
Abstract
Several lines of evidence have suggested a sustainable relationship between blood viscosity (BV) and deep vein thrombosis (DVT). But there was a lack of data on the association of preoperative BV and postoperative acute DVT. For patients who accepted total knee arthroplasty (TKA) caused by primary knee osteoarthritis (KOA), this study tried to investigate whether preoperative BV relevant parameters might affect DVT risk following TKA. We reviewed a total of 750 consecutive KOA patients treated by unilateral TKA in our hospital from March 2010 to May 2020. All patients undergoing TKA were routinely examined by the color Doppler ultrasound on the third postoperative day and were assigned into DVT and non-DVT groups. Statistical comparisons of BV relevant parameters which mainly including whole BV (low, midst, and high shear rates), plasma viscosity, whole blood reductive viscosity (BRV; low, midst, and high shear rates) were made comprehensively. It could be found that low whole BRV (low shear rate) before TKA was significantly related to postoperative DVT risk in all patients, especially in female patients after stratifying by gender (p < .05). Our results implied that low whole BRV might be a remarkable risk factor of DVT in primary KOA patients after TKA. Timely and effective DVT prophylaxis for these patients is much required.
Introduction
Osteoarthritis (OA) is a highly prevalent chronic degenerative joint disease, which usually causes joint pain and mobility difficulties. 1 Knee joint is the most common site of OA and knee osteoarthritis (KOA) is gradually becoming an important disabling disease. 2 However, there is no effective pharmacologic therapy for KOA except the application of some kinds of nonsteroidal anti-inflammatory drugs and joint arthroplasty surgery. 3 Acted as a major manifestation of venous thrombus embolism (VTE), deep vein thrombosis (DVT) is well known as one of the most severe complications in patients undergoing total knee arthroplasty (TKA) and the incidence rate of which ranged from about 18.1% to 48.6% without thromboprophylaxis in Asian patients. 4 Importantly, DVT can lead to pulmonary embolism and eventually death. 5 Taking into account the preventive anticoagulation strategies after TKA in some existing guidelines, 6 finding some potential biomarkers of a certain sensitivity or specificity such as the D-dimer 7 which can partly predict DVT will be beneficial to DVT prevention.
A triad of blood hypercoagulability, venous stasis, and vessel wall injury has historically been considered to predispose DVT. 8 It was worth mention that DVT risk factors include thrombophilic, circumstantial, and cardiovascular factors. 5 Among them, some evident factors have been confirmed to be associated with hemorheological changes such as increased blood or plasma viscosity (PV). 9 Therefore, hemorheological biomarkers might be playing underlying roles in the onset, development, and outcome of DVT. Previously, it has been demonstrated that patients in the acute phase of DVT showed higher PV, red blood cells (RBCs) aggregation, and whole blood viscosity (BV) than controls. 10 In current times, considering the relatively large number of end-stage KOA patients and a lack of studies focusing on the correlation of preoperative BV relevant parameters and postoperative acute DVT, we firstly attempted to illustrated the exact association of preoperative whole BV (low, midst, and high shear), PV, whole blood reductive viscosity (BRV; low, midst, and high shear) and DVT risk following TKA.
Materials and Methods
Participants
From March 2010 and May 2020, a total of 750 KOA patients (144 males and 606 females) who underwent TKA in our department were consecutively enrolled from a plenty of more than 1600 patients according to the exclusion criteria. 9 Patients planning to undergo bilateral TKAs and those who have rheumatoid arthritis, immune system-related disease, congenital or acquired coagulopathy, hemorheological disorders, preoperative use of anticoagulant therapy, previous operations on the suffered leg within 12 months, the steroids or hormones therapy within the last 3 years, blood transfusion within 12 months, and incomplete data records or partial loss were excluded. This study was approved by the ethical committee of our hospital and each patient needed to sign an informed consent form. Weight and height were uniformly measured by trained nurses on the first day of admission and body mass index (BMI) was subsequently calculated. Some other clinical data including age, gender, and the history of diabetes, hypertension, malignancy, cardiovascular diseases (ie, diseases originate from atherothrombosis including myocardial infract, stable or unstable angina, or stoke), VTE events, steroids or estrogens use, smoking, surgery, and blood transfusion were collected according to patients’ self-report and recorded.
