
Abstract
Immune thrombocytopenia (ITP) appears to be a heterogeneous disease. In some patients, autoimmunity may be associated with an inflammatory process, and in other patients, low platelets may interfere with other aspects of the coagulation system. Either may predispose to thrombosis or bleeding. Further investigation of the interactions of platelets, with inflammatory cytokines and endothelial biomarkers, may help us to better understand the disease, and to recognize those patients at risk of bleeding, or conversely thrombosis. The aim of this work is to estimate von Willebrand factor (vWF) and vascular cellular adhesion molecule (V-CAM) serum levels in adult immune thrombocytopenic patients (ITP) and to decipher their possible clinical correlates. Eighty adults (≥ 18 years) were enrolled in the study; naive newly diagnosed 40 patients with primary ITP (according to the ASH 2019) and 40 sex and age-matched healthy controls, all groups are subjected for complete blood count (CBC), liver, and renal function tests, ESR, CRP, V-CAM, and VWF-Ag by enzyme-linked immunosorbent assay (ELISA). There was a highly statistically significant difference between case and control as regards to the mean level of VWF-Ag and V-CAM. vWF and V-CAM could serve as biomarkers for endothelial alterations and should be investigated as a predictor of thrombocytopenic bleeding and tailor patient management accordingly.
Introduction
Besides their role in hemostasis, platelets are considered also a key player for preserving endothelial functions and integrity. Platelets continuously support the barrier function of the resting endothelium, and after inflammation by infiltrating leukocytes; they prevent or heal vascular injuries. These vascular protective actions of platelets are apart from their ability to stop bleeding. 1
Constitutive release of proangiogenic cytokines and growth factors from platelets maintains vascular integrity. These molecules bind to specific receptors on the surface of endothelial cells (ECs). When platelets numbers decrease dramatically, molecular disassembly of adjacent intercellular endothelial junctions occurs which leads to vascular fragility and liability to bleed. 2
In addition, platelets have multiple regulatory functions on endothelial progenitor cell development as well. 3
Many patients with immune thrombocytopenia (ITP) have a bleeding time that is disproportionately short for the degree of thrombocytopenia. 4
It had been established that the vascular endothelium, rather than being a mere wall between intravascular and subendothelial compartments, is a widely spread organ responsible for many functions like regulation of hemodynamics, angiogenic vascular remodeling, metabolic, synthetic, anti-inflammatory, and anti-thrombogenic processes. 5
Endothelial activation is based on its pivotal role in many diseases like coronary artery disease, hypertension, cerebrovascular disease, and diabetes. And novel therapies aimed at alleviating the morbidity and mortality from these conditions. It may be possible to apply knowledge gained by studying one disease to another disease process. 6
Endothelial cell dysfunction (ECD) is a syndrome induced by diverse intrinsic and extrinsic factors that lead to disturbances in the barrier function of the vascular endothelium; in addition to its impaired anti-thrombogenic properties; angiogenic competence; proliferative capacity, disordered regulation of vascular smooth muscle tonicity, and migratory properties; and perturbed synthetic functions and impedance of neutrophils and monocytes from diapedesis. 7
Thrombocytopenia per se is associated with ECD, as evidenced by spontaneous leakage of blood at the microvascular. Platelet antibodies may cross-react with EC antigens and cause further endothelial damage, which may increase bleeding. 8
Vascular cellular adhesion molecule-1 (VCAM-1) belongs to the immunoglobulin supergene family and is a ligand to the very late antigen-4, a β-integrin found on the surface of mononuclear cells. VCAM-1 expression is restricted to ECs and occasional fusiform cells. VCAM-1 is not expressed on healthy ECs. It has been suggested that VCAM-1 expression may result in endothelial activation. 9
The role and level of vWF, which is exclusively synthesized and secreted by the ECs, at least in the liver, is not limited to the ECS of the large veins but is also of the ECs of the hepatic sinusoid, so many factors affect its level and its role in bleeding and hemostasis is linked to cellular factors and coagulation proteins. 10
In an ITP model, thrombocytopenia had led to an alteration in endothelial function, and that the von Willebrand factor (vWF) had served as a marker of EC injury. 11
Aim of the Study
The aim is to estimate vWF and vascular cellular adhesion molecule (V-CAM) serum levels (biomarkers of endothelial activation) in adult immune thrombocytopenic patients (ITP) and to decipher their possible clinical correlates.
