
Abstract
Objective
To investigate the dynamic variation of D-dimer and to evaluate the efficacy and accuracy of D-dimer level in patients with thoracolumbar fractures caused by high-energy injuries.
Methods
A total of 121 patients with thoracolumbar fractures caused by high-energy injuries were retrospectively identified and included in this study. There were 83 males and 38 females, with an average age of 48.6 ± 11.2 years. All patients were treated with either screw fixation surgery or decompression fixation surgery. The D-dimer levels were measured 1 day before surgery and on the first, third, and fifth days after surgery. The dynamic variation of D-dimer and the effects of risk factors on D-dimer levels were analysed. A receiver operating characteristic (ROC) curve analysis was performed and the appropriate D-dimer cut-off level was determined for deep vein thrombosis (DVT) screening.
Results
Due to a trough on the third day, D-dimer levels grew in an unsustainable manner following surgery (P < 0.001). Patients with the operation time >120 min (P = 0.009) and those with an American Spinal Injury Association (ASIA) score A-C (P < 0.001) had higher D-dimer levels. The area under the curve of D-dimer was the greatest on the third day. Applying stratified cut-off values did not change the sensitivity, specificity and negative predictive value in the group with an operation time >120 min, and ASIA score A-C group.
Conclusions
D-dimer levels elevated with fluctuation in patients with thoracolumbar fractures caused by high-energy injuries after surgery. Both operation time and ASIA score had an impact on D-dimer levels. Regarding DVT diagnoses, the diagnostic value of D-dimer was highest on the third day postoperatively, and stratified cut-off values by these two factors did not show better diagnostic efficacy compared with a collective one.
Introduction
Deep vein thrombosis (DVT) is a common and serious complication in trauma patients, especially in patients with musculoskeletal trauma. 1 Previous studies have shown that the incidence of DVT after trauma was reported to be between 9.1% to 11.1%, and in serious cases, it may cause pulmonary embolism (PE) after trauma.2–5 DVT should be prevented and treated in time, otherwise, it can increase the extension of hospitalization time, and its associated costs, affecting the recovery process of patients. In recent years, orthopedists have focused more on DVT identification, prevention, and therapy.
Because of their anatomical position and load, thoracolumbar fractures are the most common spine injuries.6,7 Thoracolumbar fractures are the most common fractures of the spine, which are usually cured using surgical treatment.7–9 For patients with thoracolumbar fractures caused by high-energy injuries, vascular injuries can occur as a result of high external energy events such as falls, traffic accidents, or industrial traumas. Furthermore, immobility paired with prolonged bed rest slows venous return, making patients vulnerable to DVT.10,11 In our hospital, the Caprini score is used to assess the risk of thrombosis. For patients with a high risk of thrombosis, low-molecular-weight heparin (LMWH) is used for thrombosis prophylaxis, and their D-dimer levels are tested regularly during hospitalization. Measurement of D-dimer levels seems to be a useful diagnostic value in cases of suspected DVT, as it is a product of fibrin degradation. 12
D-dimer levels that are elevated usually indicate a boost in the coagulation and fibrinolysis systems, and can be utilized as a sensitive diagnostic of hypercoagulability.13,14 Currently, D-dimer assessment is a tool with practical value in the diagnosis of DVT and PE.12,14,15 In practice, however, for the diagnosis of venous thromboembolism (VTE), D-dimer has a high sensitivity but a low specificity. This is because increased D-dimer levels are non-specific and could be affected by tumors, surgery, and trauma. 16 Efforts should be made to improve the diagnostic efficiency of D-dimer.
Many predictive models use D-dimer as a necessary indicator to predict the incidence of DVT and classify patients according to different levels of risk.17,18 However, most models use preoperative D-dimer test results as a stationary indicator, so the dynamic trend of postoperative D-dimer concentration might be missed, leading to unwanted bias in the use of these models. D-dimer levels should fluctuate when patients with thoracolumbar fractures caused by high-energy injuries have anticoagulant medication and surgery, because D-dimer levels might be influenced by surgery and trauma. Combined with clinical risk factors, the link between D-dimer dynamic alterations and postoperative DVT can assist surgeons better manage patients in a hierarchical manner and identify the high-risk groups for postoperative thromboembolism events.
As there are few studies on the dynamic changes of D-dimer in patients with thoracolumbar fractures caused by high-energy injuries. Our study was to investigate the dynamic variation of D-dimer and evaluate the relationship between D-dimer and DVT within certain groups of patients.