Blood Sample Testing and Surgery
A day after admission, 3 tubes of 5 mL venous blood of each patient were sampled at 7
All TKAs were performed under general anesthesia with the tourniquet. The surgical process of TKA consisted of condylar-type and posterior cruciate substituting cemented arthroplasty via a knee midline skin incision and a deep medial parapatellar approach. The average using time of tourniquet was 40 min during TKA and the entire operation time is generally not exceeding 90 min. A drainage tube was placed in the joint for no more than 48 h. Postoperatively, low molecular weight heparin (LMWH) with a conventional dose (subcutaneous dose of 0.4 mL or 100 IU/kg per day) was applied for DVT prevention every day for each patient and its first-time use was started 10 h after surgery. Patients were requested to do flexion and extension exercises of the lower extremity joints and active muscles contraction at the early time after TKA. For each patient, some relevant symptoms and signs of acute DVT such as redundancy and tenderness in the calf were closely monitored.
DVT Diagnosis and Therapy
On the third day postoperatively, ultrasound examination of bilateral lower extremity veins was done in each patient to determine the presence of DVT based on the results from Dong et al 11 : (1) absence of venous flow; (2) complete noncompressibility of the vein; (3) the presence of an echogenic thrombus mass in a normally anechoic vein. The examiner was blinded to the intraoperative procedure and the preoperative hemorheological parameters. The thrombolytic (0.4 mL or 100 IU/kg every 12 h) and anticoagulant doses (0.4 mL or 100 IU/kg every 24 h) LMWH were used for thrombosis treatment and anticoagulation therapy while in hospital, respectively. After discharge, DVT patients continue to take rivaroxaban orally (10 mg per day) and the entire anticoagulant period should be at least 3 months following surgery.
Statistical Analysis
SPSS software version 22.0 was used to do an analysis. The χ2 test was conducted to compare differences in categorical variables. The mean value was presented with standard deviation and the Student's t-test was adopted to make a comparison. Preoperative confounding factors in this study were all adjusted for the multivariate logistic regression analysis. Still, a receiver operating characteristic (ROC) curve was made to evaluate the predictive cutoff value of the potential indicator. For all the tests, differences were considered significant when p < .05.
Results
Baseline Characteristics
In Table 1, there were 176 DVTs in KOA patients and the total incidence of postoperative DVT was 23.5% (176/750). Notably, female patients had a higher DVT incidence (25.1%) than males (16.7%). Through systematically comparing and analyzing, we could find that DVT patients had a higher TC (p = .010) and LDL-C levels (p = .018) and a lower smoking rate (p = .015) than non-DVT patients. In addition, no significant differences were observed in the mean age and BMI, the distributions of gender, diabetes, hypertension, malignancy, cardiovascular diseases, VTE events, steroids or estrogens use, surgery history, and blood transfusion history, blood levels of TG, HDL-C, apo A1, apo B, FIB, and the average D-dimer, platelet count, PT, APTT, and TT (p > .05).
Comparisons of General Characteristics.

Abbreviations: n, number; y, years; M, males; F, females; SD, standard deviation; BMI, body mass index; VTE, venous thrombus embolism; TG, triglycerides; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; apo A1, apolipoprotein A1; apo B, apolipoprotein B; FIB, fibrinogen; PT, prothrombin time; APTT, activated partial thromboplastin time; TT, thrombin time; min, minute; DVT, deep vein thrombosis.
Evaluated by Pearson Chi-square test.
Evaluated by continuous correction test.
General Comparison of BV Relevant Parameters
In Table 2, the analysis of BV relevant parameters showed significant differences in the whole BRV (low shear rate; p = .024) in all the patients, especially in female patients after stratifying by gender (p = .025). In males, there existed no differences in BV relevant parameters between the 2 groups (p > .05).