Subjects and Methods
Patients
Eighty adults (≥ 18 years) were enrolled in this Case–Control study; 40 treatment naïve patients with primary ITP (according to the ASH 2019 clinical practice guidelines for ITP criteria) and 40 sex and age-matched healthy controls.
Patients were sequentially selected from the hematology unit at the Menoufia University Hospitals in the period from December 2019 to December 2020.
All participants were volunteers, and all of them signed written informed consent with explaining the aim of the study before the study initiation.
Approval of the study protocol was obtained by the local Ethical Scientific Committee of Menoufia university's institutional review board under number (MNF119/2019).
Patients with a family history of platelets or coagulation defects, pregnant females, acute or chronic inflammatory disorders as well as patients with non-ITP or secondary ITP (eg HCV, autoimmune disease, lymphoproliferative diseases, and thyroid disease, etc.) were excluded.
All participants were subjected to detailed medical history, complete physical examination, and abdominal ultrasound and laboratory investigations including:
Complete blood count (CBC) and blood film.
Kidney and liver function tests, hepatitis C virus antibodies (HCV-Abs), HBsAg, HBcAb, HIV antibodies, coagulation profiles, antinuclear antibody (ANA), thyroid-stimulating hormone (TSH), H. pylori Ag in stool, CRP, ESR, fasting blood sugar (FBS), HA1C, and finally bone marrow examination (if atypical blood film).
Endothelial activation biomarkers (VCAM and vWF) plasma levels using commercially available enzyme-linked immunosorbent assay (ELISA) kits.
Sampling
Ten mL of blood sample were taken by sterile venipuncture, after minimal venous stasis using sterile disposable syringes.
The blood samples were distributed as follows:
Four mL of blood were delivered to a vacutainer plain test tube, and then the serum was separated by centrifugation at 3000 rpm for 10 min and half of the separated serum was used for the analysis of liver function tests, renal function tests, TSH, CRP, viral hepatitis markers ANA; the other half was separated, aliquoted, and stored at −80°C for the measurement of VCAM and VWF antigen
Two mL of blood were delivered to a vacutainer plastic tube containing ethylenediaminetetraacetic acid (EDTA)and used for CBC with film.
Two mL of blood were delivered to a vacutainer plastic tube containing sodium citrate (4:1) (3.8%) for ESR measurement by Westergren method.
Two mL of blood were delivered to a vacutainer plastic tube containing sodium citrate (9:1) (3.2%) for coagulation profile.
Methods
CBC using Sysmex XT-1800i automated hematology analyzer (Sysmex Corporation), and then BM aspirate was done if needed.
Liver function tests (eg total bilirubin, direct bilirubin, albumin, total protein, AST, ALT), renal function tests, and CRP were analyzed using Cobas 6000 analyzer (c501 module) (Roche).
Serum HCV-Abs, HbsAg, and HIV Ab were measured using Cobas e601 auto analyzer (Roche).
Prothrombin time and activated partial thromboplastin time were done by Sysmex CS-1600 automated hemostasis testing (Sysmex Corporation).
ANA was done by Algeria automated analyzer.
Serum levels of endothelial activation biomarkers (VCAM and VWF-Ag) was done by ELISA that is designed to measure the amount of the target that bounded between a matched antibody pair. A target-specific antibody has been pre-coated in the supplied microplate wells. Standards, samples, or controls are then added into these wells and is bind to the immobilized (capture) antibody. The sandwich is then formed by the addition of the second (detector) antibody, and finally, a substrate solution is added that will react with the Enzyme–Antibody–Target complex to produce a measurable signal. The intensity of this signal is directly proportional to the concentration of the present target in the original specimen.
VCAM-1 was measured using the human (VCAM-1) ELISA kit (Cusabio) with a detection range from 1.563 ng/mL to 100 ng/mL that measures VWF in less than 5 h according to the manufacturer's instructions
VWF-Ag measurement: using VWF Human ELISA Kit Catalog #
Statistical Analysis
Data were collected, tabulated, and statistically analyzed using an IBM personal computer with Statistical Package of Social Science (SPSS) version 22 (SPSS, Inc.).
Descriptive statistics: in which quantitative data were presented in the form of mean, standard deviation (SD), range, and qualitative data were presented in the form of numbers and percentages. Analytical statistics is used to find out the possible association between studied factors and the targeted disease. The used tests of significance included Chi-square test (χ2), Fischer exact test, and Student’s t-test.
