
Abstract
Aim
To develop and validate 3 nomograms incorporating the advanced lung cancer inflammation index (ALI) that can aid in predicting the risk of coronary artery disease (CAD) and coronary artery calcification (CAC).
Methods
The study enrolled 562 consecutive patients with suspected CAD who underwent coronary computed tomographic angiography between September 2015 and June 2017. Independent risk factors for CAD, CAC, and CAD with CAC were identified via univariate and multivariate analysis, and nomograms were established based on the independent predictors identified. The area under the curve (AUC), calibration curve, and decision curve analysis were used to evaluate the nomograms. Correlations between ALI and other clinical indicators were examined via Spearman correlation analysis.
Results
In total, 549 patients with suspected CAD who underwent coronary computed tomographic angiography were included. Male sex, hypertension, diabetes, dyslipidemia, ischemic stroke, and ALI were independent predictors of both CAD and CAC. Male sex, hypertension, diabetes, dyslipidemia, and ALI were also identified as independent predictors of CAD with CAC. The AUC values for the nomograms developed using these risk factors were 0.739 (95% confidence interval [CI], 0.693-0.785), 0.728 (95% CI, 0.684-0.772), and 0.717 (95% CI 0.673-0.761), respectively. ALI was negatively correlated with neutrophil-to-lymphocyte ratio and CAC score and positively correlated with serum albumin levels and body mass index (all P < .05).
Conclusions
ALI is an independent predictor of CAD, CAC, and CAD with CAC. Our ALI-based nomograms can provide accurate and individualized risk predictions for patients with suspected CAD.
Keywords
Introduction
Coronary artery disease (CAD) is the leading cause of cardiovascular mortality and morbidity worldwide. 1 Coronary atherosclerosis is a chronic inflammatory disease characterized by atherosclerotic plaque formation due to intimal inflammation and repeated cycles of erosion, fibrosis, healing, and calcification.2,3 Coronary artery calcification (CAC) is a specific marker of CAD and is closely related to the atherosclerotic plaque burden. 4 Given its ability to provide information regarding plaque volume and composition beyond luminal stenosis, non-invasive coronary computed tomographic angiography (CCTA) is widely used for first-line investigation in patients with suspected CAD.5–7 Indeed, research has demonstrated that the CAC score calculated based on CCTA findings is a valuable tool for the stratification of patients with low-to-intermediate risk CAD.2,8 As early detection of CAC has been identified as an important predictor of future CAD risk, 9 a CAC-related model may aid in the early identification of CAD.
Understanding and appropriately quantifying the contributions of key risk factors is critical for formulating and optimizing preventive strategies for CAD. 10 The recently proposed advanced lung cancer inflammation index (ALI; body mass index [BMI] [kg/m2] × serum albumin level [ALB] [g/dL]/neutrophil-to-lymphocyte ratio [NLR]) 11 is a marker of exacerbated systemic inflammation, 12 which has been associated with CAD in previous studies.13,14 Several studies have also reported associations between low ALI and clinical outcomes in patients with a variety of malignancies.11,15–17 However, to our knowledge, no study has assessed the diagnostic utility of the ALI for CAD or CAC.
The nomogram is a widely utilized statistical tool that uses 2 or more biological and clinical variables to calculate the probability of a particular outcome for an individual patient.18,19 In the present study, we aimed to develop and validate ALI-based nomograms for predicting the risk of CAD and CAC. We hypothesized that ALI would be identified as an independent risk factor for both CAD and CAC.
Materials and Methods
Study Population and Ethical Approval
We included 562 inpatients with suspected CAD who underwent CCTA at the Affiliated Hospital of Chengde Medical University between September 2015 and June 2017. The inclusion criteria were as follows: myocardial ischemic symptoms, clinically suspected diagnosis of CAD, agreement to undergo CCTA. CAD was diagnosed based on the presence of ≥50% stenosis in at least one branch of the left main, left anterior descending, left circumflex, or right coronary artery on CCTA. 20 The exclusion criteria were as follows: acute coronary syndrome, connective tissue disease, severe valvular heart disease, hypertrophic cardiomyopathy, and constrictive pericarditis.
