MACE) in the short term. 3 Among patients with ACS undergoing PCI, there was no significant difference in the incidence of MACE between ticagrelor and prasugrel. 4 Aspirin, combined with ticagrelor, could effectively relieve angina pectoris, reduce adverse reactions, reduce the levels of myocardial enzymes, and reduce the occurrence of acute postoperative thrombosis.5,6 For specific patients who cannot take the dual antiplatelet agents, compared with the clopidogrel monotherapy, patients who use ticagrelor alone have a reduced risk of cardiovascular events without increasing the risk of hemorrhage.7,8
A study that included 5961 patients to observe the effects of post-PCI ischemic and hemorrhage events on the prognosis suggested that post-PCI hemorrhages and perioperative myocardial infarctions were independently correlated with the increase in the one-year mortality. 9 In clinical practice, most patients undergoing PCI have ischemic factors as well as a high risk of hemorrhage. In particular, patients with renal insufficiency, old age, and chronic heart failure have a significantly higher incidence of hemorrhage events and all-cause deaths than in other patients. 10 A study has shown that most high-risk patients with thrombosis also had a high risk of hemorrhage. 11 Once a patient has a hemorrhage event after PCI, it will increase the psychological burden and, at the same time, increase the probability of death. Another study found that the post-PCI hemorrhage events were significantly associated with increased all-cause mortality in patients with hemodialysis. 12
As an indirect inhibitor of thrombin, unfractionated heparin is first synthesized into glycoprotein through the metabolism in the liver, 13 and further combines with antithrombin to form a heparin-antithrombin complex, and then combines with the thrombin catalytic site to exert an action.14–16 During the medication of heparin, if thrombocytopenia occurs in the patient, it will greatly increase the risk of hemorrhage and death. 17
As a synthetic thrombin direct inhibitor, bivalirudin does not require the metabolism in the liver, and can directly bind with thrombin to exert an action. Bivalirudin is reversibly dissociated under the action of proteolysis and is excreted by the kidney through proteolysis. Thus, it has the characteristics of quick onset and quick excretion. A study suggested that the application of direct thrombin inhibitors during the catheter ablation was safe and effective, and could be used as an alternative therapy to heparin. 16 A retrospective analysis showed that among patients with ECMO, there was no difference between heparin and bivalirudin in the incidence of thrombosis, major hemorrhage, and death. 18 There was also a study suggesting that the significant advantage of bivalirudin was reflected in the occurrence of adverse clinical events (including hemorrhage and MACE). 19 Some researchers have found that compared with heparin, the use of bivalirudin during PCI may increase the risk of cardiovascular death in patients, although this difference is not statistically significant. 13 Currently, controversy exists over the application of bivalirudin in PCI.
The purpose of the present study was to observe the application of bivalirudin combined with ticagrelor in the emergency PCI in patients with STEMI, and to further explore the effect of the thrombolysis in myocardial infarction (TIMI) blood flow classification, MACE events, and hemorrhage events after PCI, so as to investigate the effect of bivalirudin combined with ticagrelor on hemorrhage in short-term clinical treatment for patients with STEMI.
Materials and Methods
Study Objects
In the present study, the data of patients with STEMI who were admitted to the Cardiovascular Intensive Care Unit of the First People's Hospital of Yulin from October 1, 2018, to December 30, 2019, were collected. All the patients signed an agreement to undertake the emergency PCI. The study protocol had been approved by the Medical Ethics Committee of Yulin First People's Hospital, and the patients understood the research and signed informed consent. A total of 210 patients with STEMI were enrolled. According to the order of patients admitted to hospital, the random number table was used to assign the patients into the bivalirudin group (Group A) and unfractionated heparin group (Group B).
Diagnostic Criteria
The diagnostic criteria of STEMI 20 were as follows: (1) Patients with chest pain; (2) Patients with newly-onset changes of ischemic ECG. The specific ECG changes were ST-segment arched-up elevation (part of the ECG was a single-phase curve), related leads with or without pathological necrosis Q wave, a decrease of the amplitude of R wave (if there existed the myocardial infarction of the posterior wall, ST-segment changes might be atypical), often accompanied by mirror ST-segment depression in the corresponding leads; (3) Patients with newly-onset pathological Q wave; (4) When compared with previous imaging, new imaging revealed the new-onset defect of the survival myocardium or abnormal segmental motion of the ventricular wall; (5) Patients with confirmation of the presence of coronary thrombosis by coronary angiography or intracavitary imaging; (6) Patients with elevated troponin.