Patients and Methods
Study Population
This study reviewed a total of 121 patients diagnosed with thoracolumbar fractures caused by high-energy injuries from September 2019 to June 2021, admitted to Baoding No. 1 Central Hospital. We defined high-energy injury as an injury caused by high-fall injuries (>2 m), traffic accidents or industrial accidents. The criteria for inclusion were patients older than 18 years, with fresh thoracolumbar fractures caused by high-energy injuries that require surgical treatment, and with complete medical records. The exclusion criteria were patients with old thoracolumbar fractures (> 3 weeks), combined with other fractures, with anticoagulation that occurred before injury, osteoporotic fractures, a history of previous VTE, or patients requiring conservative treatment, The ethics committee of our hospital approved this study.
Electronic medical records provided the clinical data and D-dimer levels needed for the analysis, including age, gender, body mass index (BMI), operation time, blood loss, surgical procedure, American Spinal Injury Association (ASIA) score and DVT event. ASIA scores more accurately represented the disability and mobility. 19 Therefore, we used ASIA scores to quantify neurological deficits. The scale was as follows: (A) no sensory or motor function is preserved, (B) incomplete sensory but no motor function; (C) incomplete motor function is preserved below the neurological level and more than half of the key muscles below the neurological level have a muscle grade less than 3; (D) incomplete motor function is preserved below the neurological level, and at least half of the key muscles below the neurological level have a muscle grade greater than or equal to 3; and (E) sensory and motor function are normal.
After admission, all of the patients were given a Caprini thrombosis risk assessment. According to the Caprini risk model, all of the patients were in the highest risk group, and all of the patients received both mechanical and chemical prophylaxis. Mechanical prophylaxis included intermittent pneumatic compression and ankle pump training. All patients received a prophylactic anticoagulant, with administration of low molecular weight heparin (LMWH) 4100 U (Changshan Production, Hebei, China) once a day, from the day of admission until discharge. A duplex ultrasound of the veins in the lower extremity was executed to detect DVT in all patients. All patients routinely underwent duplex ultrasound approximately one day before surgery and one week postoperatively. All examinations were conducted with the same ultrasound equipment (Philips Medical Healthcare, Armstrong, Netherlands) by the qualified examiners. Direct thrombus detection by incomplete compressibility of the vessel, observation of lack of blood flow, or both were used to diagnose DVT. To ensure that any asymptomatic thromboembolism was not missed, all patients were examined on both sides of their lower limbs.
D-dimer levels were assayed using photometric immunoassay (Sysmex Chemical Medicine, Kobe, Japan) within two hours after collection from veins in the forearm. D-dimer levels were measured 1 day before surgery and on the first, third, and fifth days postoperatively.
Statistical Analysis
Statistical analysis was performed with the SPSS software (Version 26.0, IBM SPSS Inc., Chicago, IL, USA). The baseline characteristics were expressed as mean ± standard derivation (SD), ratio or median with interquartile range (IQR) accordingly. To detect the time effects on perioperative D-dimer levels, a repeated measures ANOVA was used. A post hoc test was used to analyse discrepancy of dynamics between different subgroups and differences ascribed to operation time, ASIA score and DVT within each point of time, where the P-value was adjusted by the Bonferroni method. A receiver-operating characteristic (ROC) curve was conducted to evaluate D-dimer level discrimination between DVT patients and non-DVT patients. The optimum cutoff value was approached by the Youden index. We also calculated sensitivity, specificity, and negative predictive value (NPV) using optimum cut-off values, and then compared discrepancy between groups using a chi-square test or Fisher's exact test. Values for P < 0.05 were defined as statistically significant.
Results
Patient Characteristics
A total of 121 patients were retrospectively analysed in our study, 67% of which were men. The average age of the patients was 48.6. The average BMI was 23.4 ± 2.9. The incidence of postoperative DVT was 20.7% (25/121). The average operation time was 120 min, and the average blood loss was 319.8 mL. All patients received surgical therapy. Fixation surgery was performed in a total of 101 (83.5%) patients, whereas 20 (16.5%) patients underwent fixation with decompression. In terms of ASIA scores, 100 (81.8%) of the patients were ASIA score D-E and the others (n = 21, 18.2%) were ASIA score A-C (Table 1).
Clinical characteristics and D-dimer levels of the study patients (n = 121).