The study was approved by the Institutional Review Board of The Affiliated Hospital of Chengde Medical University, and all participants provided written informed consent.
Clinical Data Collection
Data related to demographic and clinical characteristics were collected during hospitalization by postgraduate students. Age, sex, height, weight, routine blood test results, and biochemical test results were recorded. Patients also underwent careful assessment for typical clinical risk factors for CAD, such as diabetes, hypertension, dyslipidemia, and ischemic stroke. Hypertension was defined as systolic blood pressure ≥140 mmHg (1 mmHg = 0.133 kPa) and/or diastolic blood pressure ≥90 mmHg at rest, or a previous diagnosis of hypertension with antihypertensive therapy. 21 Diabetes mellitus was defined as follows, in accordance with American Diabetes Association criteria: (1) glycated hemoglobin value of 6.5% or higher, (2) fasting plasma glucose ≥126 mg/dL (7.0 mmol/L), (3) 2-h plasma glucose ≥200 mg/dL (11.1 mmol/L) during an oral glucose tolerance test using 75 g of glucose, and/or (4) classic symptoms of hyperglycemia (eg, polyuria, polydipsia, and weight loss) or hyperglycemic crisis with random plasma glucose ≥200 mg/dL (11.1 mmol/L). In the absence of unequivocal hyperglycemia, the first 3 criteria were confirmed by repeating the test. 22 Dyslipidemia was defined as a serum total cholesterol level ≥5.18 mmol/L, high-density lipoprotein cholesterol level ≤1.04 mmol/L, low-density lipoprotein cholesterol level ≥3.37 mmol/L, triglyceride level ≥1.7 mmol/L, or a previous diagnosis of dyslipidemia with prescribed medication. 23 Ischemic stroke was diagnosed by 2 experienced clinical neurologists from the Department of Neurology based on the recommendations of the World Health Organization. Diagnoses were confirmed by evaluating clinical symptoms, neurological examination results, and computed tomography and/or magnetic resonance imaging findings. 24 ALI was calculated using the following formula: ALI = BMI (kg/m2) × ALB (g/dL)/NLR. 11
Calculation of CAC Score
CCTA was performed using a 320-detector row computed tomography scanner (Aquilion ONE; Toshiba Medical Systems). Calcium was identified based on the presence of at least 3 contiguous imaging pixels >1 mm2 with a density >130 Hounsfield units (HU). The CAC score was calculated as the sum of the calcium scores of the 4 main coronary arteries (left main, left anterior descending, left circumflex, and right coronary) according to the Agatston scoring algorithm. 25 A weighting factor of 1 to 4 (1 for 130-199 HU, 2 for 200-299 HU, 3 for 300-399 HU, and 4 for ≥400 HU) was assigned based on computed tomography density, and the CAC score was calculated as the area of the lesion multiplied by the weighting factor. 2 Patients were categorized into the following 4 groups based on their CAC scores: absent (CAC score = 0), mild (CAC score = 1-100), moderate (CAC score = 101-400), and severe (CAC score >400).
Statistical Analysis
All statistical analyses were performed using SPSS (version 26.0; SPSS Inc., Chicago, IL, USA) and R software (version 4.0.2; R Foundation for Statistical Computing, Vienna, Austria). The normality of continuous variables was determined using the Kolmogorov–Smirnov test. Continuous variables without a normal distribution are presented as medians (interquartile range) and were compared using the Mann–Whitney U-test. Categorical variables are presented as numbers (%) and were compared using the χ2 test. The optimal ALI cutoff value (39.29) for the diagnosis of CAD was determined using receiver operating characteristic (ROC) curves and Youden's index. This value was used for all analyses in the current study. Spearman's rank correlation coefficients were used to examine correlations between clinical variables and ALI. Variables with P-values <.20 in the univariate analysis were included in the multivariate analysis. Multivariate logistic regression analysis was performed to identify independent risk factors (statistical significance was set at P < .05), and a forward selection method was used to identify the most precise combinations for predicting CAD, CAC, and CAD with CAC. The “rms” package in R was used to establish nomograms based on these independent predictors. The discriminative ability, predictive accuracy, and clinical usefulness of the models were assessed using ROC curves, calibration plots, and decision curve analysis (DCA). DCA was performed using the “rmda” package in R. A total of 1000 bootstrap resamples were employed to reduce the overfitting bias.