Results
Table 1 shows all characteristics of the studied ITP cases (N = 40) like demographic distribution and basic laboratory findings and the coagulation profile and bleeding severity in addition to serum von Willebrand and VCAM. Mean age among cases was equal to 46.2 ± 12.7. There were 16 (40%) males and 24 (60%) females among cases.
Baseline Characteristics of Studied Cases (N = 40).

Abbreviations: Hb, hemoglobin; N, number; WBCs, white blood cells; WHO, World Health Organization; %, percentage..
As regards to bleeding severity (World Health Organization [WHO] bleeding scale); 27 cases (67.5%) suffered from grade 1 bleeding, 10 (25%) suffered from grade 2 bleeding, and 3 (7.5%) suffered from grade 0 bleeding (no bleeding).
Platelets range was 5 to 90 (103/mm3) and mean ± SD was 50.3 ± 25.1, hemoglobin (Hb) range was 7.7 to 14 g/dL and its mean was 10.3
As regards to
The mean level of von Willebrand was (18.1 ± 5.4) in the studied patients and (13.8 ± 2.3) in the control group. The mean level of VCAM was (125.1 ± 42.2).
Comparison between the studied groups regarding age, sex, serum von Willebrand, and VCAM (N = 80) results is shown in Table 2. First, the mean age among cases was equal to 46.2 ± 12.7. The mean age among controls was equal to 42.8 ± 8.2. There were 16 (40%) males and 24 (60%) females among cases but among controls, there were 14 (35%) males and 26 (65%) females. In addition, there is a highly statistically significant difference between case and control as regards to the mean level of von Willebrand. The mean level of von Willebrand was (18.1 ± 5.4) in the studied patients and (13.8 ± 2.3) in the control group. Also from Table 2, there is a statistically significant difference between case and control as regards to mean level of VCAM. The mean level of VCAM was (125.1 ± 42.2) in the studied patients and (102.5 ± 53.3) in the control group.
Comparison Between the Studied Groups Regarding Demographic (Sex, Age), Serum Von Willebrand, and VCAM (N = 80).

Abbreviation: VCAM, vascular cellular adhesion molecule.
Table 3 shows that there was no statistically significant difference between studied patients’ platelets count as regards to age and sex. Patients with platelet counts less than 20 000 had a mean ± SD (43.7 ± 13.95). Patients with platelet count more than or equal to 20 000 had mean ± SD (46.9 ± 12.5). Patients with platelet count less than 20 000 had 4(44.4%) male patients and 5(55.6%) female patients. Patients with platelet count more than or equal to 20 000 showed 12 (38.7%) male patients and 19 (61.3%) female patients.
Baseline Characteristics of Cases According to Severity of Thrombocytopenia (N = 40).
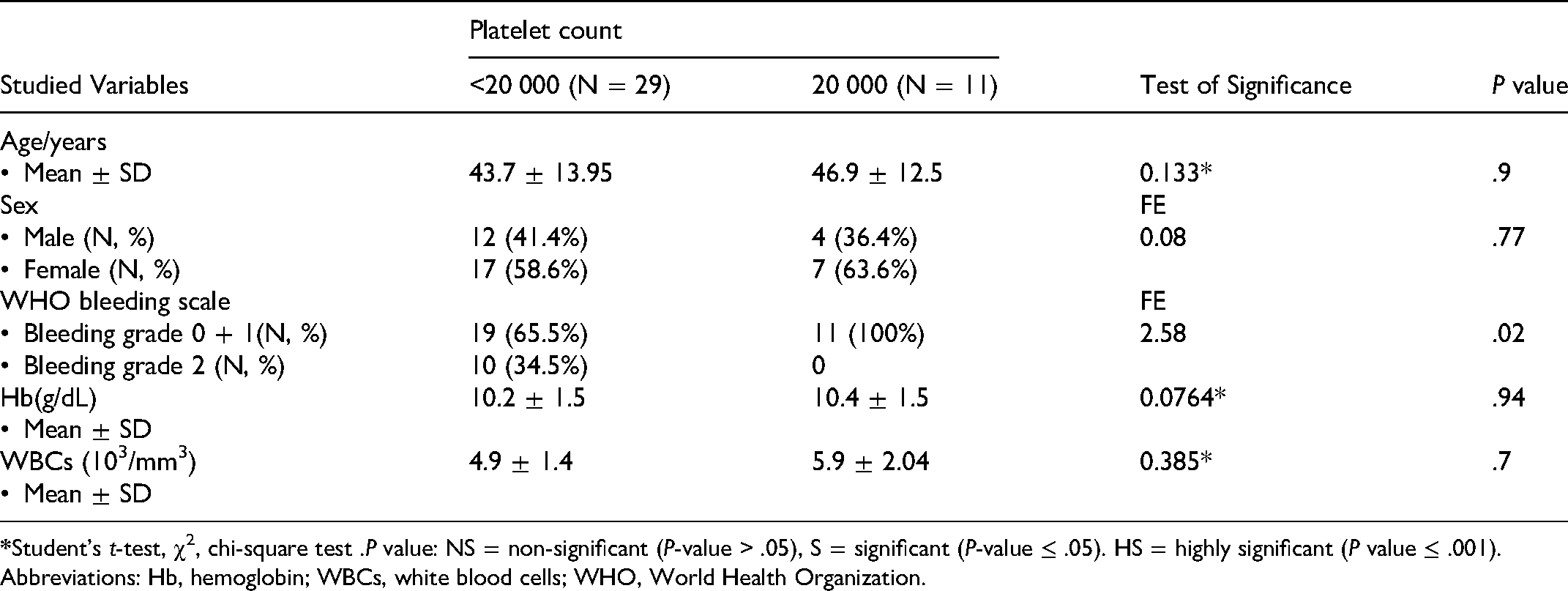
Abbreviations: Hb, hemoglobin; WBCs, white blood cells; WHO, World Health Organization.
There was a statistically significant difference between studied patients’ platelet counts as regards to WHO bleeding scale. Patients in the group of platelet count less than 20 000 were 19 (65.5%) patients with bleeding grade 0 + 1 and 10 (34.5%) were of patients with bleeding grade 2. Patients in the group of platelet count more than or equal 20 000 were 11 (100%) with bleeding grade 0 + 1 and there were no patients with bleeding grade 2.
There was no statistically significant difference between the two groups of platelets count as regards to mean of Hb and WBCs. Mean hemoglobin concentration in group of patients with platelet count less than 20 000 was 10.2 ± 1.5 g/dL and WBCs were 4.9 ± 1.4 (103/mm3). Mean hemoglobin concentration in group of patients with platelet count more than or equal 20 000 was 10.4 ± 1.5 g/dL and WBCs were 5.9 ± 2.04 (103/mm3).