BMI, body mass index; DVT, deep vein thrombosis; ASIA, American Spinal Injury Association
Perioperative D-Dimer Variation According to Clinical Factors
D-dimer levels increased significantly after surgery in general (P < 0.001) but did not continue to increase, as it declined slightly on the third day, although it was still higher than that before surgery(P < 0.001). On the fifth day after surgery, the D-dimer level peaked (Figure 1A). When it came to comparison between groups (Table 2), D-dimer levels were significantly higher in the group with an operation time >120 min (n = 60) than the group with an operation time ≤120 min (n = 61) (P = 0.009), and group with an ASIA score A-C (n = 21) had higher levels than ASIA score D-E (n = 100) (P < 0.001). The DVT group (n = 25) had higher D-dimer levels than those in the non-DVT group (n = 96) (P <0.001). There were no significant differences attributed to other clinical factors. Interestingly, by different grouping, D-dimer levels in the respective subgroups tended to be the same as those in the whole study population (Figure 1B and C). As for operation time grouping, there was a significant increase of D-dimer levels in operation >120 min group after surgery (all P < 0.001), while no significant difference was seen on preoperative D-dimer levels. At each timepoint, patients with ASIA score A-C had a much higher D-dimer concentration compared with ASIA score D-E (Table 3).

(A) perioperative D-dimer concentration (mg/L) of whole study population; (B) patients divided into different subgroups: →,operation>120; –•, operation≤120; ♦ ,all; (C), →, ASIA A-C; –•, ASIA D-E; ♦ ,all; (D) ,DVT; –•, non-DVT; –• ,all.
Comparisons of D-dimer levels(all time points) by different groups.

BMI, body mass index; DVT, deep vein thrombosis; ASIA, American Spinal Injury Association
The differences of D-dimer levels(mg/L) at four points of time according to different subgroups.

D-Dimer Changes According to DVT Outcomes
After surgery, D-dimer levels were significantly higher in 25 patients (20.7%) diagnosed with DVT than in non-DVT patients (P < 0.001). These two subgroups had the same D-dimer levels as the whole population. However, because no difference was found between preoperative time and the third day after surgery in the non-DVT group (P = 0.071, Table 4), D-dimer levels fluctuated more steadily (Figure 1D).
Changes of D-dimer between different time points in the DVT group and Non-DVT group.

ROC Analysis on Relationship Between D-Dimer and DVT
When the entire population was considered, the area under the curve (AUC) on the third day after surgery was greatest, which was 0.844 (P < 0.001, 95% CI: .767–.904), and the cutoff value of D-dimer was 2.56 mg/L (sensitivity = 84.00%, specificity = 76.04%). The AUC was then calculated in separate subgroups based on operation time and ASIA score. The AUC was higher in the operation time of >120 min group (AUC = 0.861 [P < 0.001, 95% CI: .748–.937]) than in the operation time of ≤120 min group (AUC = .636 [P = 0.156, 95% CI: .502–.755]), with significant difference (Z = −2.381, P = .017). The AUC for ASIA score A-C group was .683 (P = .144, 95% CI: .453–.862) and .838 (P < .001, 95% CI: .751–.904) for ASIA score D-E group, and there was no significant difference between the two groups (Z = −1.167, P = .243). The cut-off value for the operation ≤120 min group, operation >120 min group, ASIA score A-C group and ASIA score D-E group were 2.13 mg/L, 2.50 mg/L, 2.56 mg/L,2.50 mg/L, respectively. The differences in sensitivity, specificity and negative predictive value (NPV) between subgroups were not significant when the respective cut-off values were used, as well as when comparisons between subgroups were made using the fixed cut-off value from the whole population (Table 5).
Accuracy of D-dimer for DVT resulting from different cutoff values.