Comparisons of BV-related Parameters.

Abbreviations: BV, blood viscosity; BRV, blood reductive viscosity; SD, standard deviation; DVT, deep vein thrombosis; PV, plasma viscosity.
Risk Factors of DVT
In Table 3, it could be noted that low whole BRV (low shear rate) was a significant risk factor for postoperative DVT in both all the patients (odds ratio [OR] = .926, 95% confidence interval [CI] = .869-.987, p = .018) and female patients (OR = .911, 95% CI = .847-.979, p = .011) when stratifying by gender after adjustment for age, BMI, coagulation parameters, and all the other confounding factors in the multivariate analysis.
Multivariate Analysis on Associations of BV-related Parameters and DVT Risk.

Abbreviations: BV, blood viscosity; BRV, blood reductive viscosity; SD, standard deviation; OR, odds ratio; CI, confidence interval; DVT, deep vein thrombosis; PV, plasma viscosity; BMI, body mass index.
Odds ratio adjusted for matching factors of gender, age, BMI, and all the confounding factors in this study.
Odds ratio adjusted for matching factors of age, BMI, and all the confounding factors in this study after stratified by gender.
ROC Analysis of BRV
In Figure 1, for all the patients, the area under the curve (AUC) of whole BRV (low shear rate) was greater than that of the other BV relevant parameters to predict postoperative DVT (AUC: .568, 95% CI = .522-.614; p = .007). The cutoff value of 16.140 mPa·s with a sensitivity of 43.2% and a specificity of 72.7%. Also, whole BRV (low shear rate) had a higher AUC in female patients (AUC: .573, 95% CI = .524-.622; p = .007) and the cutoff value was set at 16.135 mPa·s with a sensitivity of 43.6% and a specificity of 76.3%.
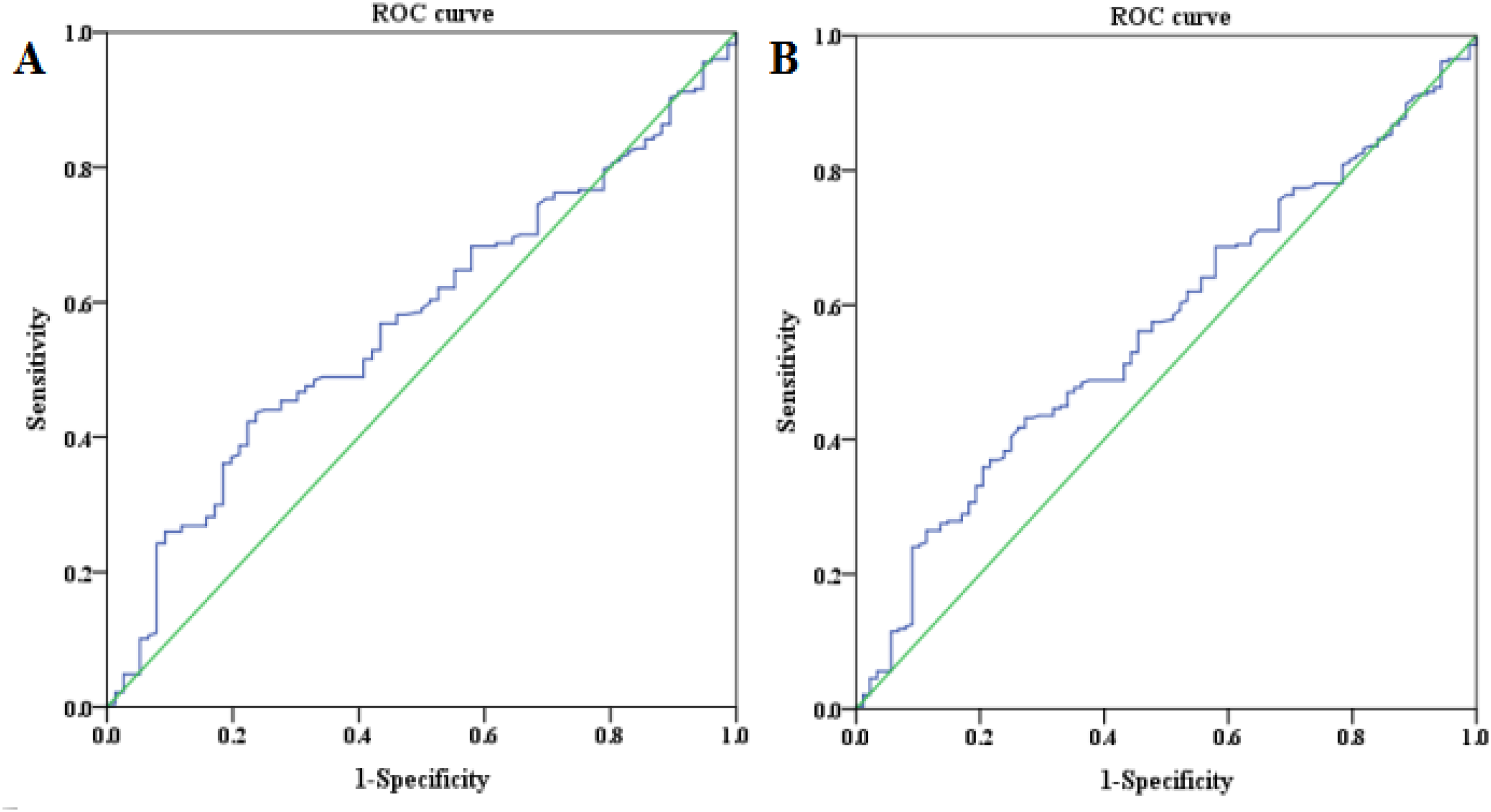
ROC analysis of whole BRV (low shear rate) to predict postoperative DVT in all patients (A) and female patients (B).
Discussion