There was no statistically significant correlation between von Willebrand and laboratory parameters of the studied patients (P value > .05). The correlation coefficient (
Correlation Coefficient (r) Between von Willebrand and Laboratory Parameters of the Studied Patients (N = 40).

*Spearman's correlation coefficient.
Abbreviations: Hb, hemoglobin; VCAM, vascular cellular adhesion molecule; WBCs, white blood cells.
Table 5 shows that there was no statistically significant correlation between VCAM and laboratory parameters of the studied patients (P value > .05). The correlation coefficient (
Correlation Coefficient (r) Between VCAM and Laboratory Parameters of the Studied Patients (N = 40).

*Spearman’s correlation coefficient.
Abbreviations: Hb, hemoglobin; VCAM, vascular cellular adhesion molecule; WBCs, white blood cells.
Discussion
Severe thrombocytopenia can result in fatal bleeding. Surprisingly, there is great variability in bleeding manifestations in thrombocytopenic patients, suggesting that factors other than platelet count determine the phenotype. While platelets play a pivotal role in the formation of hemostatic clots at the sites of vascular injury, petechial hemorrhages and capillary leakage also occur with thrombocytopenia in the absence of vascular injury. The fact that bleeding can occur without vascular injury has led to the idea that platelets support the vascular endothelium and maintain the structural integrity of intact blood vessels. 9
ECs had not been previously considered as a key component of the immune system; however, there are growing pieces of evidence that show the involvement and modulation of these cells through innate and adaptive immune responses. EC activation and perturbation have been associated with different immunopathological processes, such as atherosclerosis, diabetes, pulmonary hypertension, rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), hemoglobinopathies, and certain infectious diseases like dengue, among others. 11
One of the main functions attributed to the endothelium in the context of the immune responses is leukocyte transmigration from the vascular lumen to the tissues; this is a determinant event for the initiation and resolution of different inflammatory processes which involves the contribution of a variety of adhesion molecules that mediate their direct interaction with ECs, such as lectins CD62P and CD62E and the glycoproteins ICAM-1, ICAM-2, VCAM-1, and CD99. 12
The binding of platelets to the endothelium facilitates EC activation and thus aids the endothelium in taking on a proinflammatory function. Endothelial-bound platelets become activated and liberate numerous proinflammatory cytokines and generation of reactive oxygen species, enhanced expression of matrix metalloproteinases, and expression of adhesion molecules such as ICAM-1, VCAM-1, and E-selectin. 13
vWF behaves as an extracellular adapter molecule, linking platelets to the extracellular matrix at sites of vascular injury. These interactions are crucial for hemostasis. Too little platelet adhesion causes bleeding which is typical of von Willebrand disease, whereas too much platelet adhesion may cause thrombotic thrombocytopenic purpura. Mutations in VWF or platelet glycoprotein Ib can either reduce or increase the affinity of platelet binding. Paradoxically, affinity changes in either direction cause bleeding 14
ITP is an autoimmune disorder characterized by increased platelet destruction and/or decreased platelet production. In addition to risks of bleeding, an increased risk of thrombosis has been identified, despite low platelet counts. The reasons behind this remain unclear.