Patients with a sufficient combination of the symptoms and ECG to confirm the diagnosis of STEMI could be given reperfusion and other related treatments without waiting for the results of myocardial injury markers or imaging. The examination of myocardial injury markers was routinely recommended.
The Inclusion and Exclusion Criteria
Inclusion criteria:
Inquiry about the medical history to confirm that the onset of symptoms of chest pain and chest tightness was less than 12 hours;
The diagnosis was in accordance with those of STEMI based on medical history, combined with ECG and other auxiliary examinations;
The patient signed and agreed to undertake coronary angiography and emergency PCI after coronary angiography;
Exclusion criteria:
Patients with a history of intravenous thrombolytic therapy before admission or the onset time was more than 12 hours;
Patients with poor cardiac function (Killip grade > 2) or acute left heart failure, high risk of surgery, and who were not suitable for emergency PCI;
Patients who received intravenous infusions of GPIIb/IIIa receptor antagonists before and after PCI;
Patients with a confirmed history of aortic dissection, malignant tumors, or severe trauma, or hemorrhage in the digestive tract within three months;
Patients with a hypertensive crisis after admission and with poor control of blood pressure under drug therapy;
Patients with a confirmed history of atrial fibrillation without standardized treatment;
Patients with previous adverse reactions such as an allergy to the anticoagulant drugs and antiplatelet drugs;
Patients currently participating in another clinical trial.
Experimental Drug
Ticagrelor tablets, specification: 90 mg/tablet, manufactured by AstraZeneca Pharmaceutical Co., Ltd (Jiangsu), drug batch number: H20171080. Aspirin enteric-coated tablets, specification: 100 mg/tablet, batch number: J20130078, manufactured by Bayer Healthcare Co., Ltd Heparin sodium injection, specification: 1250U/injection, batch number: H32020612, manufactured by Jiangsu Wanbang Biochemical and Pharmaceutical Group Co., Ltd Bivalirudin, specification: 0.25 g/injection, batch number: H20140057, manufactured by Jiangsu Haosen Pharmaceutical Group Co., Ltd
Study Design
Before the emergency PCI operation after admission, the loading dose of aspirin (300 mg) was given orally, and then 100 mg/d. At the same time, the loading dose of ticagrelor (180 mg) was administered orally, and then 90 mg/bid. During the interventional treatment, all patients were treated with the Seldinger approach via the right radial artery or femoral artery. The PCI operation in each patient was completed by two experienced physicians with qualifications in coronary intervention surgery.
Bivalirudin group (Group A): Before PCI, 0.75 mg/kg of bivalirudin was injected intravenously, and then 1.75 mg/kg/h of bivalirudin was infused intravenously with a micropump until 3–4 hours after surgery.
Unfractionated heparin group (Group B): Before PCI, 100 U/kg of unfractionated heparin was injected. With stent implantation, coronary angiography should be performed to assess the criminal coronary artery. If the angiography of the criminal coronary artery suggested that the blood flow was slow and had no-reflow, Sodium nitroprusside(200ug/ time), nitroglycerin (200ug/ time), and Nicodil (2 mg/ time) should be given immediately for treatment. Then the coronary angiography should be performed again. Finally, the classification of the blood flow of the criminal vascular was evaluated. Anticoagulant drugs were discontinued 4 hours after surgery.
Observation
The blood flow of the criminal coronary artery before and after surgery
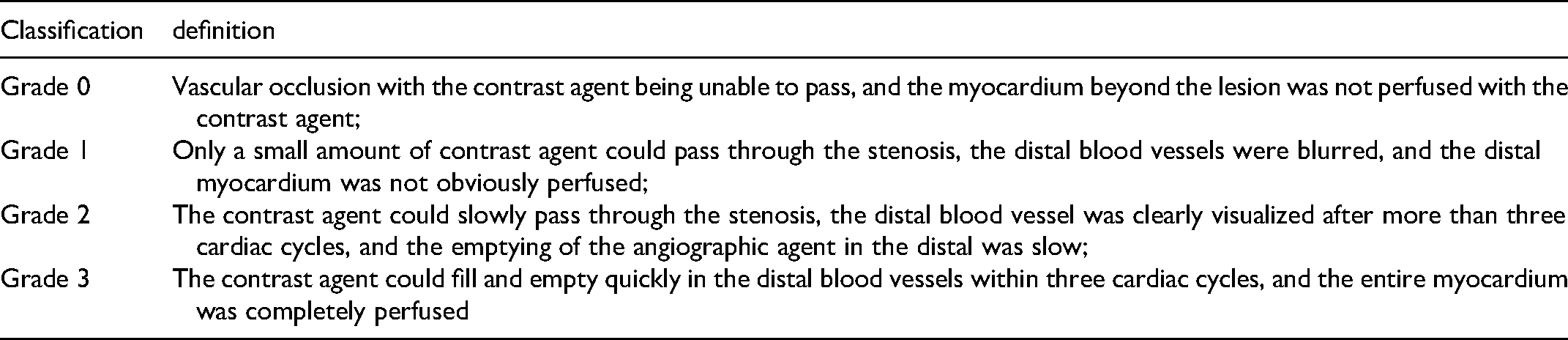
The coronary blood flow classification method of TIMI was proposed in the 1980s, and it is still used in clinical practice. According to the TIMI blood flow classification, the blood flow was divided into four grades. 21 The details are illustrated in Table 1.