Taken together, for patients who had primary KOA, our study detailedly assessed the potential association of preoperative BV relevant parameters and postoperative acute DVT risk following TKA with routine anticoagulation of LMWH. We found a statistically significant correlation between the lower whole BRV (low shear) and the increased risk of DVT, especially in female KOA patients. This emerging evidence appeared to support an increasingly larger role of BV in the etiopathogenesis of DVT, which can be considered as a novel finding. Although the AUC of whole BRV (low shear rate) does not seem to have remarkable clinical significance, it can still partially remind us that we need to keep an eye on these patients and make a contribution to DVT prevention by strengthening physical anticoagulation, prolonging anticoagulant time and/or taking some other measures from a different perspective.
In first-time and recurrent DVT patients, hyperviscosity is considered as a kind of classic prothrombotic abnormalities. 12 Intrinsically, VTE is initiated by inflammation and blood stasis, both of which can lead to the generation of thrombi rich in RBCs. 13 RBCs can increase BV and contributes to VTE mainly because of a rise in Hct, an increase in RBCs aggregation, or a decrease in RBCs deformability (increasing flow resistance).13-15 Also, a recent review proposed that RBCs were not only major components of venous thrombi and the determinants of VTE risk, but also actively involved in VTE pathophysiology. 13 Therefore, the potential role played by the alterations of BV relevant parameters results from quantitative and qualitative changes in RBCs in the onset and development of DVT is of considerable importance.5,14 In the clinic, it is noteworthy that our results seem to be inconsistent from the conclusions of previous researches.10,16,17 Different adjusted confounding factors, study populations, tested BV-related biomarkers, shear rates, detection time points, and testing instruments can partly be the explanations. In addition, by a subgroup analysis, the significant association was only existed in female patients might be due in part to the prevalence of KOA in middle and old-aged females.
