
Abstract
Introduction
Thrombo-inflammatory biomarkers play an important role in the pathogenesis of lymphoma. We aimed to characterize the interrelationship of thrombo-inflammatory biomarkers and blood cellular indices in lymphoma patients.
Materials and Methods
Ninety-eight lymphoma patient samples were collected from Lymphoma Center of Clinic of Hematology, University of Belgrade, Serbia. Normal controls (n = 50) represented plasma from healthy individuals. Plasminogen activator inhibitor (PAI-1), D-Dimer, factor XIII, C-reactive protein (CRP), microparticles (Mp), Von Willebrand factor (vWF), total protein S, urokinase-type plasminogen activator (uPA), tumor necrosis factor (TNFα), β2-glycoprotein I (β2GPI), and fibronectin levels were measured utilizing commercially-available ELISA methods. Thrombin generation profile (TGA) was measured using a fluorometric kinetic assay. Platelets, leukocytes, lymphocytes, and neutrophils were measured in conjunction with the complete blood profile.
Results
Statistically significant differences were noted in levels of PAI-1, D-Dimer, factor XIII, CRP, microparticles, vWF, uPA, TNFα, β2GPI, fibronectin, and TGA when compared to normal (all P values < .001). Platelet to leukocyte ratio (PLA) correlated to TNFα and fibronectin (R = −0.31 and −0.53, respectively) and the platelet to neutrophil ratio (PNR) correlated to factor XIII and β2GPI (R = 0.40 and 0.40, respectively).
Conclusion
Plasma samples from lymphoma patients demonstrated a significantly altered thrombo-inflammatory biomarker profile that has notable correlations to blood cellular indices.
Introduction
Lymphomas compose a group of hematogenous malignancies of lymphocytic origin and represent approximately 5% of all malignancies in the US. 1 Despite widespread impact, the etiology of most lymphomas has yet to be clearly elucidated, however, various risk factors, such as the thrombo-inflammatory profile of the tumor's microenvironment, have been strongly implicated in mediating both tumor pathogenicity and disease progression due to downstream effects on immune function.2,3 As a result of the actions of various thrombo-inflammatory biomarkers, both the activation of proto-oncogenes and inactivation of tumor suppressor genes have been observed and suspected of leading to lymphoma progression. 4
It has previously been established that elevated levels of thrombo-inflammatory biomarkers are associated with lymphoma and play a role in not only the induction of a hyper-coagulable state, but also in the generation of prognostic scores and models.5,6 In addition, increased complication rate and disease severity risk associated with such hemostatic perturbations in the lymphoma population have been supported through the association of lymphoma risk and biomarker genetic polymorphisms. 7 Indeed, in analyzing circulating levels of C-reactive protein (CRP), von Willebrand factor (vWF), fibrinogen, phospholipase A2, and factor VIII in lymphoma patients, Menschikowski et al. found patients with elevated levels to have a statistically reduced survival time. 8
Several other groups have come across similar findings in their studies and generated powerful prognostic information solely utilizing circulating levels of thrombo-inflammatory biomarkers in various lymphoma populations.9-12 Despite these findings, a thorough prognostic model remains yet to be developed due to various limiting factors in previous studies such as variety of biomarkers studies, population specificities, and a lack of blood cellular indices. Thus, thrombo-inflammatory biomarker profiles composed of a broader range of molecules and their correlating blood cellular indices are needed in order to more fully elucidate and utilize the potential prognostic value of serological lymphoma assays.
In this study, we present findings composed of 98 test and 50 control subjects designed to investigate whether plasma circulating levels of 12 thrombo-inflammatory biomarkers (PAI-1, D-Dimer, factor XIIIa, CRP, Mp, vWF, total protein S, uPA, TNF, β2GPI, fibronectin, and TGA) and their corresponding blood cellular indices (neutrophil to lymphocyte ratio [NLR], platelet to neutrophil [PNR], platelet to leukocyte ratio [PLA] and platelet to lymphocyte ratios [PLR]) are associated with a lymphoma diagnosis.
