
Abstract
Drug interactions with novel oral anticoagulants (NOACs) may decrease their advantages. We aimed to explore the drug interaction rates with NOACs and impacts of drug interaction index (DII) on mortality among older patients with atrial fibrillation (AF). In this retrospective cohort study, we enrolled 704 eligible patients aged 65≤ with AF between January 1, 2018 and December 30, 2019 in a tertiary outpatient cardiology clinic. We recorded demographic, clinical characteristics, and medications for the last 3 months. At the end of the evaluation visit (March 1, 2020), death events and dates were recorded. All medications were checked for drug interactions using Lexicomp® software. Each drug interaction was annotated according to risk grade. Moreover, we determined a new index ratio of C/D/X classes to total interactions called DII. The mean age was 75.19 ± 7.13 and 398 (56%) were male. Death events were observed in 106 (15%) patients. A total of 9883 drugs were analyzed for drug interactions. The majority of drug interactions were in class A (80.7%). Clinically relevant interactions were 14.6% (Class C/D/X). The area under receiver operating characteristic curve was 0.704 (95% confidence interval: 0.653-0.754) and 0.167 cutoff value (68.9% sensitivity and 80.2% specificity [3.11 positive likelihood ratio]) for DII to predict mortality. This study showed an overview of the NOACs interactions in older patients with AF. Additionally, the inappropriate NOAC dose and DII showed an association with mortality. NOAC treatment should be guided by drug interaction applications to reduce mortality.
Introduction
Atrial fibrillation (AF) is the most common arrhythmia that increases the risk of death by 1.5- to 2-fold. 1 AF prevalence is approximately 9% to 12.3% in the geriatric population.2,3 After 2011, a critical drug group for managing AF complications, novel oral anticoagulants (NOAC), were introduced to the Turkish market. 4 Since then, the anticoagulation market has grown in favor of NOACs and they have been proven to prevent ischemic strokes and prolong life for patients with AF. 5
Despite the safety profile of NOACs, some medications could interact and may decrease their safety and efficacy. Drug interactions are a concern because polypharmacy is becoming more common in older people with comorbid diseases. However, most of our consideration of drug interaction with NOACs comes from limited studies conducted mostly in younger populations, animal models, and case reports. 6–8 Therefore, identifying potential interactions causing an increased risk of NOAC-related complications has emerged as an essential issue.
Most of the studies evaluating the drug interactions dwell on only the clinically relevant part. 9–11 Clinically relevant drug interaction is described as a recommendation for monitoring or modifying the therapy according to Lexicomp® application (Class C, D, and X). Moreover, there is a neglected aspect in previous studies. We believe that interaction intensity should be evaluated as the third dimension besides the drug numbers and clinically relevant interactions. However, there is no parameter for evaluating drug interaction intensity. So, we developed an index to reflect interaction intensity. This index could be simply explained as taking the ratio of clinically relevant drug interactions to total drug interactions.
There are 2 primary aims of this study: (1) To determine potential drug interaction rates with NOACs. (2) To ascertain the effects of drug interaction index (DII) on mortality among older adults AF patients.
Material and Methods
Patient Population
We performed a single-center, retrospective cohort study at the Afyonkarahisar Health Sciences University Hospital (AFSU), a 550-bed teaching hospital in Turkey. All adult patients admitted to the AFSU outpatient clinic who were prescribed apixaban, dabigatran, edoxaban, or rivaroxaban from January 1, 2018 to December 30, 2019 were identified from an electronic medical record system (Enlil, Hospital Management System). Criteria for selecting the subjects were: (1) aged 65 and over; (2) diagnosed AF; (3) taking 1 NOAC for at least 3 months before the assessment; and (4) medication list including last 3 months. A total of 828 individuals were identified for the first assessment. Then, 112 subjects were excluded based on these factors: taking NOACs for less than 3 months before the drug interaction assessment (n = 68); non-AF situations as deep venous thrombosis (n = 24); pulmonary thromboembolism (n = 3); severe rheumatic mitral stenosis (n = 17) diagnosed as valvular AF due to not required NOACs (Figure 1).

Flow diagram of the inclusion procedure.
After identifying 716 recorded individuals, 12 patients whose drug information could not be reached were excluded during visits between January 2, 2020 and March 1, 2020 (Figure 1). Finally, we evaluated and recorded 704 eligible patients’ concomitant diseases, CHA2DS2VASC and HASBLED scores, and medications for the last 3 months from the drug lists provided by the pharmacies in a national medication tracking system. During the evaluation visit, routine blood tests and echocardiography results were also recorded. At the end of evaluation visits (March 1, 2020), death events and dates were recorded from the system (National death notification system that provides only death events and dates).