Results
Patient Characteristics
In total, 549 patients with suspected CAD who underwent CCTA were included in our study (Figure 1) and assigned to the CAD (n = 396) and non-CAD groups (n = 153). Table 1 shows the clinical characteristics of the included patients. The CAD group exhibited a higher prevalence of male sex, chest pain, smoking, hypertension, diabetes, dyslipidemia, ischemic stroke, total cholesterol ≥5.2 mmol/L, triglycerides ≥1.7 mmol/L, and abnormal wall motion (all P < .05). Median height, body weight, creatinine, blood urea nitrogen, left atrium diameter, left ventricular end-systolic diameter, left ventricular end-diastolic diameter, and CAC scores were significantly higher in the CAD group than in the non-CAD group (all P < .05).

Screening flowchart of all patients enrolled in the study.
Baseline Clinical Characteristics for the CAD and non-CAD Groups.

Abbreviations: CAD, coronary artery disease; BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; WBC, white blood cell; ALB, albumin; CAC, coronary artery calcification; ALI, advanced lung cancer inflammation index.
When analyses were performed based on ALI, patients in the low-ALI group (ALI ≤39.29) were more likely to be male and have CAD and dyslipidemia than those in the high-ALI group (all P < .05). Neutrophil count, NLR, and CAC scores were higher in the low-ALI group (ALI ≤ 39.29) than in the high-ALI group, whereas BMI, ALB, and lymphocyte levels were lower (ALI >39.29; all P < .05) (Table 2).
Baseline Clinical Characteristics for the Low-ALI and High-ALI Groups.

Abbreviations: ALI, advanced lung cancer inflammation index; BMI, body mass index; ALB, albumin; NLR, neutrophil to lymphocyte ratio; CAD, coronary artery disease; CAC, coronary artery calcification.
Correlation Analysis
In the Spearman correlation analysis, ALI was negatively correlated with NLR, white blood cell count, neutrophil count, monocyte count, and CAC score (all P < .05), whereas ALB, BMI, total cholesterol level, triglyceride level, low-density lipoprotein cholesterol level, platelet count, and lymphocyte count were positively correlated with ALI (all P < .05) (Table 3).
Correlations of ALI With Other Clinical Parameters.
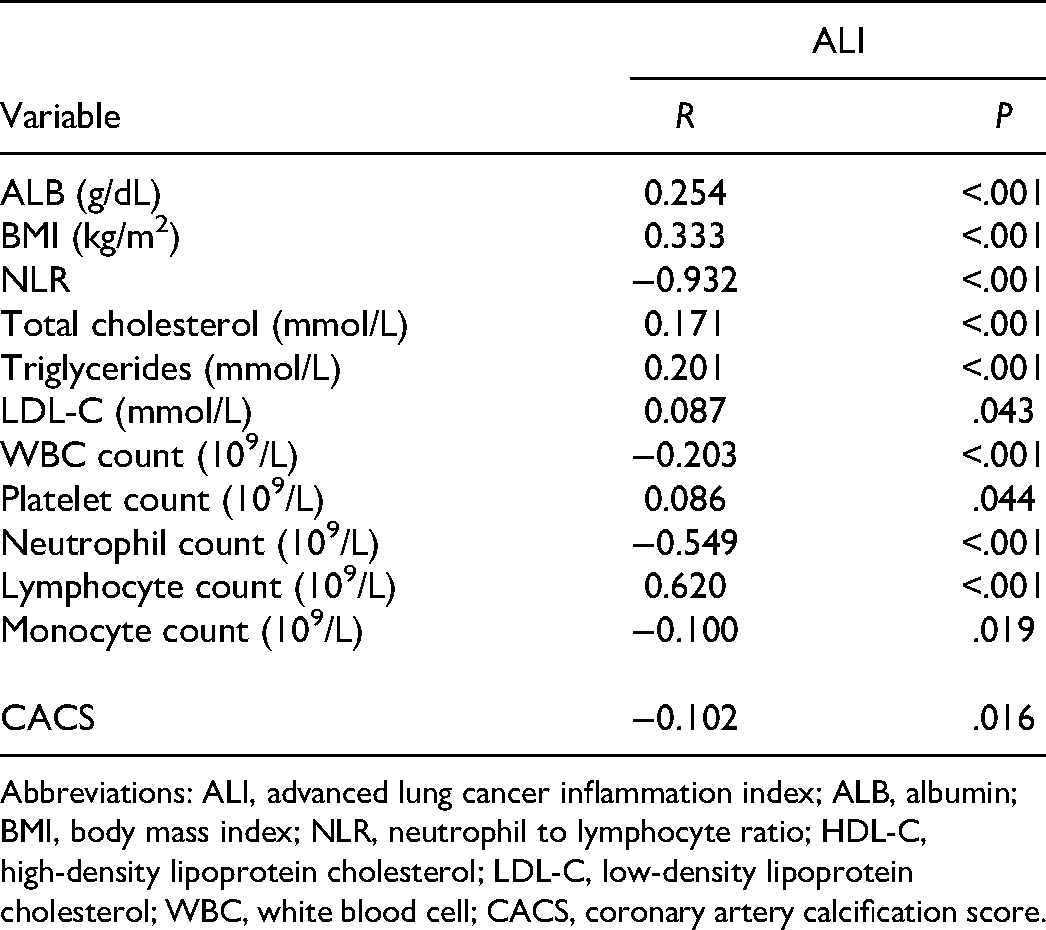
Abbreviations: ALI, advanced lung cancer inflammation index; ALB, albumin; BMI, body mass index; NLR, neutrophil to lymphocyte ratio; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; WBC, white blood cell; CACS, coronary artery calcification score.
Feature Selection and Nomogram Development