Patients and Methods
Study Design
In this retrospective study, plasma samples of lymphoma patients were used to investigate the relationship between thromboinflammatory biomarkers and blood cellular indices of inflammation in lymphoma patients with respect to healthy controls.
Patients’ demographic information was collected in addition to lymphoma and malignancy characteristics and categorizes appropriately. Plasma analytes consisted of citrated blood samples from 98 patients with histologically confirmed diagnosis of non-Hodgkin lymphoma (NHL), Hodgkin lymphoma (HL) and Chronic lymphocytic leukemia/Small lymphocytic lymphoma (CLL/SLL). Samples were collected under the IRB approved protocol from the Clinic of Hematology Unit, University of Belgrade, Belgrade, Serbia. Eligibility Criteria included availability of plasma sample, consent to biochemical studies, and diagnosis of histologically confirmed lymphoma. Control measurements were generated by analyzing normal human plasma (NHP) of 25 male and 25 female samples which were obtained from a commercial source (George King Biomedical, Overland park, KS, US.). Normal human pooled plasma was used for referencing purposes.
Laboratory Assays
A fluorogenic substrate method for thrombin generation was used which employed a Fluoroskan Ascent fluorimeter, calibrated automated thrombogram from Diagnostica Stago (Parsippany, NJ, US). Reagents used in this assay included the fluo-substrate, fluo-buffer, tissue factor high reagent (mixture of tissue factor and phospholipids) and a thrombin calibrator. The tissue factor activator used in this study was a recombinant version which is commercially available. The thrombin generation assay was carried out in 96-well Immulon 2HB transparent round bottom plates. Thrombin generation potential was measured in terms of the peak thrombin concentration, lag time, and endogenous thrombin potential (ETP)/area under the curve (AUC). % peak thrombin and % endogenous thrombin potential were calculated.
Quantification of thrombo-inflammatory biomarker levels, such as PAI-1, D-Dimer, factor XIIIa, CRP, Mp, vWF, total protein S, uPA, TNF, β2GPI, and fibronectin, was performed utilizing commercially-available and clinically-approved sandwich ELISA kits by Aniara Diagnostica (West Chester, Ohio, USA), utilizing a SpectraMax plus 384 microplate reader (Molecular Devices, CA, USA) set at 450 nm, as recommended by the manufacturer.
Statistical Analyses
Demographical data were analyzed via descriptive statistics. Blood cellular indices, such as NLR, PNR, PLA, and PLR, were calculated in conjunction with the patients’ complete blood profile via Coulter counter via simple ration generation.
GraphPad Prism software was used in performing statistical analyses, such as one-way ANOVA, Pearson's correlation coefficient, Sidak's multiple comparisons, and calculation of means and standard error of the mean. All conducted statistical analyses were 2-sided with an α of .05.
Results
Patient Demographics
The demographical data of the enrolled patients are summarized in Table 1. Participants were an average of 56.8 ± 12.7 years old at time of initial diagnosis and composed of a relative even split of males (57.1%) and females (42.9%). Within the broader category of lymphoma, the most common histologic subtypes were aggressive Non-Hodgkin Lymphoma (46.9%, NHL), small lymphocytic lymphoma (23.5%, SLL), indolent NHL (17.3%), and Hodgkin Lymphoma (9%).
Participant Demographic Data.
