
Abstract
Objective
To explore the correlation between the fracture line inferior plane and perioperative deep venous thrombosis (DVT) in patients with tibial fractures.
Methods
Data was collected from the medical records of 536 consecutive patients with tibial fractures at Xi’an Honghui Hospital. The patients were divided into distal, shaft, and proximal segment groups according to the fracture line inferior plane on radiographs. Multivariate logistic regression models were used to identify the role of the inferior plane of the fracture line in perioperative DVT.
Results
A total of 431 patients were included in the study and 226 patients had perioperative DVT in the lower extremities, including 11 proximal and 215 distal DVTs. Univariate regression analysis showed a significant correlation between the proximal segment and perioperative DVT; however, no correlation was found in the shaft segment group. Additionally, age, coronary heart disease, associated injuries, and time to operation ≥6 days were risk factors for perioperative DVT. However, fixation with intramedullary nails may be a protective factor for perioperative DVT compared with plates. After adjusting for potential confounding factors, the proximal segment group had an increased incidence of perioperative DVT compared to the distal segment group.
Conclusions
The proximal segment may be correlated with an increased incidence of perioperative DVT by 7.30-fold in patients with tibial fractures compared to that in the distal segment. In clinical practice, surgeons should be vigilant for DVT formation in these patients.
Introduction
Deep venous thrombosis (DVT) is a common complication of lower-extremity fractures. The incidence of DVT varies across locations. The incidence of perioperative DVT in patients with tibial fractures is 4.7 to 16.3% in the tibial plateau,1,2 13.3% in the shaft, 3 and 1.7% in the distal tibia. 4 The incidence of DVT in the proximal segment was higher than that in the distal segment.
Tibial fractures often occur in both low- and high-energy trauma, or repetitive impact activities. Injuries caused by high-energy trauma are more likely to involve complex and open tibia fractures and fractures in specific locations, such as the tibial plateau, 5 and injuries caused by low-energy trauma often result in simple transverse or linear tibial fractures. 6 Usually, tibial fractures are divided into proximal 1/3, middle 1/3, and distal 1/3 fractures because these three parts correspond to the characteristics of the tibial anatomy and distribution of the nutrient artery. 7 The nutrient artery generally enters the shaft of the tibia in its upper 1/3; this arrangement deprives nutrition to the lower one-third of the shaft, thus making the lower 1/3 of the tibia more liable to undergo nonunion in the event of a fracture. 7 The tibial anatomy and nutrient artery make the tibial fractures more complicated as various patterns of injury can occur. Some fractures, even with a long fracture line extending to the segment of the tibial shaft, are still called tibial plateau fractures. Some distal roof fractures reach up to the shaft; however, they are called pilon fractures. Thus, the fracture line locations does not correspond to the fracture types.
The end of the fracture line corresponds to the actual injury plane. Various tibial fractures have unequal planes with different fracture lines. In addition, different fracture line planes influence soft injuries in various planes. Below this plane, the distal function would be lost in the injured tibia. The fracture plane in the proximal segment restricts the activity of the knee joint, and the fracture plane in the distal segment obstructs the ankle joint.
Clinically, our focus is on the fracture site and specific classification, not on the span of the fracture line inferior plane. Therefore, this study explored the correlation between the fracture line inferior plane and perioperative DVT in tibial fractures. We hypothesized that the fracture line inferior plane would affect the incidence of DVT, and that the fracture line inferior plane at the proximal segment would increase the probability of DVT.
Materials and methods
Study Population
Clinical and surgical data of the cases reviewed in this study were obtained from the original medical records. The ethics committee of Xi’an Honghui Hospital approved this retrospective study.
A total of 536 consecutive patients with tibial fractures at Xi’an Honghui Hospital between February 2016 and November 2018. The inclusion criteria were as follows: age ≥18 years; fresh and closed tibial fractures receiving surgical treatment; availability of DVT results at admission and postoperatively; availability of plain film x-rays of full-length tibia; and x-rays or computed tomography scans that could clearly show the fracture line inferior plane. We excluded patients with open fractures and a history of thrombosis.
According to the fracture line inferior plane on x-rays, two senior surgeons (Zhan Wang and Han-zhong Xue) divided the patients into three groups: distal segment, shaft, and proximal segment. On the radiographs, we divided the entire tibia into three sections using two horizontal lines: 1) the fracture line or the most distal end of the fracture line at the superior 1/3 of the tibia was the proximal group; 2) the fracture line or the most distal end of the fracture line in the range of the middle 1/3 of the tibia was the shaft group; and 3) the fracture line or the most distal end of the fracture line at the inferior 1/3 of the tibia was the distal group.