The coronary blood flow classification method of TIMI.
MACE events and hemorrhage events 30 days after emergency PCI in patients through outpatient follow-up and telephone follow-up
The MACE events included the revascularization of the target vessel (re-PCI or coronary artery bypass grafting), stroke, non-fatal myocardial infarction, and death.
The hemorrhage events included primary hemorrhage, secondary hemorrhage, mild hemorrhage. 22 The details are illustrated in Table 2.
Hemorrhage events and treatments.

Statistic Analysis
SPSS 22.0 software was used for data analysis in the present study. The χ2 test or Fisher's exact probability test was used for enumeration data and expressed as a percentage (%) and cases. For comparison of measurement data between groups, the t-test was adopted, and mean ± standard deviation (
Results
Comparison of the Baseline Data Between the two Groups
In the present study, a total of 210 patients with STEMI were enrolled. The random number table was used to assign the patients into the bivalirudin group and the unfractionated heparin group. There were 105 patients in both groups. Drug-eluting stent was used in both groups. No patients in either group were lost during the observation and follow-up period in the present study and were closely followed up. The statistic results showed that there was no statistical difference in the clinical characteristics such as gender, age, previous history of hypertension, diabetes, and personal history of smoking, classification of cardiac function, and the time required for the patient to progress from the door of the hospital to the balloon expansion during the PCI (D2B) between the bivalirudin group and unfractionated heparin group (P > 0.05 in all). The details are illustrated in Table 3.
Comparison of the general characteristics including age, past history and so on between the two groups.

Note: RCA referred the right coronary artery, LCX referred the left coronary circumflex, LM referred the left main branch, LAD referred the left anterior descending coronary artery, D2B referred the time required for the patient from the door of the hospital to the balloon expansion during the PCI.
Comparison of the Coronary TIMI Blood Flow Classification of the Criminal Artery After Emergency PCI Between the two Groups
Through the analysis of coronary angiographic results, the blood flow of the criminal coronary artery before coronary PCI was compared between the two groups. The TIMI blood flow classifications of the criminal coronary artery before the surgery in the bivalirudin group were as follows: 64 cases in grade 0, 12 cases in grade 1, nine cases in grade 2, and 20 cases in grade 3. In the unfractionated heparin group, the blood flow classifications before surgery were as follows: 73 cases in grade 0, six cases in grade 1, seven cases in grade 2, and 19 cases in grade 3. There was no statistical difference in the classifications of the TIMI blood flow of the criminal coronary artery before the coronary PCI between the bivalirudin group and the unfractionated heparin group (P > 0.05).
The blood flow of the criminal coronary artery after the coronary PCI was compared between the two groups. The TIMI blood flow classifications of the criminal coronary artery after surgery in the bivalirudin group were as follows: zero cases in grade 0 and zero cases in grade 1, three cases in grade 2, and 102 cases in grade 3. In the unfractionated heparin group, the blood flow classifications before surgery were as follows: zero cases in grade 0 and zero cases in grade 1, three cases in grade 2, and 102 cases in grade 3. There was no statistical difference between the two groups (P > 0.05). The details are illustrated in Table 4.
Comparison of the TIMI blood flow of the criminal coronary artery after the emergency PCI between the two groups.

Note: PCI, Percutaneous coronary intervention; TIMI, thrombolysis in myocardial infarction; A = Bivalrudine, B = Unfractionated heparin.
MACE Event 30 Days After Emergency PCI
Through the 30 days of outpatient and telephone follow-up after surgery, one patient died in the unfractionated heparin group, while no deaths occurred in the bivalirudin group, and no other adverse clinical event occurred. There was no statistical difference in death, myocardial infarction, or revascularization between the bivalirudin group and the unfractionated heparin group. The comparison of mortality between the two groups was 0.0% vs. 1.0% (P = 1.000). The details are shown in Table 5.