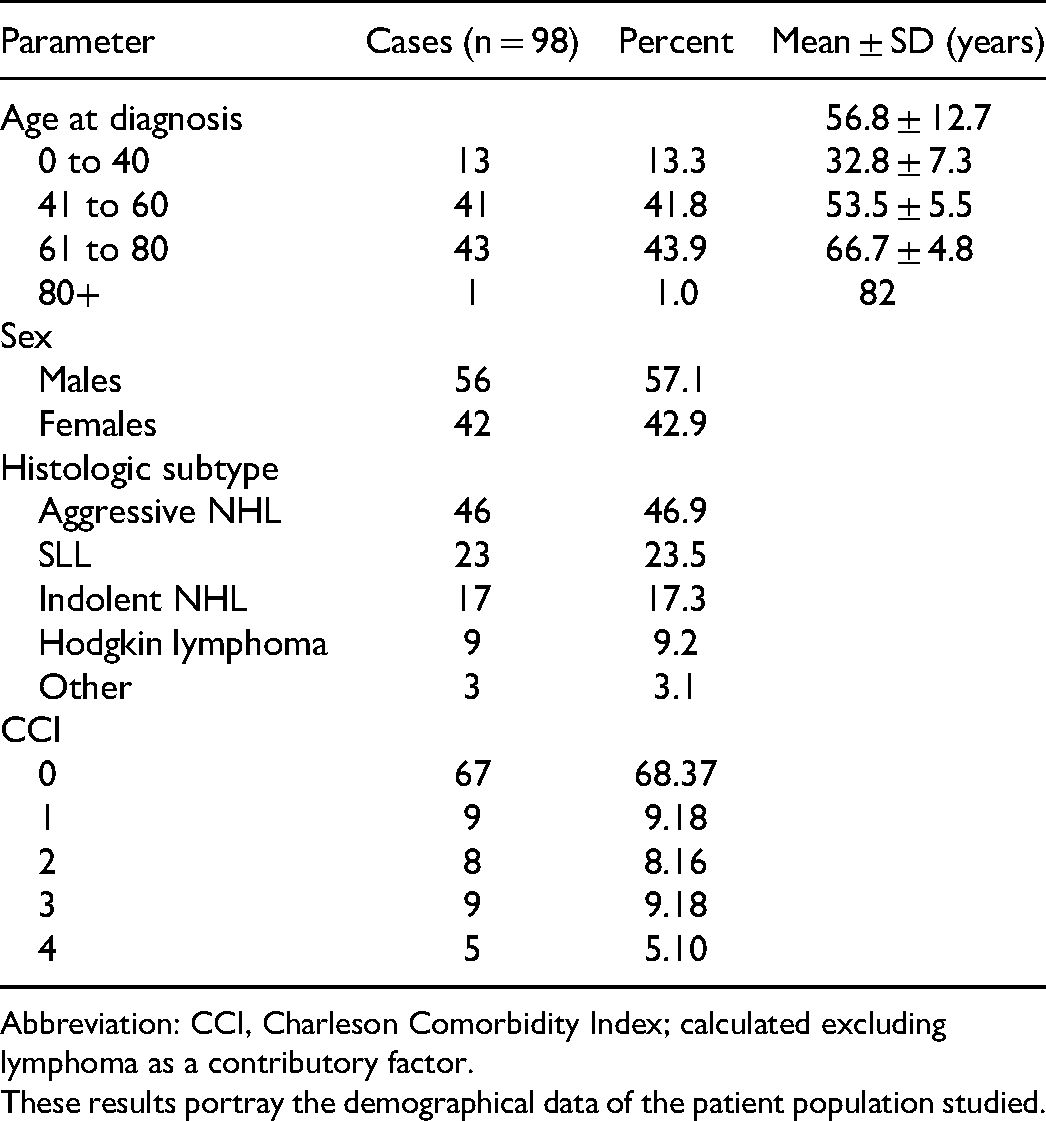
Abbreviation: CCI, Charleson Comorbidity Index; calculated excluding lymphoma as a contributory factor.
These results portray the demographical data of the patient population studied.
