
Abstract
Osteoarthritis is a condition in which joint cartilage and bone degenerate progressively over time. Total joint arthroplasty is a definitive treatment. Cortisol is a hormone that is associated with pain and inflammation. This study aims to investigate the cortisol levels in patients undergoing total joint arthroplasty. Plasma samples were collected from 71 total joint arthroplasty (TJA) patients at baseline (pre-surgery), 24 hours post-operation, and 5 days post-operation. Cortisol levels were measured in each sample using a commercially available ELISA kit. All results were compiled as group means ± SD. The plasma cortisol level at baseline were 218.5 ± 12 ng/mL. The 24-hour post-surgical samples showed a marked increase in cortisol levels 240.7 ± 15 ng/mL. The blood samples drawn at the 5th day after surgery showed a downward trend (74 ± 12 ng/mL). At 5 days post-operation, cortisol levels were significantly lower than at baseline or 24 hours post-operation. These results point to the fact that prior to surgery, the patient’s emotional stress contributes to increased serum cortisol levels. The higher level of cortisol persists at 24 hours post-operation due to inflammation from the procedure. This data also suggests that at 5 days post-operation, the inflammatory response from the surgery and emotional stress subside, resulting in a near normalization of the cortisol levels. Cortisol is a hormone that plays a major role in the body’s response to surgery. The relevance between cortisol and different points in the surgical timeline has the potential to prognosticate and improve recovery measures.
Background
Osteoarthritis is a condition in which joint cartilage and its adjacent bone degenerate progressively over time. In the United States, the lifetime risk of suffering from this disease is 40% in men and 47% in women. 1 First line treatments for osteoarthritis include medications, such as acetaminophen and nonsteroidal anti-inflammatory drugs (NSAID), and physical therapy. 2 For patients who are refractory to these treatment options, total joint arthroplasty (TJA) is a common surgical treatment for osteoarthritis of the hip or knee. 2
Surgical treatment induces stress on the body. 3,4 One component of this stress response, tissue inflammation, is a demonstrated perioperative and postoperative response to surgical treatment. 5 Biomarkers including IL-6 and CRP have been studied and found to be elevated during the post-operative period. 6 IL-6, which is released by monocytes and T2-lymphocytes in response to tissue trauma, was shown to peak 6 hours post-operation, while CRP was shown to peak 2 days post-operation. 6,7 These markers are all indicative of the body’s inflammatory response.
Cortisol is a steroid hormone in the class of glucocorticoid hormones—it affects many organs in the human body. 8 It is produced endogenously in the adrenal gland in a circadian manner; it is also produced in response to physical or emotional stress. 9 This response is produced through the hypothalamic-pituitary-adrenal axis (HPA). 9 This axis begins with the release of corticotropin-releasing hormone (CRH) from the hypothalamus, which induces adrenocorticotropic-releasing hormone (ACTH) release from the anterior pituitary gland. ACTH then binds to the melanocortin 2 (MC2) receptor on adrenal gland cells, which induce the release of cortisol. 9
This axis has been shown to be impacted in response to surgery. In patients who underwent neck surgery, the immediate postoperative period reflected elevations in ACTH, cortisol, and epinephrine, a hormone whose action is influenced by cortisol levels. 10 In response to abdominal surgery, neural input from the surgical wound site was found to increase ACTH and cortisol levels. 11 In orthopedic patients, cortisol levels were found to be above those of normal control in post-operative orthopedic patients. 12 In this population, increased cortisol levels post-operatively were negatively associated with patients’ subjective evaluations of their own pain. 12 Another study compared post-operative cortisol levels in patients of different age groups who underwent total joint arthroplasty—the immediate post-operative stress response is tempered in the aged population (>65 years) compared to the middle aged (40-65 years). 13
While many studies have been done on the inflammatory response to orthopedic surgeries, information is limited on the stress response. In particular, while the pre and post-operative periods have been studied independently, the study of multiple time-points within a large sample of patients has seldom been studied. This study aims to investigate the cortisol levels in patients undergoing total joint arthroplasty at multiple time points. In addition, the study aims to synthesize the physiologic, psychological, and hemodynamic role of cortisol in patients undergoing total joint arthroplasty.