Perioperative DVT was defined as thrombosis occurring before or after the operation. Ultrasonography was used to diagnose DVT. Venous ultrasonography was performed by three trained operators using a bedside machine. The diagnostic criterion for fresh thrombosis was the presence of a constant intraluminal filling defect. 8 All patients underwent initial examination of both lower extremities at admission.
We collected the baseline information of the patients, including age, sex, fracture line inferior plane on x-rays, comorbidity (hypertension, diabetes, coronary heart disease, and associated injuries), length of hospital stay, time to operation, blood transfusion, fixation type (plate, intramedullary nail, cannulated screw), blood loss, and liquid infusion. Comorbidities were diagnosed upon admission. Patients with associated injuries were defined as having other injuries and receiving conservative treatment. The time to operation was defined as the duration from the injury to the completion of the procedure. Blood transfusion and liquid infusion were defined as the number of intraoperative transfusions given.
During hospitalization, the surgeons assessed the thromboembolism risk for patients using the Risk Assessment Profile for Thromboembolism score. 9 For patients without contraindications, low-molecular-weight heparin (LMWH) was subcutaneously injected to prevent DVT, according to guidelines. 10 Anticoagulant therapy was discontinued 12 h preoperatively and resumed 24 h postoperatively. In addition, we used a mechanical pressure pump (20 min, twice per day) to prevent DVT. For patients without thrombosis, a prophylactic dose of LMWH was continuously injected subcutaneously. For patients with thrombosis, surgeons from the vascular surgery department prescribed DVT treatment, and the treatment dose of LMWH was subcutaneously injected. If needed, an inferior vena cava filter was used to prevent fatal pulmonary embolism before the operation. After the operation, anticoagulant therapy was continued. The patients underwent a second ultrasonography examination in both lower extremities between the second and fourth day after the operation.
Statistics Analysis
First, we compared the data distribution of each covariate among the three groups. Second, univariate and subgroup analyses were used to examine whether fracture line inferior plane and other covariates had an independent effect on the perioperative occurrence of lower-extremity DVT following tibial fractures. Third, we explored the relationship between the fracture line inferior plane and perioperative DVT in patients with tibial fractures using multivariate logistic regression models with adjustment for potential confounders. All analyses were performed using R (http://www.R-project.org) and EmpowerStats software (www.empowerstats.com, X&Y Solutions, Inc. Boston MA).
Results
Patient Characteristics
Among the 431 patients included in this study, there were 60, 159, and 212 patients in the distal, shaft, and proximal groups, respectively. The demographic and clinical characteristics of the patients are shown in Table 1. The shaft group had a lower percentage of associated injuries (15.72%, P = 0.021) than the distal (25.00%) and proximal (27.83%) groups. The distal and proximal groups tended to receive plates, and the shaft group was prone to use intramedullary nails (P < 0.001). The duration of the operation and distribution of infusion in the three groups were significantly different (P < 0.001). Apart from these factors, there were no noticeable differences in the clinical characteristics among the three groups.
The demographic and clinical characteristics.

Univariate and Multivariate Analysis
Two hundred and twenty-six patients (52.44%) had perioperative DVT in the lower extremities. There were 11 proximal DVTs (4.87%) and 215 distal DVTs (95.13%). No pulmonary embolism was observed. Univariate regression analysis showed that the proximal segment was significantly correlated with perioperative DVT (odds ratio [OR] = 5.95, 95% confidence interval [CI]: 3.13-11.30, P < 0.001); however, no correlation was found in the shaft segment group (OR = 1.90, 95% CI: 0.99-3.66, P = 0.054). In addition, age (OR = 1.05, 95% CI: 1.04-1.07, P < 0.001), coronary heart disease (OR = 2.52, 95% CI: 1.09-5.83, P = 0.030), associated injuries (OR = 2.15, 95% CI: 1.34-3.44, P = 0.001), and time to operation ≥ 6 days (OR = 2.66, 95% CI: 1.63-4.34, P < 0.001) were risk factors for perioperative DVT. However, fixation with intramedullary nails (OR = 0.58, 95% CI: 0.38-0.91, P = 0.017) may be a protective factor for perioperative DVT, as shown in Table 2.
The univariate analysis of risk factors on perioperative DVT.

The subgroup analysis of the risk factors contributing to perioperative DVT is shown in Table 3. Among these factors, the results for the different subgroups were comparable, and the results were relatively stable.
Subgroup analysis of potential factors contributing perioperative DVT.

Because age, time to operation, operative time, blood loss, and infusion were continuous variables, the smoothing curve fitting of these factors between perioperative DVT was drawn, as shown in Figure 1. As for the curve relationship to perioperative DVT, only age was considered as the adjustment factor. In addition, we explored the relationship between DVT and the fracture line inferior plane and found that the fixation type was an essential factor. Thus, we identified factors that need to be controlled.