Circulating Thrombo-Inflammatory Biomarker Levels
Thrombo-inflammatory biomarker values of percent change from normal values were calculated as 103.74% (PAI-1), 350.53% (D-Dimer), −43.42% (factor XIIIa), 2442.64% (CRP), −38.84% (Mp), 267.38% (vWF), −4.61% (total protein S), −27.86% (uPA), 740.84% (TNFα), −4.04% (β2GPI), −51.48% (fibronectin), and −58.10% (TGA). Figure 1 depicts Tukey box and whisker plots for individual biomarkers in terms of percent change in lymphoma patients compared to normal. Table 2 shows the composite results these in terms of Mean ± 1 standard deviation of 98 lymphoma patients and 50 normal plasma samples. The percent change values indicate the relative change of the biomarkers in comparison to the normal.
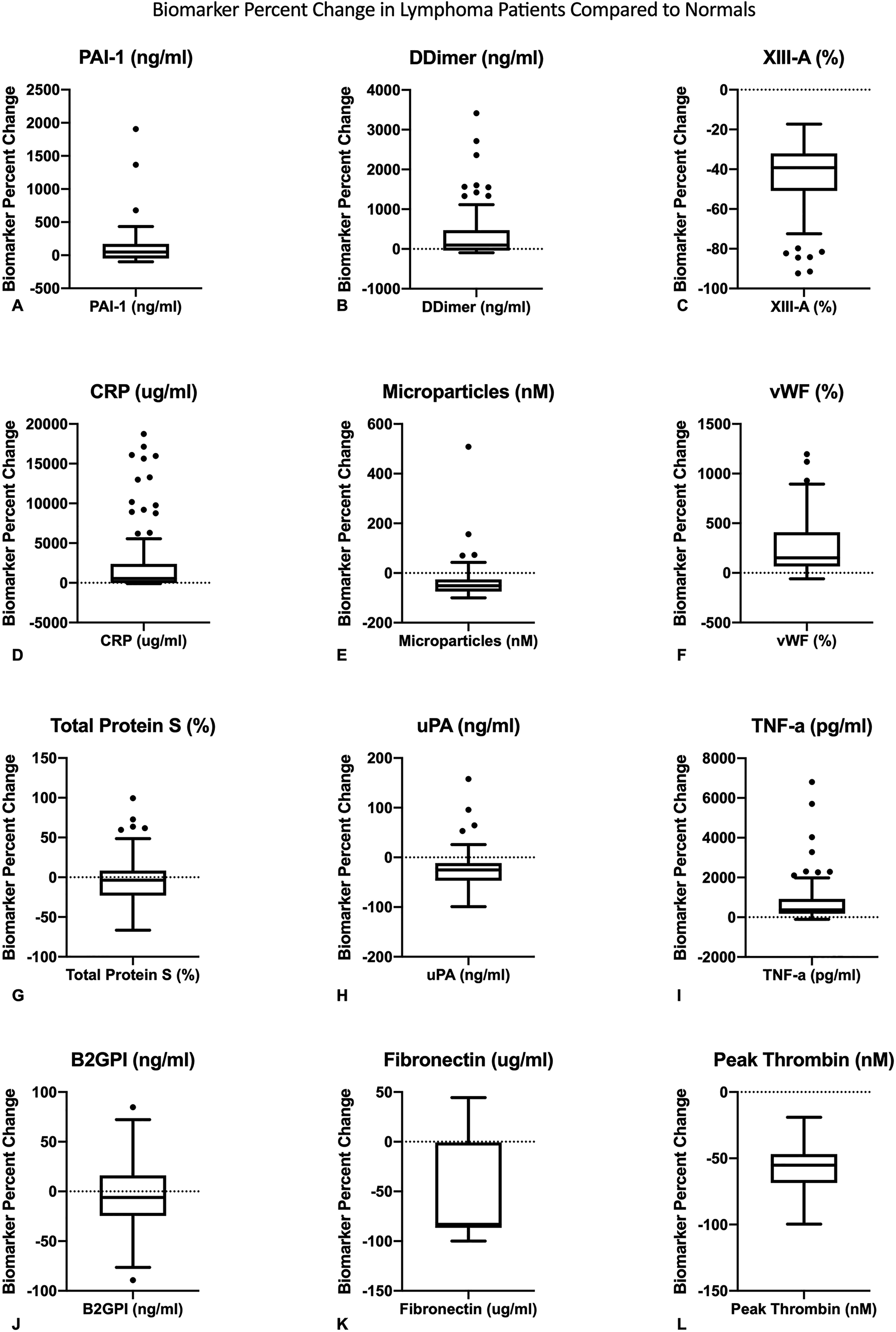
Tukey box and whisker plots of thrombo-inflammatory biomarker percent change values in lymphoma patients (A-L).