Materials and Methods
The current study is a prospective observational study. The study included patients who had undergone total joint arthroplasty under spinal anesthesia. Patients with recent comorbidities such as a 6 month history of acute coronary syndrome, cerebrovascular incident or deep venous thrombosis were excluded from the study. Additionally, a 3-month history of acute inflammatory disease and permanent glucocorticoid therapy were deemed to be exclusion criteria. Finally, chronic liver failure, chronic kidney disease, and active neoplasm excluded patients from the study.
Plasma samples were prospectively collected from 71 total joint arthroplasty (TJA) patients at baseline (pre-surgery), 24 hours post-operation, and 5 days post-operation. All of the patients included in this study were operated under spinal anesthesia with bupivacaine 0.5%. Before the administration of anesthesia, patients received 2 g Cefazolin in 100 mL saline over 15 minutes and 1 g tranexamic acid. Patients were provided prophylactic anticoagulant therapy according to the American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. All patients’ surgeries were performed in the lateral decubital position using the anterolateral approach. Normal controls represented plasma samples from drug free healthy individuals (n = 50). Cortisol levels were measured in each sample using a commercially available ELISA kit.
Statistical Analysis
Data was analyzed using GraphPad Prism Version 8.0 (GraphPad Software, San Diego, CA), and Microsoft Excel. The results were stated as mean ± standard error of the mean. Paired analysis was performed between the TJA patients’ baseline, 24 hour, and 5 day post-operation samples. The Kruskal-Wallis one-way ANOVA was used to determine statistical significance. P values <0.05 were considered statistically significant.
Results
The plasma cortisol level in normal individuals were 318 ± 11 ng/mL. In contrast, the pre-surgical and 24-hour post-surgical samples showed a marked increase in cortisol levels (> 200ng/mL). The blood samples drawn at the 5th day after surgery showed a downward trend reaching near normal levels (74 ± 12 ng/mL) (Figure 1). There was no significant difference between cortisol levels pre-operatively and within 24 hours of the operation, however the was a significant difference in comparison to the levels on the 5th day and normal.
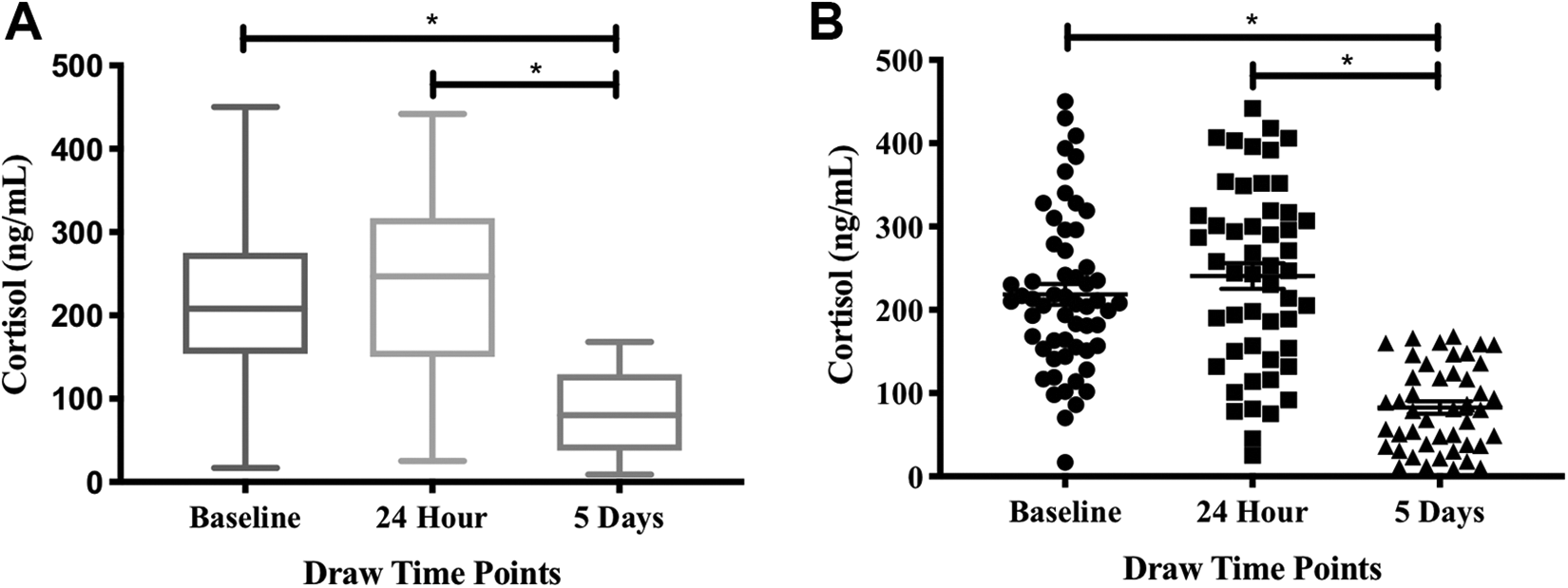
Comparison of cortisol levels within TJA patients at various time points demonstrated by box (A) and scatter (B) plots with mean ± SD. ∗p < 0.05. SD, standard deviation.
