
Abstract
The pathogenesis of chronic refractory immune thrombocytopenia (C/RITP) is mechanistically complex and considerably varies across patients. Few studies have focused on the genetic characteristics of C/RITP in children. The aim of this study was to analyze and summarize the clinical manifestations and genetic characteristics of C/RITP children with mutations in immune-related genes. In the study, 51 children with variants in immune-related genes (mutation group) and 103 children with no abnormal mutations (control group) were enrolled. Children in the mutation group showed severity of hemorrhage, a higher incidence of abnormal immunological indices, and an increased expression of SLE biomarkers. The number of peripheral T and B lymphocytes in the mutation group significantly increased. Nine patients (17.6%) had probable pathogenic variant genes associated with primary immunodeficiencies (TNFRSF13B, CARD11, CBL, and RAG2), and 42 patients (82.4%) had variants of uncertain significance in 23 genes. C/RITP patients with variants in immune-related genes had more severe bleeding, abnormal immunological indices, and an increased expression of SLE biomarker. Next-generation sequenciong (NGS) might be a useful way to differentiate those patients from C/RITP.
Introduction
Immune thrombocytopenia (ITP) is an acquired hemorrhagic autoimmune disease. However, because of its complex, heterogeneous pathogenesis, its mechanistic cause remains unclear. Various studies have reported that ITP results from a mixture of genetic and acquired factors. 1 ITP is a self-limiting disease with good prognosis, and the extent of bleeding in children is usually mild.2–4 Only 20% children eventually develop chronic ITP (CITP) or refractory ITP (RITP). 1 The presence of platelet autoantibodies is used to diagnose classical ITP. T lymphocytes and B lymphocytes play an important part in the initiation and maintenance of C/RITP. T lymphocyte abnormalities in C/RITP have been demonstrated, such as unbalance of Th1/Th2 ratios, decrease in T-regulatory cells, and increase in Th17 and Th22 cells.5–7 Moreover, autoimmune disorders, such as systemic lupus erythematosus, antiphospholipid antibody syndrome, and rheumatoid arthritis are prone to developing ITP. 8 Therefore, detection of relevant immunological indices is particularly important for C/RITP patients, such as SLE biomarkers (antinuclear antibodies titer), antinuclear antibodies, antidouble-stranded DNA antibody, anti-ENA antibodies, anticardiolipin antibody, and rheumatoid factor. One study found that some chronic ITP children have a positive family history of ITP. 9 There is also evidence for a genetic predisposition to ITP, which might in part lie within immune-related genes. 10
However, few studies have focused on the clinical features and genetic basis of C/RITP children with mutations in immune-related genes. To date, studies have not compared C/RITP in children with and without mutations in immune-related genes. In this study, we retrospectively screened the high-throughput next-generation sequencing (NGS) data of children with C/RITP. Notably, we found significant differences in the clinical outcomes of C/RITP children with immune-related mutations compared to children without detectable genetic abnormalities.
Materials and Methods
Patients
We retrospectively evaluated the NGS data of 252 C/RITP children from March 2016 to March 2019 in our medical center. In total, 40 patients out of 252 patients with C/RITP were diagnosed with hereditary thrombocytopenia, 140 patients without any identified genetic defect, and 72 patients with a high frequency of gene mutation. According to the NGS data, we divided the 72 patients to two groups, immune-related gene mutation group and non immune-related gene mutation group (Figure 1).

Summary of inclusion patients.
In the study group, 51 patients with immune-related gene mutation of 72 patients with a high frequency gene mutation were included (Figure 1). The inclusion criteria were as follows: We enrolled children with (1) clinically relevant gene variants associated with thrombocytopenia and/or autoimmune diseases, as determined by NGS, especially those affecting proteins predicted to be “harmful” or mutations in genes located in key protein domains. (2) A mutation that was a heterozygous mutation of an autosomal dominant inheritance or a complex heterozygous mutation of autosomal recessive inheritance, but the pathogenicity of the mutation was uncertain significance (usually an uncommon mutation without prior literature report). Additionally, 103 patients with complete clinical data out of 140 patients without any identified genetic defect were included in the control group.
We recorded the relevant clinical data including the sex, age, predisposing factors, location of hemorrhage, severity of hemorrhage, blood count results, serum immunoglobulin levels, immune parameters, type of treatment, treatment response, and death. The response criteria were defined according to the consensus of Chinese experts. 11 The severity of hemorrhage was recorded according to the score sheet developed by Buchanan. 12 We also collected the data from the parents of patients and follow up.
The study was conducted according to the Declaration of Helsinki. The parents of all patients provided informed consent, and this study was approved by the Ethical Committee of Beijing Children's Hospital.