Distribution of Thrombo-inflammatory Biomarker in Normal and Lymphoma Patients.

These results represent Mean ± standard deviation of 98 lymphoma patients and 50 normal plasma samples. The percent change values indicate the relative change of the biomarkers in comparison to the normal.
As shown in Table 2, Sidak's multiple comparisons test demonstrated statistical significance in the differences of D-Dimer, factor XIIIa, CRP, vWF, TNFα, and TGA levels between lymphoma patients and normal (all P values ≤ .001).
Blood Cellular Indices Compared to Thrombo-Inflammatory Biomarker
Measured blood cellular parameters were found to be 234.32 ± 131.50 × 109/L (platelets), 32.34 ± 58.31 × 109/L (leukocytes), 21.17 ± 8.40 × 109/L (neutrophils), and 6.93 ± 7.49 × 109/L (lymphocytes) with calculated percent change values of −14.79%, 361.95%, 30.94%, and −28.60%, respectively. Platelet to leukocyte ratio (PLA), PLR, PNR, and NLR values of 28.98 ± 23.11, 21.09 ± 28.53, 4.52 ± 2.19, and 4.68 ± 5.18, respectively, were generated.
Table 3 shows the relationship between thrombo-inflammatory biomarker levels and blood cellular indices. Pearson product-moment correlation coefficients suggested an interrelationship between PLA and TNFα and fibronectin (R values = −0.31 and −0.53, respectively) and PNR and factor XIII and B2GPI (R values = 0.40 and 0.40, respectively).
Blood Cellular Indices and Biomarker Correlations in Lymphoma Patients.
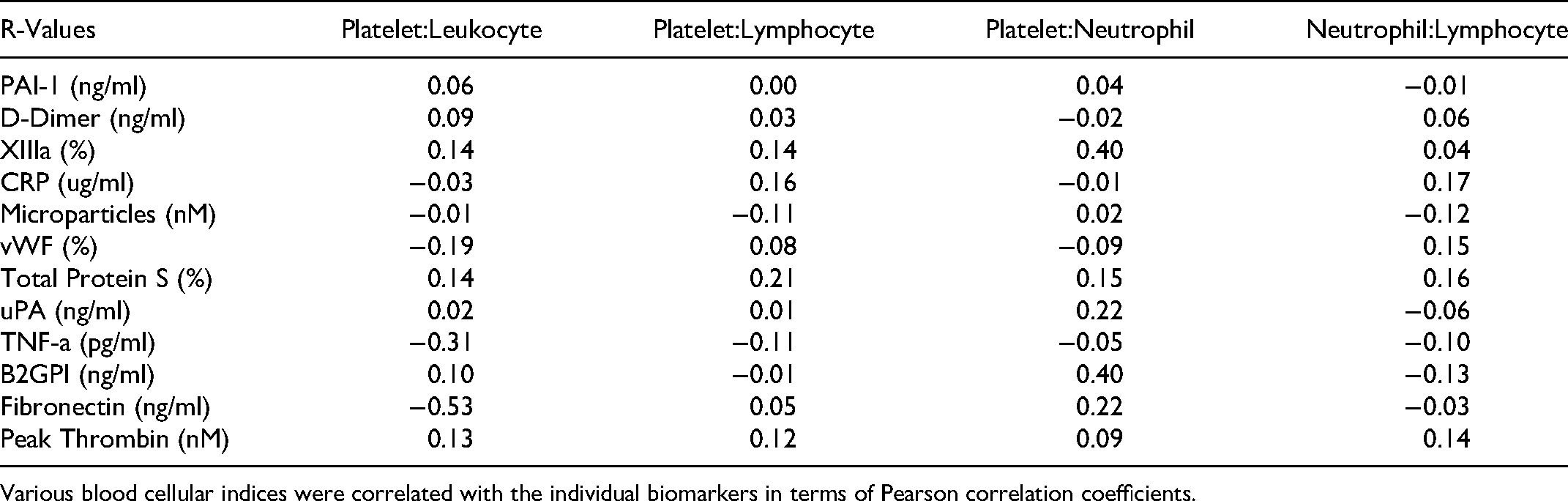
Various blood cellular indices were correlated with the individual biomarkers in terms of Pearson correlation coefficients.