As shown in Figure 2, there was no significant difference between cortisol levels pre-operatively and within 24 hours of the operation, however the was a significant difference in comparison to both the pre-operative and 24 hour levels on the 5th day and normal.

Percent change of cortisol levels in TJA patients calculated from 5-day post-operative levels for each individual patient demonstrated by bar (A) and scatter (B) plots.
At 24 hours, the mean cortisol level for the TJA patients was 240.7 ng/mL, and the median was 247 ng/mL. The range was 417 ng/mL. The cortisol level at 24 hours was not significantly different from NHP or TJA patients’ baseline plasma. At 5 days post-operation, the mean cortisol level for the TJA patients was 82.67 ng/mL. The median was 80 ng/mL, and the range was 159 ng/mL (Table 1). This result was significantly different from NHP, TJA patients’ baseline, and TJA patients’ 24 hours (p < 00001).
Cortisol Levels in Total Joint Arthroplasty Patients.

All results represent a mean ± 1 SD of the total cohort for each group.
Discussion
The current study aims to clarify previous studies regarding the stress response to surgery, using cortisol as a biomarker. Previous studies have shown that cortisol levels are increased in surgical patients post-operatively relative to their own baseline levels. 13 In addition, studies have shown post-operative cortisol levels in surgical patients to be increased relative to those of the healthy age-matched population. 12
In the current study, patients’ baseline cortisol levels were elevated relative to that of the normal population. This may be related to the pain responses sustained by osteoarthritis patients requiring surgical interventions. A previous report has described the higher cortisol level in relation to post-operative pain in spine surgery patients. 14 It would have been of interest to measure the cortisol levels after surgical intervention in these patients to demonstrate direct relevance of cortisol levels with pain sustained by these patients. This finding reflects that prior to surgery, a stress related response may already have started in surgical patients. Given that hemodynamic stress has yet to be inflicted on these patients, there are 2 likely explanations for the pre-operative elevation of cortisol.
Firstly, the psychological stress of the pre-surgical timeframe is sufficient to cause an elevation of serum cortisol level in the patient. This idea is supported by previous studies that have examined the effects of pre-operative cortisol levels on surgical, recovery, and functional outcomes.
From the standpoint of successful surgical completion, there is limited literature on the role of pre-operative cortisol on the success of the surgery. Little research exists on whether pre-operative plasma cortisol levels impact surgical success rates, complication risks, or immediate post-surgical recovery. In the context of cardiac surgery, early post-operative cortisol levels have been shown to negatively impact immediate post-operative surgical recovery. With regard to the psychological aspect of operative care, serum cortisol levels have been studied as a marker of pre-operative stress and has been studied in regards to risk for post-operative delirium. 15
Previous studies on cortisol measurement in TJA patients have provided discordant results in specified settings. 15,16 Consistent with our findings, previous studies have demonstrated that elevated pre-operative cortisol levels correlated with functional markers such as cognitive capacity. 15 Similar patterns exist between pre-operative levels of other inflammatory markers, such as IL-6 and CRP, and functional outcomes, suggesting that these biomarkers may significantly impact the recovery process. 6,7 In our studies, we have measured cortisol levels over a period of 5 days in a heterogeneous population without taking into account any age or gender considerations. The reported differences between our studies and other reported results may be due to population differences and methodological consideration. Such considerations may be helpful in a larger cohort to demonstrate variations in cortisol levels. It is likely that if the same collective analysis approach is used to analyze the other studies, the reported results may be similar to those reported in this manuscript. Similarly, our data can be further analyzed and stratified on age-based groups. However, such a study will be more reliable with a higher number of patients. Regardless of the reported differences in cortisol level in TJA patients, our results clearly point out that pathophysiologic and a stress factor result in increased level of this biomarker, warranting additional investigations.