Genetic Analysis
DNA samples were isolated from whole blood using a DNA extraction kit (Qiagen, China). Targeted genes associated with thrombocytopenia and/or autoimmune diseases were selected using a gene capture strategy and a GenCap custom enrichment kit (MyGenostics, China). The immune-related genes are as follows: TNFRSF13B, CARD11, CBL, RAG2, AIRE, C1R, LAT, LRBA, CASP10, CD40LG, CTLA4, FASLG, CATA2, IFIH2, IL2KG, JAK2, LZTR1, NHEJ1, NLRP1, NLRP2, NLRP12, PIK3CD, PIK3R1, and PLCG2. The NGS panel was designed according to the Human Gene Mutation Database (HGMD). The biotinylated capture probes were designed to tile all the exons without any repeated regions. The captured DNAs were eluted, amplified, and purified. The enriched libraries were sequenced for 150-bp paired-end reads using Illumina HiSeq X Ten.
The raw data were saved in the FASTQ file format. Illumina sequencing adapters and low-quality reads (<80 bp) were filtered using Cutadapt. Clean reads were aligned to the University of California Santa Cruz hg19 human reference genome using the Burrows–Wheeler Alignment tool (BWA,V.0.7.3). Duplicated reads were removed using Picard. Insertions, deletions, and single-nucleotide polymorphism variants were detected and filtered using a Genome Analysis Toolkit. Then, the identified variants were annotated using ANNOVAR (ANNOtate VARiation). The pathogenicity of mutations was assessed according to the American College of Medical Genetics and Genomics (ACMG) guidelines. All the genetic results and pathogenicity analysis were verified by three genetics experts and two clinicians.
Statistical Analysis
Statistical analysis was performed using SPSS software. All the data are reported as mean ± standard deviation (SD) or as frequency and percentage. Where appropriate, student's st-tests, χ2 testing, or Fisher exact test were performed for comparisons between controls and patients with immune-related mutations.
Results
In total, we identified 252 C/RITP patients who were to be evaluated for a cause by NGS. 72 patients with a high frequency of gene mutation cannot be diagnosed with hereditary thrombocytopenia. We divided the 72 patients into immune-related gene mutation group and non immune-related gene mutation group. We focused on the clinical features and genetic basis of 51 patients with immune-related gene mutation. 103 patients with complete clinical data of 140 patients without any identified genetic defect were included in the control group (Figure 1). The complete demographics and clinical characteristics are shown in Table 1, and the information about mutant genes is shown in Table 2.
Clinical Characteristics of the 154 Patients With C/RITP.
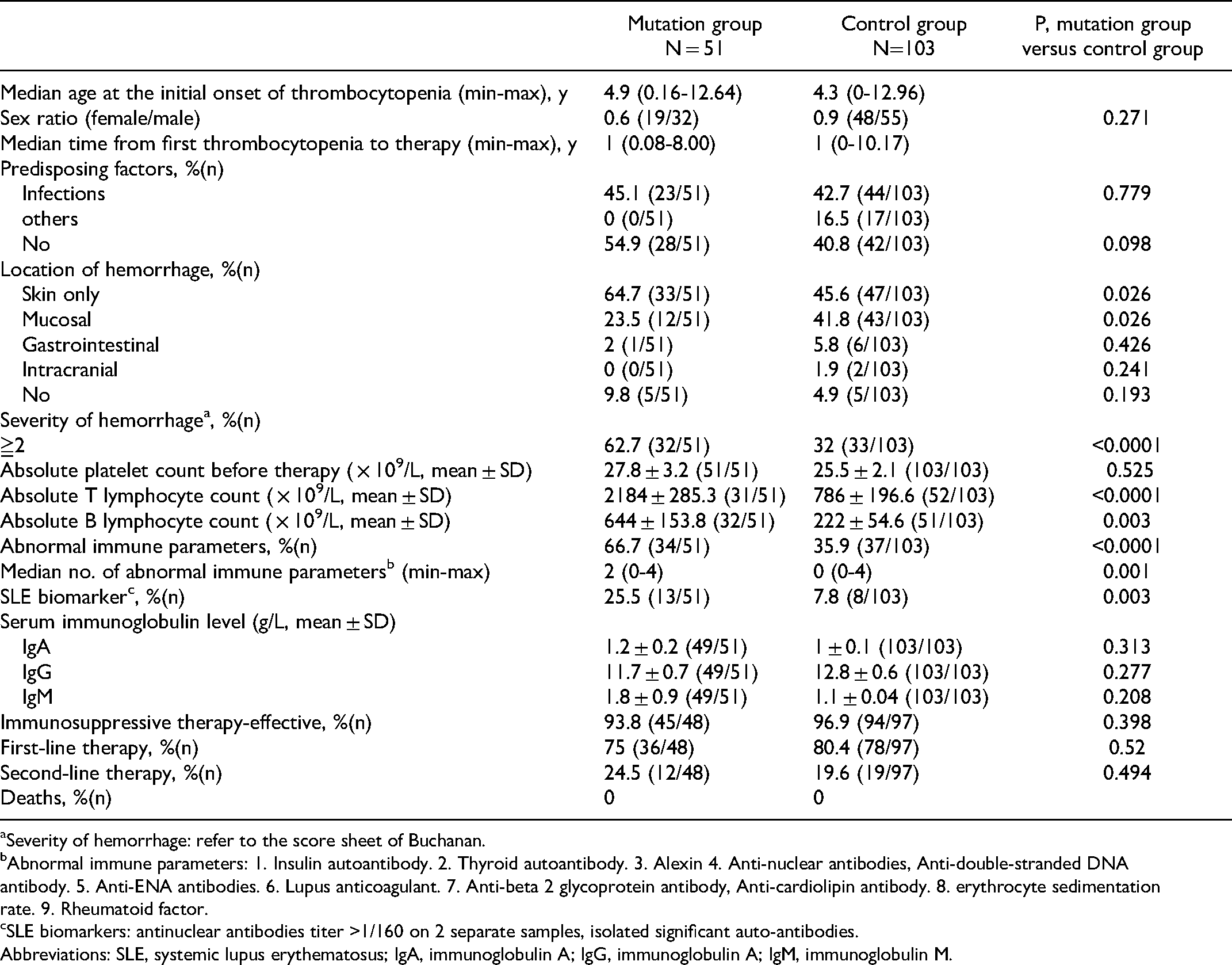
Severity of hemorrhage: refer to the score sheet of Buchanan.
Abnormal immune parameters: 1. Insulin autoantibody. 2. Thyroid autoantibody. 3. Alexin 4. Anti-nuclear antibodies, Anti-double-stranded DNA antibody. 5. Anti-ENA antibodies. 6. Lupus anticoagulant. 7. Anti-beta 2 glycoprotein antibody, Anti-cardiolipin antibody. 8. erythrocyte sedimentation rate. 9. Rheumatoid factor.