Discussion
Thrombo-Inflammatory Biomarkers
While the lymphoma subgroup of this malignancy represents a large and heterogeneous class of cancers with varying presentations and degrees of aggressiveness, its propensity for eliciting a hypercoagulable state has been repeatedly demonstrated as a unifying factor.13-16 To further elucidate the lymphoma thrombo-inflammatory microenvironment, we analyzed the interrelationships between not only multiple biomarkers, but also various blood cellular indices in order to generate a more holistic lymphoma inflammatory and hypercoagulable profile. In a Serbian population of lymphoma patients, data showed thrombo-inflammatory variations in the form of elevated plasma values of D-Dimer, CRP, vWF, TNFα, neutrophils, and leukocytes and decreased values of factor XIII, platelets, and lymphocytes, overall suggesting a predominantly thrombotic state. Interestingly, the thrombin generation parameters were reduced in the lymphoma cohort, presumably due to the ongoing progressive consumption of coagulation factors due to hypercoagulable state, resulting in this observed change.
The thrombotic component of the overall plasma biomarker profile has previously been extensively documented and our results suggest similar tumor microenvironment characteristics.17-19 D-Dimer values were elevated by 350.53% and had a mean value of 868.62 ± 1197.47 ng/mL, suggesting both a much higher mortality risk per double increase of D-dimer levels (1.5 hazard ratio, P = .001) and a 22% chance of developing a venous thromboembolism (VTE) over a period of 6 months (P = .0033).20,21
Similarly, elevated levels of CRP, a major biomarker of inflammation, also contribute to the thrombo-inflammatory nature of lymphoma as shown in previous studies and reaffirmed in the current study (mean = 16.02 ± 27.61 µg/mL). 5 As a common endpoint in the mechanistic actions of pro-inflammatory cytokines such as interleukin-1 and TNFα, CRP has been implicated in playing a major role in the poor prognosis and systemic inflammatory response associated with lymphoma.22,23 Furthermore, multivariate analysis of CRP values ≥ 10 µg/mL were found to be independently associated with a significantly reduced overall survival (OS) (relative risk = 1.952, P = .012). 5 Lymphoma patients are susceptible to infections due to their immuno-compromised status and it is likely that, in this lymphoma cohort, some of these patients have subclinical infection which may have contributed to the elevated levels of CRP.