The forward stepwise logistic regression analysis identified male sex, hypertension, diabetes, dyslipidemia, ischemic stroke, and ALI as independent predictors of CAD and CAC (Tables 4 and 5). Male sex, hypertension, diabetes, dyslipidemia, and ALI were also identified as independent predictors of CAD with CAC (Table 6). Models incorporating these independent predictors were developed and presented as nomograms. Each predictor was assigned a point in the graphical interface of the nomogram, the bottom of which included a line indicating the total number of points. Scores for each predictor ranged from 0 to 100, and the total point value was determined by summing the scores for each predictor. The total score corresponded to the individual risk of developing CAD, CAC, or CAD with CAC (Figures 2 to 6).

Nomogram to estimate the risk of CAD. To estimate the risk of CAD, first identify the value for each axis, and then draw a vertical line upward to the point axis from the axis for each factor. Sum up the points for all factors and locate the value on the total point line. Subsequently, draw a vertical line down to the risk of CAD. For example, the factors of male sex (100 points), hypertension (85.5 points), diabetes (48 points), absence of dyslipidemia (0 points), ischemic stroke (75 points), and ALI ≤39.29 (57.5 points) result in a total of 366 points, which gives an estimated probability of 94% for the occurrence of CAD.

Nomogram to estimate the risk of CAC. To estimate the risk of CAC, first identify the value for each axis, and then draw a vertical line upward to the point axis from the axis for each factor. Sum up the points for all factors and locate the value on the total point line. Subsequently, draw a vertical line down to the risk of CAC. For example, the factors of male sex (100 points), hypertension (72.5 points), absence of diabetes (0 points), dyslipidemia (67.5 points), ischemic stroke (81 points), and ALI ≤39.29 (48 points) result in a total of 369 points, which gives an estimated probability of 92% for the occurrence of CAC.

Nomogram to estimate the risk of CAD with CAC. To estimate the risk of CAD with CAC, first identify the value for each axis, and then draw a vertical line upward to the point axis from the axis for each factor. Sum up the points for all factors and locate the value on the total point line. Subsequently, draw a vertical line down to the risk of CAD with CAC. For example, the factors of female sex (0 points), hypertension (87 points), diabetes (63 points), dyslipidemia (67.5 points), and ALI ≤39.29 (48 points) result in a total of 265.5 points, which gives an estimated probability of 77% for the occurrence of CAD with CAC.