The curve correlation between age (a), time to operation (b), operative time (b), blood loss (c), and infusion (d) and perioperative DVT.
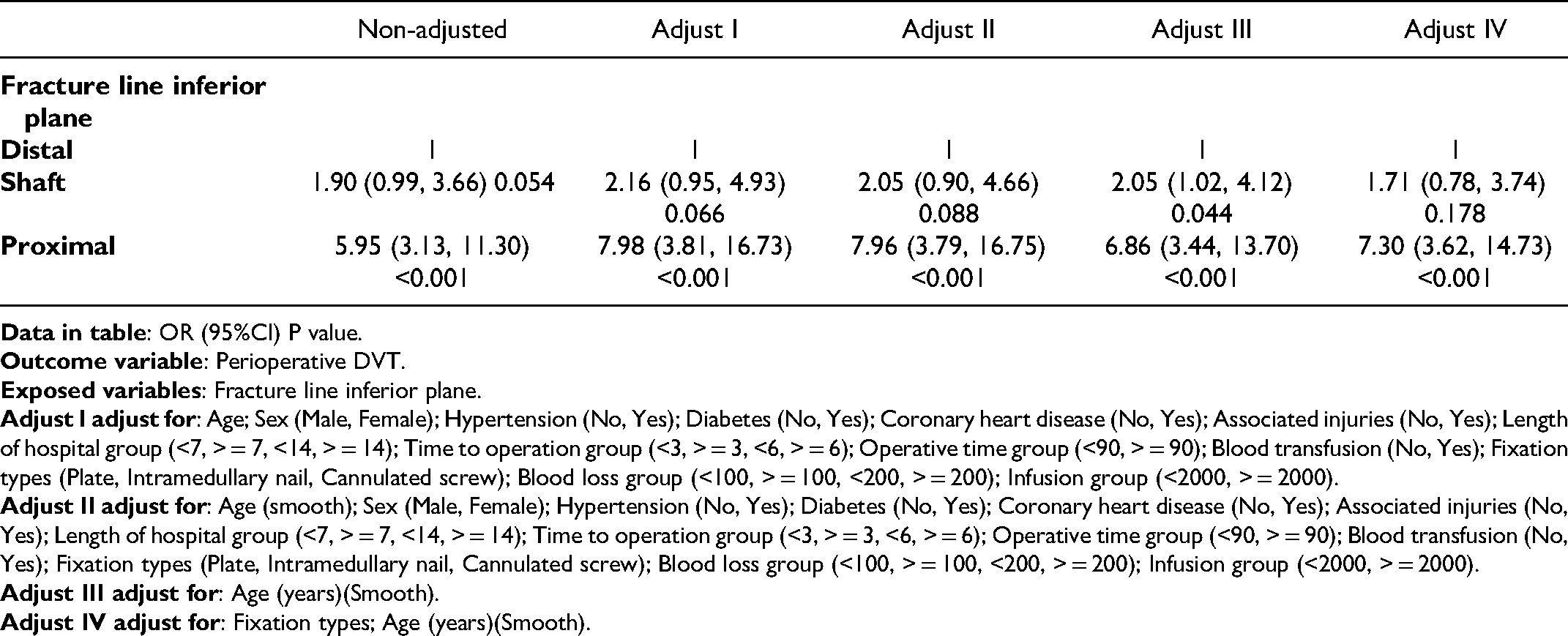
After adjusting for potential confounding factors, the independent effect of the fracture line inferior plane on perioperative DVT was confirmed, as shown in Table 4. Compared to the distal segment group, the proximal segment group had an increased incidence of perioperative DVT (OR = 7.30, 95% CI: 3.62-14.73; P < 0.001). Compared to the distal segment group, the shaft segment group increased the DVT risk; however, the statistics were not unanimous in different models.
Relationship between Fracture line inferior plane and perioperative DVT.
In addition, we continued to complete the sensitivity analysis to explore the stability of the results. When the subgroups were divided into the above-identified factors individually, the results in the different subgroups were very close.
Discussion
Several studies have investigated the risk factors for perioperative DVT after tibial fractures,2,5 such as body mass index, pre-existing diabetes, delay to ultrasonography, platelet count, neutrophil count, older age, hyponatremia, and prolonged surgical time1–3. Surgeons always pay attention to fracture classification and build an association between tibial plateau fracture and DVT,1,2 tibial shaft fracture and DVT, 3 and distal tibial fracture and DVT. 4 However, the end of the fracture line is the actual injury plane, and the effect of the plane on perioperative DVT has not been explored. This study aimed to show the relationship between the fracture line inferior plane and perioperative DVT in patients with tibial fractures. We found that the fracture line inferior plane could influence the occurrence of perioperative DVT in patients with tibial fractures. Compared to the distal segment group, the proximal segment group had an increased DVT incidence, and the shaft segment group showed the same trend but without statistical difference.