Drug Interaction Measurement
We checked all prescriptions for drug interactions using Lexicomp®-Online software (Lexi-Comp, Inc.,). Each drug interaction is annotated with a risk grade based on the relevance of the interaction. This program's classification is as follows: A—no evidence of interactions in literature; B—known interactions but no action needed; C—monitor therapy; D—consider therapy modification; X—avoid combination. Some medications and supplements cannot be classified and are noted as not applicable.
Most studies were evaluating drug interactions with the Lexicomp® application focus only on the clinically relevant part (C, D, and X). Previous researchers have not usually considered classes A and B.9,10 We believe that a parameter including total drug number and clinically relevant drug interactions at the same time should be evaluated as the third dimension. So, we developed a new index called “the DII” defined as follows: firstly, drug interaction groups were determined as A, B, C, D, and X according to the Lexicomp® classification. Secondly, we count a sum of group C, D, and X interaction numbers and total interaction numbers. Thirdly, we calculate group C, D, and X ratio to all groups (A, B, C, D, and X). The DII formula showed below:

Statistical Analysis
We calculated the sample size for a logistic regression test allowing 95% statistical power, 5% alpha error, and 0.3 R2, two-sided, with an odds ratio (OR) of 1.9 for the mortality associated with AF 15 using Gpower software v3.1.9.4 (Erdfelder, Faul, & Buchner, 1996). 16 The estimated sample was 704.
Statistical analyzes were conducted using the SPSS software version 22.0 (SPSS, Inc.). The mean and standard deviation (SD) or median and interquartile ranges (IQR) were used for descriptive statistics. Chi-square and Fisher's exact test analyzed categorical variables whenever appropriate. The variables were analyzed using visual and analytical methods (Kolmogorov–Smirnov test) to determine whether they were normally distributed.
Among the NOAC subgroup, a comparison of means was by the analysis of variance test, and the chi-square test compared variables. Categorical variables and medians were analyzed using the Kruskal–Wallis test and evaluated using the Bonferroni correction.
Determining the best predictor(s) that affect(s) mortality outcome (ie age, congestive heart failure, chronic kidney disease, diabetes mellitus, coronary artery disease, stroke/transient ischemic attack, inappropriate NOAC dosage, daily medication number, DII, and HASBLED and CHA2DS2VASC scores) was performed by using the multiple logistic regression enter method. A P-value of less than .05 was considered to show statistically significant results.
Ethical Considerations
The study was approved number 2020/8 by the Ethics Committee of AFSU. The study was conducted under the guidelines of the declaration of Helsinki and the principles of good clinical practice and respect for the rights and dignity of all parties. Verbal informed consent was obtained from participants following a brief explanation of the aim of the study.
Results
Among the 704 eligible patients enrolled in the study, the median age was 75.19 ± 7.13 and 398 (56%) were male. All patients were diagnosed with AF previously. The most prescribed NOACs in our study population were rivaroxaban (49.5%) and apixaban (35.9%). The main comorbidity was cardiovascular diseases such as arterial hypertension (514 [73%]), ischemic heart disease (319 [45.3%]), and heart failure (234 [33.2%]). The mean (±SD) CHA2DS2VASC score was 4.11 ± 1.56 and the mean HASBLED score was 4.14 ± 0.88. Death events were observed in 106 (15%) patients using NOACs for 3 months or more (Table 1). A critical result from the data is that 167 (23.4%) patients were taking inappropriate NOAC dosage.
Characteristics and Drug Interaction Groups of the Study Population at Baseline.

Abbreviations: F, Female; M, Male; TIA, transient ischemic attack; N/A, not applicable; NOAC, nonvitamin K oral anticoagulant; SD, standard deviation; IQR, 25-75 interquartile range.
The 82.5% of medications (8169) have no or low drug interaction class (Class A and B). And clinically relevant drug interaction groups were as follows: 256 class C (2.7%), 1168 class D (11.8%), and 23 class X (0.2%). Additionally, clinically relevant drug interaction rates were not different among NOAC subgroups (Table 2). The majority (66%) of group X was antiepileptics (carbamazepine, phenytoin).
Subgroup Analyzes of Drug Interaction Characteristics and Test Results of the Study Population.

Abbreviations: WBC, white blood cell; Hb, hemogram; Plt, platelet; GFR, glomerular filtration rate; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LVEF, left ventricle ejection fraction; NOACs, nonvitamin oral anticoagulants; TIA, transient ischemic attack; N/A, not applicable; SD, standard deviation.