In the same study, they investigated whether inflammatory mediators associated with the acute disease could play a role. CRP levels were elevated in many patients with ITP, but this did not correlate with VWF levels.
Using the correlation analysis and the linear regression, there was no statistically significant correlation between von Willebrand and VCAM with the laboratory parameters of the studied patients.
In the current study, we didn’t find any statistically significant difference between studied cases and controls as regards to age, sex, and routine laboratory data. ITP patients showed female predominance with a peak in reproductive years. We aimed to examine the near percentage of age, sex, and clinical data in both the studied cases and controls to decrease any differences that could affect the result.
In agreement with
Bleeding events are often unpredictable, and patients with ITP, even in the setting of severe thrombocytopenia, may not exhibit bleeding beyond bruising and petechiae. However, more serious mucosal bleeding may occur, including menorrhagia, epistaxis, gastrointestinal hemorrhage, hematuria, or, rarely, intracranial hemorrhage (ICH). There is a study demonstrated that ICH has been reported in 1.4% of adults and 0.1% to 0.4% of children with ITP. Severe bleeding is reported in 9.5% of adults and 20.2% of children. Adults with ITP have a 1.3- to 2.2-fold higher mortality than the general population due to cardiovascular disease, infection, and bleeding. 18
In our study, some studied cases suffered from low Hb which is mostly due to bleeding and low platelets, but our controls have no bleeding.
The study of
In this study, there was no statistically significant difference between studied patients’ platelets count as regards to age and sex which was demonstrated also in the study of
There was no statistically significant difference between studied patients’ platelet counts as regards to Hb and WBCs.
There was a statistically significant difference between studied patients’ platelet count as regards to WHO bleeding scale. This is in agreement with
In agreement with
There is a highly statistically significant difference between case and control as regards to mean level of PC and INR.
This is the first study on the relation between endothelial activation biomarkers (VCAM-1 and vWF) in naive adult ITP patients.
Our study revealed that there was a highly statistically significant difference between Case and Control as regards to mean level of von-Willebrand and a statistically significant difference between Case and Control as regards to mean level of VCAM.
A very interesting study
Endothelial dysfunction has been increasingly recognized in patients with SLE over the past two decades or so. In a Case–Control study by
In a study by
Limitations
The small number of the studied immune thrombocytopenia ITP patients in our work, as from the inclusion criteria we selected newly diagnosed naïve patients only which were limited by that duration.
Detection of vWF and V-CAM only once at diagnosis and it was not repeated after a while of follow-up or after treatment to take a real-time follow-up of it, so we recommend to do this sequential follow up serum level detection to them in future studies.
Conclusion
This pilot observational study depicted the possible association between endothelial activation and ITP, a relationship which needs to be challenged by further large-scale studies with a larger No. of patients with persistent and chronic ITP in addition to comparing it with the newly diagnosed ITP patients. We had taken only limited prototypes of markers, but we recommend other studies in more depth for assessing coagulation proteins, fibrin, inflammatory proteins, and albumin roles on endothelial activation.
Footnotes
Author’s Contributions
Alaa Efat and Walaa Elgheriany wrote the manuscript and analyzed the data. Aida Nazir and Essam Abdelmohsen performed data collection and manuscript preparation. Hanan Bedair and Ashraf Dawood performed the laboratory study. Sabry Shoeib was responsible for the selection and follow-up of patients. All the authors revised the study and reviewed the article.
Data Availability
Data are available upon request by contacting the corresponding author (Dr Alaa Efat).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.