In regard to TNFα, a key endogenous factor and major inflammatory cytokine, substantial evidence has been generated implicating its expression with extensive and pronounced contribution to the lymphoma-associated thrombo-inflammatory state, poor prognosis, and reduced progression-free survival.3,24 In the Serbian cohort, TNFα expression was markedly increased in comparison to the control group (740% ± 1085.28%), suggesting a sizable contribution to the pro-inflammatory state of lymphoma by TNFα. However, levels of TNFα in lymphoma have been associated with a broad spectrum of tumoral effects ranging from neoplasm regression to metastasis promotion.3,25,26
A key coagulation mediator and marker of thrombosis, vWF, serves a crucial role in hemostasis and, in the pathogenic state, has been shown to directly promote thrombotic processes that contribute to arterial and venous thrombosis risk.27,28 Indeed, in a prospective study of 19 237 individuals with a median follow-up of 7.8 years, values of vWF ≥ 204% activity demonstrated a hazard ratio of 7.6 for developing VTE. 29 Comparatively, this study's cohort demonstrated a mean vWF percent activity of 260.51 ± 197.62, further potentiating the pathogenic involvement of vWF in both promoting and maintaining a thrombo-inflammatory state.
Regarding the thrombin generation parameters, peak thrombin concentration was found to be lower (113.71 ± 53.40 nM) in the lymphoma cohort compared to healthy individuals (271.4 nM). This is inconsistent with a previously reported healthy cohort, with a much higher mean of 271.4 nM. 30 The increase in various biomarkers of thrombin generation and a decreased generation of thrombin in lymphoma patients are consistent with previously established findings which indicated the lymphoma tumor microenvironment is associated with mediators of thrombosis with a decreased thrombogenesis. 31 In addition, increased thrombin has also extensively been associated with the propagation of both tumor growth and metastasis. 32
With respect to factor XIIIa, this study's cohort demonstrated a mean percent activity of 87.95 ± 25.68 compared to normals’ mean percent activity of 155.44 ± 48.07 (−43.42 ± 16.52% change, P < .0001). Conventionally, a decrease in plasma factor XIIIa suggests a quantitative biomarker dynamics deviation towards hypocoagulability, i.e a reduced potential for the stabilization of fibrins in the final step of the coagulation pathway; however, factor XIIIa deficiency classification is not met until percent activity declines to less than 1%.33,34 Thus, despite significant differences among the two groups, the relatively preserved percent activity of factor XIIIa within the lymphoma group suggests adequate clot stabilization potential, however, there is an inherent lack in previous studies which have explored this phenomenon in lymphoma patients. Limited data generated by Adany et al. suggested tumor-associated macrophages containing factor XIII to exist as a non-homogeneous population with varying protein expressivity. 35
Blood Cellular Indices
To further determine the thrombo-inflammatory interactions in lymphoma patients, we explored the associations between blood cellular indices ratios and biomarker levels which revealed an inverse relationship between the PLA and TNFα and fibronectin (R values = −0.31 and −0.53, respectively). In accordance with previous findings and the current study, the PLA has been associated with an increased release of pro-inflammatory and coagulation factors.36-39 Notably, the PLA is negatively correlated to the also pro-inflammatory and coagulatory TNFα, however, this seemingly paradoxical relationship likely originates from the notion that consensus regarding TNFα‘s conclusive role in lymphoma has yet to be reached.3,25,26 Additionally, this unexpected inverse relationship is further rationalized by the inherent nature of a reduced platelet count, and thus PLA, in lymphoma and concomitant increase in TNFα expression as demonstrated by the current study. In regards to the inverse relationship between PLA and fibronectin, previous studies have demonstrated high fibronectin expression with an increased OS (6.3 years vs 3.6 years, P = .05), thus generating the result of the current study. 40
The interplay between the PNR and factor XIII and β2GPI (R values = 0.40 and 0.40, respectively) are supported by the related mechanisms each component participates in throughout the pro-inflammatory and coagulant cascade. 41 More specifically, the positive correlation between the PNR and factor XIIIa is corroborated through the positive associations between an increasing platelet count, and thus PNR, with an increase in thrombotic state and subsequent clot-stabilizing action of factor XIIIa.42,43 Furthermore, the positive correlation between the PNR and its thrombo-inflammatory nature and the pro-coagulant properties of β2GPI, although still not fully understood, have been upheld by several groups; indeed, in addition to its plasminogen activating abilities, β2GPI has been shown to propagate the thrombotic cascade via indirect inhibition of protein C activation and interruption of anticoagulant Annexin V shield as well as directly interfering with thrombomodulin function.44-46
Study Parameters
In designating the limitations and criteria of the various parameters assessed throughout this study, we aimed to strike a balance between exceeding the limitations of previously published works and maintaining overall feasibility. Consequently, while this study more holistically integrates different aspects of the thrombo-inflammatory state of lymphoma patients than previous works, subsequent to financial, temporal, and overall pragmatic boundaries, inherent limitations exist which confine the generality and scope of the current study.