One-way analysis of variance was used to test and Kruskal–Wallis test differences among the 4 groups and post hoc analyzes were conducted using the Tukey test and Duncan test multiple-comparisons test.
Compared to edoxaban group, P < .05.
Compared to dabigatran group, P < .05.
The 570 (81%) were taking 5 or more drugs. The median number of prescribed medications (IQR) was 14 (9-19). The median DII (IQR) was 0.130 (0.025-0.210). A total of 9883 concomitant drugs were analyzed for potential interactions. Most drug interactions were in class A (80.7%; Figure 2).
According to subgroup analyzes of the study population, there was no difference in mortality (P = .175), clinically relevant drug interaction rates (class C, P = .115; class D, P = .313; class X, P = .341), DII (P = .721), blood test results (white blood cell P = .102, Hemogram, P = .932, Platelet P = .105, Glomerular filtration rate [GFR], P = .244, Aspartate aminotransferase P = .434, Alanine aminotransferase, P = .222) left ventricular ejection fraction (P = .788), or CHA2DS2VASC (P = .374) and HASBLED scores (P = .507) between NOACs (Table 2). However, most higher rates of inappropriate dosing were in apixaban (P < .001) and there was a shorter duration of NOAC taking in edoxaban (P < .001; Table 2).
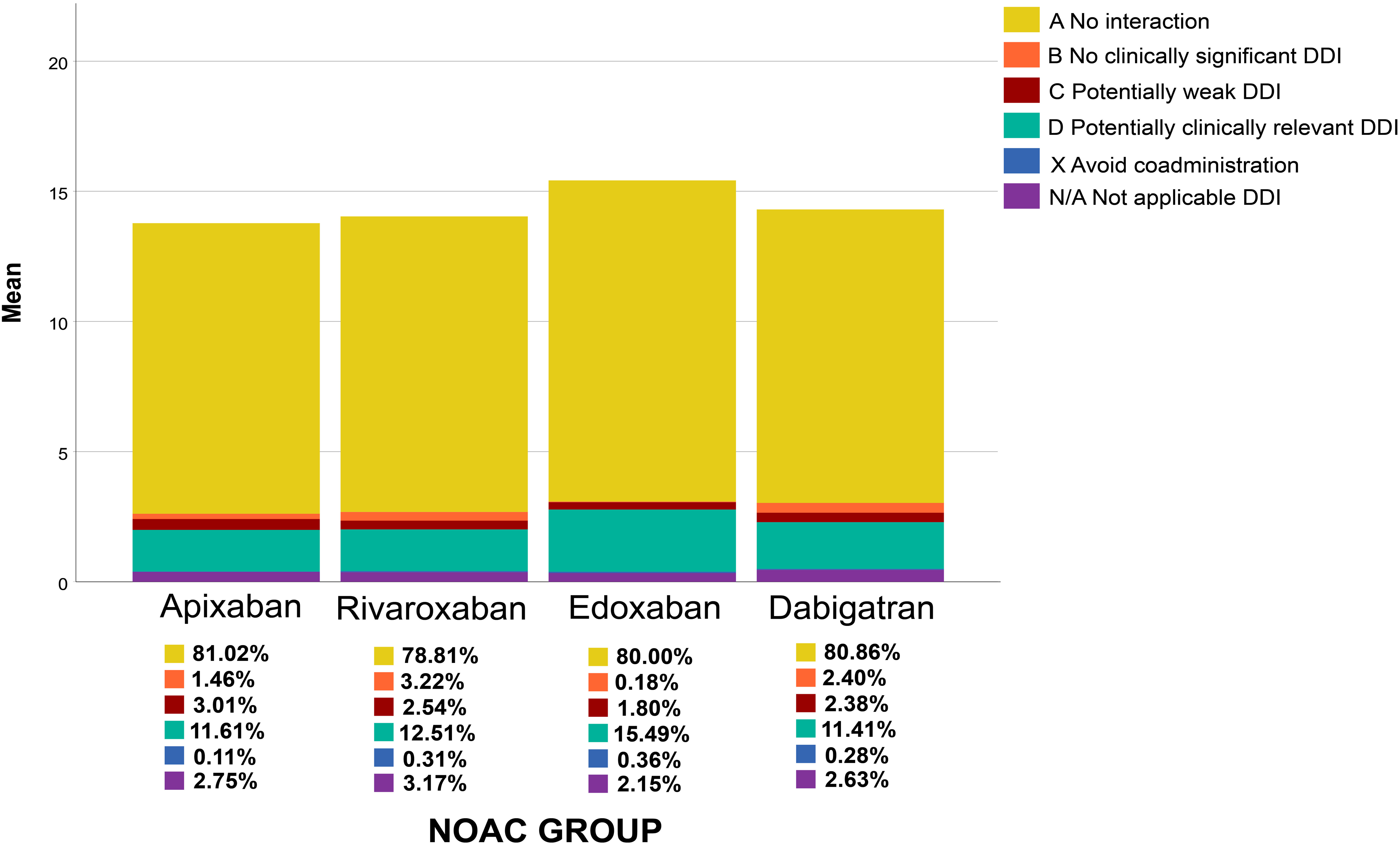
Drug interaction rates according to NOAC subgroups.