The second explanation for the elevated pre-operative cortisol levels in the current study is that the tissue inflammation from long-standing disease has resulted in a baseline plasma cortisol elevation in these patients. A recent report has also shown that cortisol reactivity seems to be associated with pain development. 14 The increased level of cortisol may therefore be considered as biomarkers of both the inflammatory and pain responses. The associations between pain and inflammation is difficult to differentiate and will require additional studies to score the pain responses along with the level of inflammation. In the current study, we did not differentiate between these 2 factors and additional studies are needed to address these. This idea is supported by literature that has shown elevated cortisol in chronic pain patients, particularly of musculoskeletal origin. 17
At 24 hours post-operation, the patients in the current study did not significantly change relative to the patients’ own baseline values. In the current study, the results validate some of the earlier observations where circulating cortisol levels were elevated in various groups of patients. However, it is interesting to note that 5 days after surgery, the median level of cortisol levels were markedly decreased and reached near normal levels. A limitation of the current study is the lack of an age-matched control group population cortisol level comparison to delineate the effect of aging on cortisol levels. Despite this limitation, the data presented clearly suggests that pain, level of anxiety, inflammation, and other comorbid factors contribute to the enhanced cortisol levels observed in the patients undergoing total joint arthroplasty. The cortisol levels in these patients were elevated relative to those of normal controls who had not underwent surgery. This data differs from that of other studies, who have shown that cortisol levels in the immediate post-operative period are elevated relative to the pre-operative timeframe. 12
At 5 days post-operation, cortisol levels were significantly lower than at baseline or 24 hours post-operation. This finding also differs from previously reported findings in the literature, which noted increased levels post-operatively relative to at baseline.
Cortisol is a hormone that plays a major role in the body’s response to inflammatory stimuli, and therefore recovery from surgery. The relevance between cortisol and different points in the surgical timeline has the potential to prognosticate and improve recovery measures.
One of the limitations of this study is the lack of long-term cortisol values after 5 days. Had values been collected longer into the recovery, cortisol’s role in the post-surgical process could have been further analyzed. Additionally, more data points in the immediate post-operative period would have been useful in trending the cortisol levels between the 24 hour and 5 day point in the post-operative period. Nevertheless, our study clearly shows the increased cortisol level in the baseline and 24 hour post-surgical plasma samples, which are markedly reduced on the 5th day.
Conclusion
Our studies suggest that cortisol levels in patients undergoing TJA are markedly upregulated prior to surgery and slightly increased 24 hours after surgery. There is a dramatic decrease 5 days after surgery in circulating cortisol levels. The data is highly suggestive that inflammatory responses associated with osteoarthritis and other factors result in enhanced cortisol levels in this patient group. While the relevance of such responses as pain and anxiety have not been clearly established, inflammatory responses are reportedly resulting in increase in circulating cortisol levels. Thus, more cortisol levels in pre and immediate post-surgical levels may provide a cumulative index of the pathogenesis which may provide guidance to the management of patients undergoing total joint replacement. The surgical intervention and other measures for the post-operative management of these patients including bed rest and decreased anxiety contribute to the downward trend resulting in near normalization of the biomarkers of inflammation and stress. The observed decrease in the plasma cortisol level in our cohort may reflect the combined pharmacological process to control the pain and post-surgical inflammatory processes.
Footnotes
Acknowledgments
The authors gratefully acknowledge the assistance of the staff of the Department of Orthopaedic Surgery and Rehabilitation, the Department of Pathology, the assistance of the staff of the Hemostasis Research Laboratories for their assistance in the collection and processing of the patients’ plasma samples used in this study. We are also thankful to Dr. Alexander Ghanayem and Dr. Adam Schiff of the Department of Orthopaedic Surgery and Rehabilitation of Loyola for their guidance and support for this work.
Authors’ Note
Ethical approval to collect residual blood samples from the clinical laboratories was granted by the Institutional Review Board of the Loyola University Medical Center (IRB# 9192 0510980).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.