Multiple Logistic Regression Analysis for Independent Predictors of CAD.

Abbreviations: CAD, coronary artery disease; SE, standard error; OR, odds ratio; CI, confidence interval; ALI, advanced lung cancer inflammation index.
Multiple Logistic Regression Analysis for Independent Predictors of CAC.

Abbreviations: CAC, coronary artery calcification; SE, standard error; OR, odds ratio; CI, confidence interval; ALI, advanced lung cancer inflammation index.
Multiple Logistic Regression Analysis for Independent Predictors of CAD with CAC.

Abbreviations: CAD, coronary artery disease; CAC, coronary artery calcification; SE, standard error; OR, odds ratio; CI, confidence interval; ALI, advanced lung cancer inflammation index.
Validation of the Nomograms
For the CAD nomogram, the area under the curve (AUC) was 0.739 (95% confidence interval [CI], 0.693-0.785; Figure 3a). The nomogram had a bootstrapped concordance index of 0.739 and was well-calibrated (Figure 3b). For the CAC nomogram, the AUC was 0.728 (95% CI, 0.684-0.772) (Figure 5a). The probabilities predicted by the nomogram were well-matched with clinical outcomes (Figure 5b). For the CAD with CAC nomogram, the AUC was 0.717 (95% CI, 0.673-0.761) (Figure 7a), and good agreement was observed between the predicted and observed probabilities of CAD with CAC (Figure 7b).
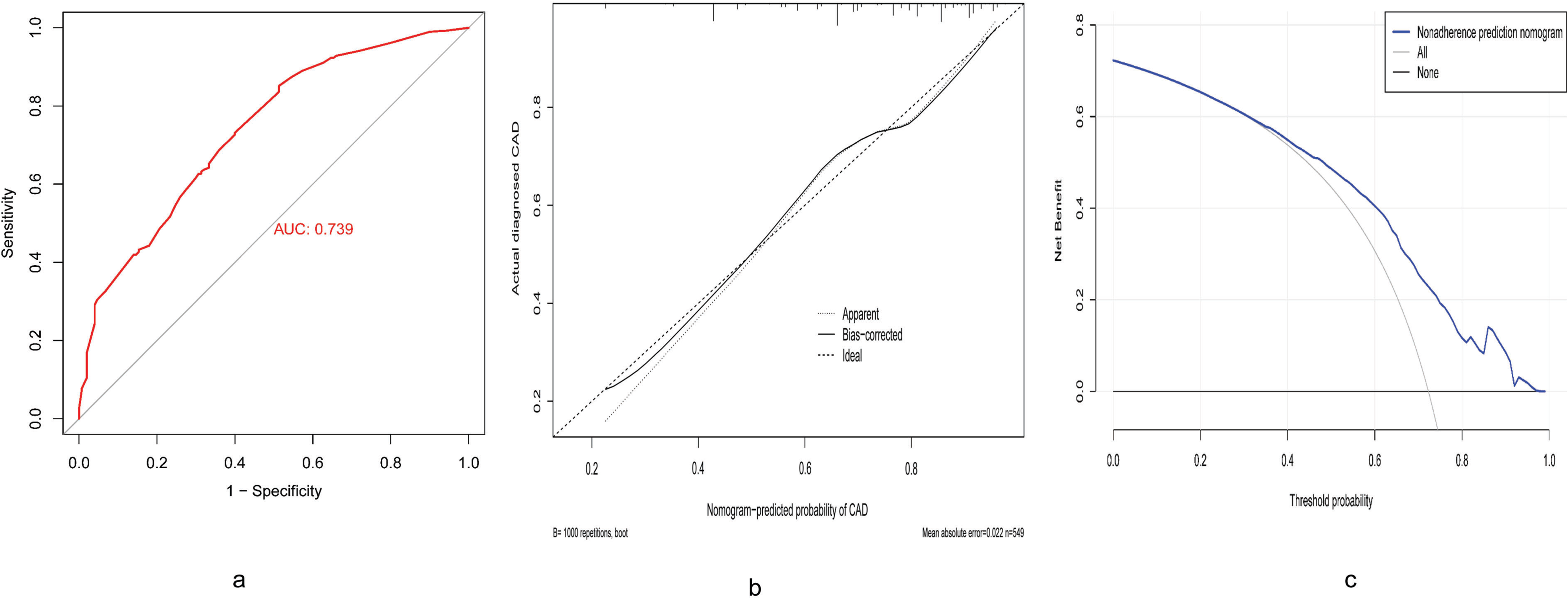
Receiver operating characteristic curve (a), calibration curve (b), and decision curve analysis (c) for the CAD nomogram.