SLE biomarkers: antinuclear antibodies titer >1/160 on 2 separate samples, isolated significant auto-antibodies.
Abbreviations: SLE, systemic lupus erythematosus; IgA, immunoglobulin A; IgG, immunoglobulin A; IgM, immunoglobulin M.
Genetic Results of 51 Patients With C/RITP.

Clinical Characteristics
No significant difference was observed in the mean platelet count before therapy across groups. However, we found that the hemorrhage of patients was more severe in the mutation group (Figures 2A and 2B). Infections occurred in 45% of the mutation group and in 43% of the control group, a nonsignificant difference. Next, we compared the patients’ immunological indices, such as insulin autoantibody, thyroid autoantibody, alexin, antinuclear antibodies, antidouble-stranded DNA antibody, anti-ENA antibodies, lupus anticoagulant, anti-beta 2 glycoprotein antibody, anticardiolipin antibody, erythrocyte sedimentation rate, and rheumatoid factor in the two groups. The patients in the mutation group had a higher incidence of abnormal immunological indices (Figure 2D) and an increased expression of SLE biomarkers (P = 0.003). The number of peripheral T and B lymphocytes in the mutation group significantly increased (Figure 2C). No significant difference was observed in the total immunoglobulin serum level between the two groups.

The clinical characteristics of mutation group and control group patients.
Immunosuppressive Therapy
No significant difference in immunosuppressive therapy-effective was observed between the two groups. Then, we compared the second-line therapeutic choice between the two groups. 45 children (out of 48 children, 94%) needed immunosuppressive therapy in the mutation group, and 12 of those cases required further second-line treatment. Similarly, in the control group, 94 children (out of 97 children, 97%) needed immunosuppressive therapy, and 19 cases needed second-line treatment, a nonsignificant difference.
Genetic Analysis
A total of nine cases had probably pathogenic mutations in four genes (TNFRSF13B, CARD11, CBL1, RAG2). Another 42 cases had variants of uncertain significance in 23 genes (AIRE, C1R, LAT, LRBA, CARD11, CASP10, CBL, CD40LG, CTLA4, FASLG, GATA, IFIH1, IL2KG, JAK2, LZTR1, MHEJ1, NLRP1, NLRP2, NLRP12, PIK3CD, PIK3R, PLCG2, and TNFRSF13B). In the mutation group, 49 patients had autosomal heterozygous mutations, and two patients had autosomal homozygous mutations either in CD40LG (n = 1) or IL2KG (n = 1). Nine patients had variants in six genes (CTLA4, CBL, LRBA, RAG2, PIK3CD, and FASLG) known to be implicated in primary immunodeficiencies.13–18 Eight patients had a variant in a gene (TNFRSF13B) that has previously been shown to predispose individuals to familial or sporadic ITP. 19 A total of 34 patients had mutations in 17 genes that are known to be immune related. However, no studies previously reported a role of these genes in immunodeficiency or autoimmune disease.