This may be due to the following reasons: First, proximal fractures are likely to cause direct damage to the posterior and anterior tibial veins. When the intima of the venous blood vessel is injured, endothelial cells undergo degeneration, necrosis, and shedding. Consequently, collagen fibers under the endothelium are exposed, activating endogenous coagulation. 11 Second, the proximal small arteries or veins were injured, which caused blood extravasation, leading to tissue edema and changes in the osmotic pressure and pressure of the local tissue. Third, the blood loss of tibial fractures was 500 to 1000 ml. 12 Due to greater blood loss in tibial plateau fractures, proximal fractures lead to high blood viscosity and slow blood flow. Fourth, surgeons chose long braces for proximal fractures. After fixation, the muscles of the lower limbs were in a relaxed state, which greatly affected the activities of the lower limbs. The above possible causes are consistent with the three elements of thrombosis, which explains our conclusion to a certain extent.
In the process of identifying patients, we included fresh closed tibial fractures that received surgical treatment, avoiding the confounding factors associated with open fractures and conservative treatment. In addition, we identified two crucial confounding factors: age and fixation type. Age is closely related to perioperative DVT, which has been proven in many tibial studies2,3 and other lower extremity sites.13,14 The age range in this study varied from 18 to 88 years. The average age was 47.33 years. Thus, referring to the survey by Li et al. 2 and the distribution of age in this study, we divided the participants into three age groups: age <40 years, age ≥ 40 and <55 years, and age ≥ 55 years. The overall trend was similar to the final results in the different subgroups (Table 3). The results were similar between the groups. As for the fixation types, the surgeons often preferred plates for tibial plateau fractures and distal tibia fractures.15,16 Intramedullary nails are typically chosen for shaft fractures. 17 In this study, 303, 110, and 18 patients received plates, intramedullary nails, and cannulated screws, respectively. The overall trend was close to the result in different subgroups, and the results were similar among plates, intramedullary nails, and cannulated screw groups (Table 3). Furthermore, tibial fractures are usually associated with other injuries. In our study, 99 patients had associated injuries, including fibula fractures, craniocerebral injuries, thoracic injuries, pelvic fractures, spine injuries, ankle joint injuries, foot ligament injuries, and nerve injuries. All associated injuries were treated conservatively. Thus, the included patients underwent surgery only once. Yu et al. demonstrated that patients with tibial fractures have a higher associated risk of torso, severe head, and severe spine injuries than patients with other fractures. 18 In our analysis, the trends in the subgroups with and without associated injuries were consistent.
In the sensitivity analysis, the results for the different subgroups were similar. Thus, we found that compared to the fracture line inferior plane on the distal segment, the proximal segment may be correlated with an increase in the incidence of DVT by 7.30 folds. However, the shaft segment only exhibited a trend without statistical differences.
In clinical practice, when a patient with a high fracture line inferior plane is admitted, surgeons should be alert and look out for DVT formation in the lower extremities and screen such patients using ultrasonography frequently.
Although our analysis suggested that the fracture line inferior plane on x-rays was correlated with perioperative DVT, this study has several limitations. First, the results are suitable for patients with closed tibia fractures; therefore, patients with open fractures could not adopt this conclusion. Second, although we have presented the relationship between the fracture line plane and perioperative DVT, it does not provide new crucial evidence in the field of DVT. Third, according to previous studies, other risk factors, such as a history of cancer, trauma energy, fracture classification, stroke, and hormonal therapy were important; however, we these were not assessed in this study.
Conclusions
Compared to the fracture line inferior plane on the distal segment, the proximal segment may be correlated with an increased incidence of perioperative DVT by 7.30 folds in patients with tibial fractures. In clinical practice, surgeons should pay more attention to DVT formation in these patients.
Ethics Approval and Consent to Participate
The study was approved by the ethics committee of Xi’an Honghui Hospital.
Consent for Publication
Not applicable
Availability of Data and Material
The datasets generated and/or analyzed during the current study are not publicly available because of data privacy.
Footnotes
Authors’ Contributions
According to the definition given by the International Committee of Medical Journal Editors, the authors listed above qualify for authorship by making one or more of the substantial contributions to the intellectual content of the following:
Kun Zhang and Wei Huang carried out the conception and design. Wang, X. Wang, X. Xue, Z. Li, W. Jiang, Y. Nian, and Y. Zhu performed the analyses Xiao Cai and Wei Huang participated in drafting of the manuscript.
All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the Foundation of Xi’an City (grant number 2019115713YX012SF052, 2019ZDLSF01-09).