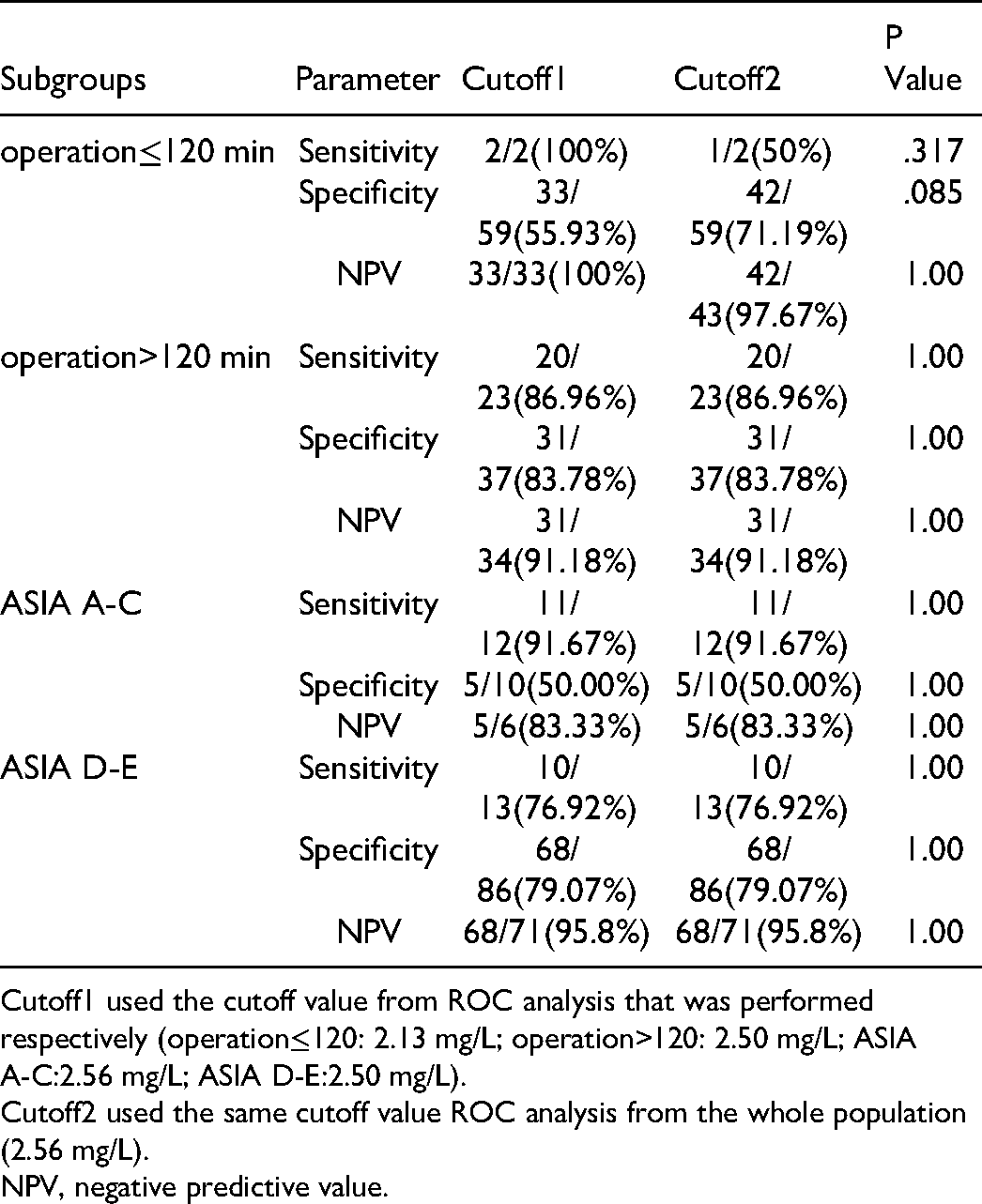
Cutoff1 used the cutoff value from ROC analysis that was performed respectively (operation≤120: 2.13 mg/L; operation>120: 2.50 mg/L; ASIA A-C:2.56 mg/L; ASIA D-E:2.50 mg/L).
Cutoff2 used the same cutoff value ROC analysis from the whole population (2.56 mg/L).
NPV, negative predictive value.
Discussion
Many studies have demonstrated that traumatic patients have a significantly increased risk of DVT.1,2,20,21 Venous thromboembolic disease is the major cause of morbidity and mortality in patients undergoing traumatic orthopedic surgery.21,22 Therefore, early detection and diagnosis of DVT is very important clinically. In the present study, we wanted to see if D-dimer levels varied early after surgery in patients with thoracolumbar fractures caused by high-energy injuries, and if D-dimer might be utilized to diagnose DVT. We also looked at the effects of various factors on D-dimer dynamics and whether there was a difference in diagnostic efficacy between subgroups as a result of these factors.