Two of the variants were spontaneous mutations (CARD11 and CBL). Nine children had a set of six variants (TNFRSF13B, FASLG, GATA2, IL2KG, JAK2, and PLCG2) inherited from their mothers, and five children had a set of four variants (TNFRSF13B, CASP10, CBL, and CTLA4) inherited from their fathers. However, none of the parents of those children had immunodeficiency or autoimmune disease.
Discussion
This retrospective study focused on identifying differences between the two observed groups of pediatric patients with C/RITP:1) patients with mutations in immune-related genes that could not be diagnosed with hereditary thrombocytopenia and 2) patients without any detected genetic abnormalities.
We found that, compared with the control group, children with mutations in immune-related genes had more severe bleeding. Further, the incidence of abnormal immune phenotype was higher in the mutation group, such as the findings of increased peripheral T and B lymphocytes, a higher incidence of abnormal immunological indices, and an increased expression of SLE biomarkers. Self-tolerance is typically maintained by a combination of central tolerance and peripheral tolerance.20–24 This type of analysis of immune-related genes can provide a wealth of information about the mechanisms of autoimmune-related diseases. The increased risk of various abnormal immune phenotypes in the mutation group might indicate a genetic predisposition toward immunodeficiencies. However, the identification of specific mechanisms is a topic for future research. Patients in the mutation group experienced an earlier onset of immune abnormalities. In principle, this suggests that they require more frequent immunosuppressive therapy and use of second-line treatments, and these children would be expected to have worse prognosis. To our surprise, no significant difference was observed in the frequency of immunosuppressive therapy across the two groups. This may be due to the relatively small number of patients who underwent immunosuppressive therapy in our study.
In this study, we found that some children with C/RITP had variants in immune-related genes that were predicted to be probably pathogenic. According to our inclusion criteria, we need the variants of uncertain significance in the pathogenicity, but the nine cases cannot be diagnosed with hereditary thrombocytopenia, gene variants associated with thrombocytopenia, and/or autoimmune diseases, so we included these patients. However, we found some variants of genes in primary immunodeficiencies, including CTLA4, LRBA, PIK3CD, RAG2, and CBL. PLCG2 mutations have been reported to be involved in autoinflammatory disease with immunodeficiency.25,26 CARD11 mutations have been reported to cause primary immune disorder and even severe combined immune deficiency.27,28 In our cohort, we identified a number of C/RITP patients with variants in autoimmunity- or immunodeficiency-related genes. However, no parents of those children had immunodeficiency or autoimmune disease. Some studies have confirmed that the clinical manifestations of diseases might occur many years later. 13 Therefore, according to the current data, we supposed that heterozygosity for the identified probable pathogenic mutations may not cause disease. The homozygous mutations in CD40LG and IL2KG were variants of uncertain significance, but the pedigree validation needs to be verified. Meanwhile, the variants of uncertain significance in genes previously reported to predispose to ITP or to be in genes related to autoimmunity/immune disease were still the variants of uncertain significance in this cohort.
This study found that C/RITP patients with variants in immune genes had more severe bleeding, as well as a greater frequency of abnormal immunological indices and an increased expression of SLE biomarkers. The NGS panel was based on the updated HGMD in our study. Therefore, NGS might be an applicable and useful way to differentiate those patients from C/RITP. Rivalta et al. 29 showed that NGS evolved into a routine application in evaluating primary immune deficiency disease in patients with autoimmune cytopenia. Ma etal. found that NGS could be applied earlier in the differential diagnosis for suspicious common variable immunodeficiency (CVID) in children with ITP. 30 Because our targeted genes are associated with thrombocytopenia and/or autoimmune diseases, physicians should differentiate those patients from the primary immune deficiency disease, such as CVID.
Our study has several important shortcomings. First, this study is a small, single-center, retrospective study. Second, owing the technical defects, most of the patients’ mutations had no protein prediction, and pedigree validation was not performed.
Conclusion
C/RITP patients with variants in immune genes had more severe bleeding, as well as a greater frequency of abnormal immunological indices and an increased expression of SLE biomarkers. NGS might be beneficial for the early diagnosis of those patients from children with C/RITP. The findings of this study might have implications for future large-scale, multicenter studies on the pathogenesis and diagnosis of those pediatric C/RITP.
Footnotes
Author Contributions
Dr Wu contributed to the study design. Dr Zhao wrote the manuscript. Dr Ma, Zhu and Zhang collected the data and conducted critical revisions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No. 81970111), Beijing Natural Science Foundation of China (No. 7192064), Pediatric Medical Coordinated Development Center of Beijing Municipal Administration of hospitals (No. XTZD20180205), and National Science and Technology Key Projects (No. 2017ZX09304029001).