Receiver operating characteristic curve (a), calibration curve (b), and decision curve analysis, (c) for the CAC nomogram.

Receiver operating characteristic curve (a), calibration curve (b), and decision curve analysis (c) for the CAD with CAC nomogram.
Clinical Benefit Evaluation
To evaluate the ability of the nomograms to improve clinical decision-making, each model was evaluated using DCA. When the threshold probability was approximately 38% to 98%, the benefit of using the CAD nomogram was beyond both the thin gray line (treat-all scheme) and the thick gray line (treat-none scheme) (Figure 3c). Furthermore, the threshold probability could be set between 30% and approximately 88% when the benefit of using the CAC nomogram was greater than either the treat-all or treat-none scheme (Figure 5c). Moreover, the DCA demonstrated a net benefit of using the nomogram to predict CAD with CAC when the threshold probability was approximately 28% to 88% (Figure 7c).
Discussion
In this study, we developed and validated 3 ALI-based nomograms for predicting CAD, CAC, and CAD with CAC. Our multivariate logistic regression analysis revealed that ALI was an independent risk factor for CAD, CAC, and CAD with CAC. The odds ratios for the associations of ALI with CAD, CAC, and CAD with CAC risk were 1.873 (95% CI, 1.177-2.982), 1.661 (95% CI, 1.088-2.534), and 1.608 (95% CI, 1.069-2.420), respectively. Our analyses suggested that male sex, hypertension, diabetes, dyslipidemia, ischemic stroke, and ALI were independent predictors of CAD and CAC. Male sex, hypertension, diabetes, dyslipidemia, and ALI were also identified as independent predictors of CAD with CAC. The AUC values for the nomograms based on these predictors were 0.739 for the CAD nomogram, 0.728 for the CAC nomogram, and 0.717 for the CAD with CAC nomogram, all of which exhibited good diagnostic value (AUC 0.7). The calibration curve and DCA also indicated good diagnostic performance of the nomograms. To the best of our knowledge, this is the first clinical diagnostic model to incorporate ALI for identifying the risk of CAD, CAC, and CAD with CAC in patients who have undergone CCTA.
Atherosclerotic lesion progression is associated with intimal calcification. 26 CAD has long been regarded as a chronic low-grade, subclinical, systemic inflammatory disease, and the role of calcification in CAD is gaining importance given that plaque calcification is closely related to the level of vascular inflammation. 27 Non-invasive tests have been increasingly used for risk stratification and to aid in the clinical decision-making process in patients with suspected CAD. 28 Previous research has demonstrated the clinical utility of CAC scores, reporting that an absence of calcium reliably excludes the diagnosis of obstructive coronary artery stenosis. 29 Furthermore, higher calcium scores have been associated with a greater likelihood of future acute coronary events. 26 Considering the important role of inflammation in atherosclerosis and CAC, exploring novel risk factors that can be used to identify each patient's level of risk remains crucial.