To identify those at high risk of developing DVT, an effective and non-invasive surveillance of coagulation indicators is essential. Although D-dimer is affected by many factors, it is still considered as a most powerful indicator of venous thromboembolic events.23,24 Owings et al. 25 sampled the plasma of severely injured patients for D-dimer assay at hours 8, 16, 24, and 48; and at days 3, 4, 5, and 6. they found before 48 h after injury, the vast majority of patients without thromboembolism had positive D-dimer assays, and D-dimer levels might be very low within 48 h of injury. Our previous study found that in patients with thoracolumbar fractures caused by high-energy injuries, D-dimer at admission was a risk factor for DVT, but the AUC value was not very high. 26 So in the present study, we measured the D-dimer level at 1 day before surgery and on the first, third, and fifth days postoperatively to detect the early changes of D-dimer levels.
During the first five days after surgery, we found a non-linear increase in D-dimer levels in the current study. There was a trough on the third day after surgery. Bytniewski et al. 27 investigated the dynamics of D-dimer level after the cemented and cementless total hip and total knee replacement, and found a similar tendency, which was consistent with our research. The reasons for the elevation of D-dimer after surgery may be due to surgical trauma, anaesthesia interference, intraoperative blood loss and blood transfusion, the activation of coagulation system by implants, and the participation of various inflammatory mediators in the body to promote coagulation under stress. The decrease of D-dimer level on the third day is probably because of the increase of active and passive activities after surgery, the intervention of mechanical and chemical prophylaxis, the secondary fibrinolytic activities of the body, and the degradation of fibrin in the process of tissue repair.
In our study, two major clinical factors affecting postoperative D-dimer level, namely operation time and the ASIA score, were identified. A previous study found that, in neurosurgical patients, prolonged operation time was identified as an independent predictor for postoperative DVT. 28 As for patients undergoing spinal surgery, a meta-analysis which included 46,891 patients reported that long surgical times increased the incidence of VTE. 29 Our study showed that the levels of D-dimer on the first, third, and fifth days postoperative were significantly higher in patients with operation time >120 min. However, no significant difference was observed on 1 day before surgery. We thought that the extended operation time could lead to more intraoperative blood loss and longer stasis in lower extremity veins. As a result, patients with long operation time tended to be in a more procoagulant state and had higher D-dimer levels. Patients in this study received ASIA Impairment Scale examination at admission which was a standardized neurological examination assessing the severity of motor and sensory levels for spinal cord injury. According to ASIA score, we divided the patients into grade A-C and grade D-E in our study. We found patients with ASIA score A-C had higher levels of D-dimer than those with ASIA score D-E. This phenomenon not only appeared at all postoperative time points, but also the preoperative comparison was significant. Ma et al. 30 demonstrated in a study from their institution with 2432 patients with spinal fracture that patients with ASIA A and B had a 2.36-fold increased risk for the occurrence of DVT, which was in concordance with the findings by our previous study. 26 The loss of the motor function can weaken muscle pumps which may cause hypercoagulability and venous stasis. Therefore, patients with ASIA score A-C have venous stasis and higher D-dimer levels.
Doctors have a hard time identifying high-risk patients based on a variety of risk factors. When employing D-dimer, many studies have taken various measures to improve the diagnostic value of D-dimer.23,31,32 Ke et al. used a respective cut-off value of D-dimer in subgroups and elevated the diagnostic ability of D-dimer in lung cancer patients after surgery. 23 In the present study, we performed a separate ROC analysis in order to determine the cut-off value in subgroups. But we showed the cut-off values were so close that the sensitivity, specificity and NPV does not change compared to the whole population. This phenomenon indicated that the cut-off value of D-dimer was stable in these patients.
Our study has several limitations. First, the small sample size and retrospective study nature had inherent limitations. Second, the number of subgroups was not equal, which can lead to bias. Third, we only measured the D-dimer levels at three time points during the five days after surgery, which reflected the early variation of the D-dimer levels. So large population size and multiple time points measurement of D-dimer after surgery were needed to detect the dynamic variation of D-dimer.
Conclusions
D-dimer levels elevated with fluctuation in such patients after surgery. Operation time and ASIA score had an impact on D-dimer levels. Regarding DVT diagnosis, the diagnostic value of D-dimer was highest on the third day postoperatively and stratified cut-off values by these two factors didn't show better diagnostic efficacy compared with a collective one.
Footnotes
Author Contributions
.
Ethics Approval
The Ethics Committee of Baoding No.1 Central Hospital approved this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Baoding Science and Technology Bureau project (grant number 2041ZF100).