We intended to assess the lymphoma thrombo-inflammatory state circulating biomarker levels in conjunction with blood cellular indices of inflammation using a more comprehensive and inclusive approach than previously done. This combinatorial approach allowed us to more aptly dissect the components responsible for the lymphoma thrombo-inflammatory state than previous studies which incurred limitations such as fewer biomarkers, limited blood cellular indices, a smaller patient population, or a combination thereof.8,47-52 We believe the integration of parameters set within our design allowed us to more thoroughly depict the lymphoma state such that we were able to both uncover thrombo-inflammatory links within blood plasma measurements in lymphoma patients and further solidify the basis for future studies.
As a consequence of our comprehensive plasma analysis, we encountered various limitations in this study. Similar to the barriers reported by other groups, our study encountered marked variance within many measurements due to the limited sample size.53-56 From a demographic standpoint, the lymphoma cohort was older than the control group, which is due to the fact that control plasma samples were obtained from a commercial source. An age-match control group with other balanced parameters is more appropriate for such a comparison which should be considered for future studies. Additionally, the high variance observed within our samples is, moreover, due to the heterogeneity of lymphoma sub-types observed in this cohort which consisted of both Hodgkin's and non-Hodgkin's lymphoma. In addition, with the ever-growing list of markers involved in the inflammatory process, our relatively inclusive list of 12 biomarkers is, in reality, limited based on current technological abilities and, in comparison to select previous studies, would benefit from expansion. 47
Conclusion
In conclusion, the overall relationship between thrombo-inflammatory biomarkers and blood cellular indices of inflammation in lymphoma patients is composed of many dynamic components, several of which partake in multiple processes. In comparison to normals, the thrombo-inflammatory biomarker profile and blood cellular indices in lymphoma patients demonstrated a close interrelationship which functioned to highlight the significant plasma alterations observed. These findings warrant further clinical outcome analysis in a larger, stratified lymphoma population cohort.
Footnotes
Acknowledgments
The authors would like to acknowledge the faculty of The Hemostasis and Thrombosis Research Unit, Loyola University Health Science Division. In addition, we thoroughly appreciated the efforts put forth by the nursing and laboratory staff of the lymphoma center, University of Belgrade, Belgrade Serbia. Dr Paul Riley, of Diagnostica Stago (Paris, France), is gratefully acknowledged for generously providing us with the instrument and reagents for the thrombin generation studies. We also acknowledge the support of Dr Eva Wojcik, Chairperson, Department of Pathology and Laboratory Medicine. Finally, the authors acknowledge the guidance and support of vice provost of research, Dr Meharvan Singh, for enhancing the research program for students at Loyola University.
Author Contributions
(I) Conception and design: All authors. (II) Administrative support: Darko Antic, MD, PhD, Debra Hoppensteadt, PhD, and Jawed Fareed, PhD. (III) Provision of study materials or patients: All authors. (IV) Collection and assembly of data: MD, Mark Jaradeh, BS, Nausheen Baig, BA, Darko Antic, MD, PhD. (V) Data analysis and interpretation: Mark Jaradeh, BS, Nausheen Baig, BA. (VI) Manuscript writing: All authors. (VII) Final approval of manuscript: All authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by institutional review board of Loyola University Medical Center (NO.211663: the registration number of ethics board) and individual consent for this retrospective analysis was waived.