Comparison of MACE in patients between the two groups.

Note: A = Bivalrudine, B = Unfractionated heparin; MACE, major cardiovascular adverse events.
Hemorrhage Event 30 Days After Emergency PCI
No major hemorrhage occurred in the bivalirudin group and unfractionated heparin group 30 days after surgery under close follow-up. A total of five patients in the bivalirudin group had hemorrhage events, including one patient with secondary hemorrhage. With the occurrence of hemorrhage, close attention was paid to the patient to observe changes in condition. The cause of the hemorrhage was hemorrhoid bleeding. The routine blood test after the hemorrhage was as follows: hemoglobin 160 g/l, hematocrit 0.484 (the hemoglobin was 172 g/l and hematocrit was 0.510 at admission). The antiplatelet therapy with ticagrelor and aspirin continued, while antacids were used to suppress the secretion of acid and protect the stomach, together with local hemostasis treatment. The hemorrhage improved, and the results before discharge were as follows: hemoglobin 163 g/l, hematocrit 0.497. All four cases with mild hemorrhage (two cases with gum hemorrhage and two cases with puncture hematoma) improved spontaneously. In the unfractionated heparin group, there were 14 hemorrhage events and one case of secondary hemorrhage with the symptom of hematemesis. The routine blood test after the hemorrhage was as follows: the lowest level of hemoglobin was 117 g/l, and the hematocrit was 0.327 (the hemoglobin was 157 g/l and hematocrit was 0.454 at admission). Ticagrelor was continued in the antiplatelet therapy, and symptoms improved with the administration of omeprazole. The hemoglobin was 122 g/l, and hematocrit was 0.348 at re-examination. There were 13 cases with mild hemorrhage (three cases with gum hemorrhage, one case of vaginal bleeding, one case of conjunctival hemorrhage, one case of epistaxis, and seven cases of puncture hematoma). Mild hemorrhage events in the bivalirudin group were significantly less than those in the unfractionated heparin group, and the difference was statistically significant (3.8% vs. 12.4%, P = 0.040). The details are illustrated in Table 6.
Comparison of the hemorrhage event between the two groups (Case,%).
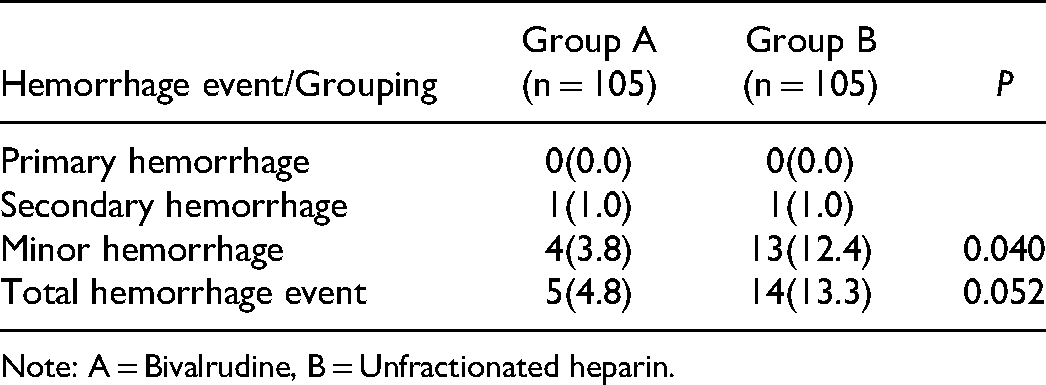
Note: A = Bivalrudine, B = Unfractionated heparin.
Discussion
Atherosclerotic diseases include coronary atherosclerosis (such as coronary heart disease), cerebrovascular disease (such as stroke), and peripheral vascular disease (such as arterial occlusion), and are the important causes of death.23,24 Coronary reperfusion therapy is the key to the successful treatment of acute myocardial infarction. Drug thrombolysis significantly reduces the mortality of patients with acute myocardial infarction. 25 PCI technology, which has features that traditional coronary artery bypass grafting does not have, including the small trauma, high recanalization rate of the affected vessels, and low risk of hemorrhage, makes it the preferred treatment for patients with STEMI.