Previously, it has been expounded that the potential damage to the vessel wall, blood hypercoagulable state after surgery, and the venous stasis because of long-term bed rest are thought to be the 3 main reasons for the formation of postoperative DVT. 18 Combined with our conclusions, it can be speculated that the prothrombotic effects of RBCs in patients with low BRV before surgery may be more likely to be influenced by multiple factors during the surgery, which in turn lead to a relatively large increase in BV that consequently have an imperceptible impact on DVT. In this regard, the change law of BV can provide useful data for the diagnosis, treatment, and prognosis of some arterial vascular diseases. 19 To the authors’ knowledge, few researches have paid attention to the correlation between the specific change rule and/or amplitude of BV-related parameters and DVT. We herein prompted that the rapid increase of BRV may actually affect DVT in such patients and the occurrence of low BRV before surgery can potentially be considered as an implication of thrombophilia. It is plausible that the increased value of the whole BRV may be closely associated with DVT.
Vayá et al have summarized that low blood shear conditions favored red blood cell-cell interactions.5,15 Still, it has been confirmed that RBCs aggregation at low shear increases BV, while at high shear, aggregates are dispersed and BV decreased. 20 In this long-term large-sample retrospective study, related parameters of BV were measured at low, midst, and high shear rates. Nevertheless, we didn't find any other correlations of preoperative whole BV and PV with postoperative DVT, which could be owing to the potential effects on BV exerted by Hct. Since whole BV is linearly related to Hct is the main factor influencing BV,10,21 we firstly try to tested whole BRV and there is reason to believe that the results are of certain reliability and practicality. For all this, it's unignorable that systemic hemorheological alterations maybe not comparable to those in local blood flow areas where minimum disturbances can be more associated with DVT.5,12 A local hemorheological variation may be played a crucial role in DVT formation and confirming the pathogenic importance of locally altered blood rheology in the development of DVT is quite a necessity.
In the past few years, OA has been well recognized as a kind of low-grade inflammatory disease, which is usually accompanied with an elevation in systemic inflammatory factors. 22 Meanwhile, KOA is more common in obese people and obesity is deemed as a low-grade inflammatory disorder as a result of inflammatory cytokines secreted by adipocytes. 23 Notably, there is mounting physiological evidence for the important role of inflammatory biomarkers in thrombogenesis.24,25 Accordingly, it is tempting to demonstrate that the production of inflammatory mediators in these patients may be promoted by TKA surgery itself and then accelerate the formation of DVT via imperceptibly affecting BV. At present, the exact mechanisms linking inflammation and BV remain poorly understood and await clarification, the results of our study may open new perspectives in this field.
For the specific population of KOA patients who needed to undergo TKA, we firstly and systematically analyzed the correlation between BV-related indicators and postsurgery DVT risk. After adjustment for important confounders and effect modifiers, the findings emphasized the importance of BV in DVT prevention and are of a certain accuracy, which may have great guiding significance for follow-up clinical work and imply a breakthrough point for subsequent researches. However, due to the generally high cost of measuring BV-relevant parameters in Chinese hospitals, we failed to describe the specific changes of these parameters by retests. Still, the small sample size of males and the possible uncontrollable factors during TKA surgery may limit our results.
Conclusion
In conclusion, in primary KOA patients treated with TKA, preoperative low whole BRV is independently associated with postoperative DVT. The result may be valuable for recalling the role of BV in thrombosis formation and optimizing prophylaxis methods.
Footnotes
Acknowledgments
The authors would like to acknowledge all participants, the nurses, the ultrasound department, and the clinical laboratory for their patience and assistance.
Author's Note
X.D., X.W., and W.D. designed the study and wrote the article. Z.H. and K.W. collected the blood samples. X.D., Z.H., and W.D. provided the funding. X.D., X.W., Z.H., and W.D. did the operations and data analysis. X.W. and K.W. made the diagnosis for DVT and set the exclusion criteria of this study. X.D., X.W., Z.H., and W.D. revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Committee Approval and Guidelines on Patient Consent
All procedures involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical approval to report this case series was obtained from the local ethics committee of the Third Affiliated Hospital of Soochow University (CY20100304)* and written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Basic Research Project of Changzhou Science and Technology Bureau (grant number CJ20200112).