The novel inflammation-related marker ALI was first evaluated as a powerful prognostic index for metastatic non-small cell lung cancer. 11 The ALI combines BMI, ALB, and NLR (BMI × ALB/NLR), all of which play pivotal roles in nutritional, immune, and systemic inflammation status.12,30 Previous studies have reported that the ALI is associated with non-small cell lung cancer, 11 esophageal squamous carcinoma, 17 colorectal cancer, 15 and diffuse large B-cell lymphoma. 16 A low ALI based on a decreased BMI, lower ALB, and/or high NLR indicates a high level of systemic inflammation. 31 Among these 3 factors, BMI may represent the patient's nutritional status, and it is not rare for patients with CAD to experience malnutrition characterized by anorexia, weight loss, insulin resistance, and increased breakdown of muscle protein.13,32 These conditions lead to a poor prognosis and are often observed in patients with chronic heart disease. 33 A similar association between malnutrition, inflammation, and atherosclerosis has also been reported in patients with end-stage renal disease. 34
Inflammation and oxidative stress are at the forefront in the initiation and development of atherosclerosis and the onset of cardiovascular disease.14,35,36 ALB, which is the major protein in human plasma, plays an important role in maintaining a stable plasma colloid osmotic pressure and also functions as a transport protein in combination with other substances. 37 ALB synthesis is regulated by nutrient intake, insulin levels, and oncotic pressure. 32 Serum ALB exhibits anti-inflammatory, antioxidant, anticoagulant, and antiplatelet aggregation activity as well as a colloid osmotic effect; thus, hypoalbuminemia may act as a risk factor. 36 Furthermore, there is increasing evidence that hypoalbuminemia on admission is a strong independent predictor of long-term mortality in patients with acute coronary syndrome.38,39
The NLR is a classic biomarker for systemic inflammation and is based on the ratio of circulating neutrophils and lymphocytes, which can be calculated easily based on the results of routine blood tests. 19 Researchers have proposed that neutrophil extracellular traps are released from stimulated neutrophils in a process known as NETosis, which is closely related to inflammation, thrombosis, oxidative stress, and cardiovascular diseases. 40 Low lymphocyte counts have also been associated with poor clinical outcomes in patients with CAD, and lymphocytopenia may reflect a poorly regulated immune response. 13 Thus, an increased NLR based on increased neutrophil counts and/or decreased lymphocyte counts indicates an imbalance between the innate and adaptive immune systems, resulting in a systemic increase in proinflammatory cytokines. 41 Previous studies have shown that an elevated NLR is associated with coronary artery calcium levels and CAD severity.27,42 These mechanisms may have influenced the associations between malnutrition, inflammation, and cardiovascular outcomes in this study.
In summary, we constructed and validated relatively accurate clinical nomograms, which demonstrated adequate discrimination and calibration, in predicting the individual risk of CAD, CAC, or CAD with CAC. Our findings highlight the potential of these nomograms to improve individualized patient counseling and clinical decision-making regarding treatment for patients with CAD, CAC, and CAD with CAC. Compared with classic markers of inflammation such as C-reactive protein, the ALI is easy to calculate in clinical practice, suggesting that it may be a more useful clinical predictor of CAD and CAC.
Limitations
This study had several limitations, including its single-center design, which may have resulted in selection bias. Second, although our nomograms were validated using bootstraps with 1000 resamples, further prospective multicenter studies should be performed for external validation.
Conclusion
In this study, we developed and validated nomograms incorporating a novel inflammation-related marker (ALI) and other classical clinical risk factors to aid in predicting the risk of CAD, CAC, and CAD with CAC. The proposed nomograms demonstrated the pivotal role of systemic inflammation in predicting these diseases. Our findings highlight the potential of these nomograms to improve individualized patient counseling and clinical decision-making regarding personalized treatment for CAD, CAC, and CAD with CAC.
Footnotes
Acknowledgments
The authors acknowledge the staff at the Affiliated Hospital of Chengde Medical University who contributed to this study. We thank Mingdong Li for the assistance with the data analysis.
Authors’ Note
Ethical approval was obtained from the Institutional Review Board of The Affiliated Hospital of Chengde Medical University (Number: LL164). Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Technology Innovation Guidance Project-Science and Technology Work Conference from Hebei Provincial Department of Science and Technology (202011) to Dr Lixian Sun, and from the Hebei Provincial Department of Education Graduate Innovation Funding Project (No. CXZZSS2021138) to Wenjun Fan.