The mechanism of no-reflow during the PCI may be correlated with vascular endothelial injury, thromboembolism, vasospasm, and so on. The formation of micro-thrombosis is closely correlated with the activation of coagulation pathways. 26 Adequate anticoagulation during the operation can effectively prevent the occurrence of coronary thromboembolism. In order to avoid thrombosis, the use of anticoagulants during PCI has become a consensus. The current use of anticoagulants includes heparin and bivalirudin. However, the choice of the two is still controversial. 20
The MATRIX-OCT 27 study suggested that compared with heparin, the minimum blood flow area after the surgery in the bivalirudin group was larger, which provided a mechanical basis for the terminal blood flow. In a controlled study in patients with STEMI undergoing PCI after intravenous thrombolysis and using bivalirudin and heparin respectively, 28 there was no statistical difference in the postoperative TIMI blood flow classification of the criminal coronary artery, the incidence of MACE (4.9% vs. 7.8%), and hemorrhage events (7.3% vs. 11.7%), which was consistent with the results of the present study. In the present study, three patients in both groups had TIMI grade 2 blood flow after the operation, while all of them had TIMI grade 0 before the operation with obvious thrombus loads under angiography.
A meta-analysis suggested 29 that in patients with acute myocardial infarction undergoing PCI, therapy of bivalirudin and heparin showed a similar incidence of MACE and cardiovascular mortality, but the use of bivalirudin would increase the risk of in-stent acute thrombosis. It was suggested in that study that stent thrombosis in the bivalirudin group was correlated with the thrombus load, and there was no stent thrombosis in patients with NSTEMI. In the present study, all patients were STEMI, and neither of the two groups had acute stent thrombosis, which might be correlated with the small number of patients in the present study. However, we could not ascertain whether there exists a correlation between stent thrombosis and bivalirudin and whether there exists an impact of poor stent adhesion on the stent thrombosis. Regarding the surgical approach of patients with STEMI, a trial involving 1074 patients was reported to compare the use of bivalirudin in patients with the femoral artery approach (443 patients), and the use of heparin in patients with the radial artery approach (501 patients). The results indicated that there was no significant difference in the incidence of hemorrhage and mortality between the two groups. 30 This was consistent with the results of the present study. In the present study, the statistics suggested that more than 97% of operations were through the radial artery approach, and a total of six patients adopted the femoral artery approach with three patients in each group. There was no difference in the surgical approach between the two groups.
An observational study mainly evaluated the safety of heparin combined with short-term use of tirofiban compared with bivalirudin in PCI treatment. 31 The results indicated that there was no difference in the MACE events between the two groups. While the combination of heparin with tirofiban significantly reduced the incidence of major hemorrhages (0.7% and 4.1%, P = 0.001), the reasons for the decrease in major hemorrhages were not clear. In the present study, patients using tirofiban had been excluded; thus, the clinical application of tirofiban combined with bivalirudin could not be well-evaluated. In future research designs, a group consisting of patients treated with heparin combined with short-term tirofiban and a second group consisting of patients treated with bivalirudin combined with a short-term tirofiban may be added to further evaluate the effect of bivalirudin combined with short-term tirofiban on clinical hemorrhage events.
In a prospective trial in which 123 older patients with high hemorrhage risk were enrolled, 55 cases belonged to the heparin group, and the other 68 belonged to the bivalirudin group. The MACE and hemorrhage rates in the patients within one year were observed. 32 The results indicated that the hemorrhage rate of the two groups was similar, and cerebral hemorrhage and death occurred in one patient in the heparin group. Thus, it suggested that bivalirudin was not inferior to heparin in older patients with a high hemorrhage risk. This was not researched in the present study. The study of patients with high hemorrhage risks, older patients, and patients with chronic coronary occlusive disease will be further evaluated in future trials.
The present study showed that compared with unfractionated heparin combined with ticagrelor used in patients with STEMI, the application of bivalirudin combined with ticagrelor could reduce the occurrence of mild hemorrhage events in patients 30 days after surgery. Bivalirudin might have more advantages, especially for patients with heparin-induced thrombocytopenia and high hemorrhage risk.
The limitations in the present study were as follows: 1. Only the inpatients from the First People's Hospital of Yulin were enrolled in the present study, and the data from patients in other hospitals were not included. It was a non-multicenter study with only 210 patients included, which was not well represented for the population. 2. The present study focused on the MACE and hemorrhage events 30 days after surgery. The duration of observation was short, with few observation indexes. The present study failed to make the argument based on many aspects, and the evidence was insufficient.
In summary, the combination of bivalirudin and ticagrelor in PCI was not inferior to the combination of unfractionated heparin and ticagrelor, which could reduce the occurrence of mild hemorrhage events, and was safe and effective. Bivalirudin could also be used as a first-line anticoagulant for emergency PCI in patients with STEMI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.