The receiver operating characteristic analysis was conducted to identify the DII value for mortality prediction; an AUC 0.704 and cutoff value was 0.167 with 68.9% sensitivity and 80.2% specificity (3.11 positive likelihood ratio) for the DII could predict mortality with 95% CI:0.653 to 0.754 (P < .001; Figure 3).

The ROC analyzes for the ability of drug interaction index to mortality prediction.
Logistic regression was performed to ascertain the effects of age, congestive heart failure, chronic kidney disease, diabetes, ischemic heart disease, stroke/transient ischemic attack, inappropriate NOAC dose, daily medication number, DII, and HASBLED and CHA2DS2VASC scores on the likelihood of mortality. The logistic regression model was statistically significant, χ2 = 329.151, P < .001. The model explained 55.3% (Nagelkerke R2) of the variance in mortality and correctly classified 84.9% of cases. Inappropriate NOAC dosing (OR: 2.211 [95% CI: 1.205-4.055], P = .010), increasing age (OR: 1.079 [95% CI: 1.034-1.126], P < .001), congestive heart failure (OR: 3.363 [95% CI: 1.792-6.313], P < .001), DII (OR: 6.065 (95% CI: 4.055-16.716], P < .001), total drug count (OR:1.939 [95% CI: 1.903-1.977], P = .001), HASBLED score (OR: 11.291 [95% CI: 6.951-18.341], P < .001), and CHA2DS2VASC score (OR:1.551 [95% CI: 1.438-1.694], P < .001) were all associated with an increased likelihood of mortality (Table 3).
Univariate and Multivariate Logistic Regression Analysis of Predictors for the Mortality.

Abbreviations: OR, odds ratio; CI, confidence interval; NOACS, nonvitamin K oral anticoagulants.
Discussion
NOAC treatment rates have been increasing in older adults, and recent guidelines put NOACs into standard therapy for AF.4,11 However, current guidelines11,12 often do not include drug–drug interaction management in geriatric AF with comorbidity because it has often not been studied. Thus, it is still unknown whether drug interactions could increase the mortality rate in real life. Our study's initial objective was to find out the impacts of drug interaction intensity on mortality in older adults with AF. Furthermore, we found that a higher DII with a 0.167 cutoff value could be an independent risk factor for all-cause mortality. The regression analysis also showed that age, congestive heart failure, inappropriate NOAC dose, medication number, HASBLED, and CHA2DS2VASC scores affect mortality. Another finding was that the majority of medications have no or low drug interaction levels. Clinically relevant drug interaction rates were 14.6% for all NOACs and did not differ among NOAC subgroups.
In our study, the drug number was median 14 and 81% of patients took 5 or more drugs. According to the post hoc analysis of the phase III studies of rivaroxaban and apixaban, two-thirds of the participants consist of patients with polypharmacy.17,18 A previous report from Turkey showed that 55% of AF patients taking NOAC have polypharmacy. 19 Hypertension, ischemic heart disease, heart failure, and diabetes were the main contributors to polypharmacy. Our polypharmacy levels were higher compared to the literature. This finding may be explained by our participants’ nature. Polypharmacy is a result of increased age and multiple morbidities. Only 18 participants (0.2%) had no comorbid disease except AF. As expected, our population had higher CHA2DS2VASC and HASBLED scores, which are associated with mortality. There was no difference in death rates, comorbid diseases, HASBLED and CHA2DS2VASC scores, renal and hepatic functions among NOAC groups in our study group.
The results of this study show that the most powerful predictor of mortality was a higher HASBLED score (Table 3). This finding was also reported by Gallego et al 20 According to the multifactorial nature of death, bleeding, and thrombotic events were the greatest causes for mortality in older patients with AF. The HASBLED score was designed to predict bleeding; however, it has a strong relation with thrombotic risk and, thus, to mortality. 21 To develop a full picture of mortality in high HASBLED scores, additional studies will be needed to determine bleeding or thrombosis in the setting of elderly AF using NOACs.
We found one-quarter of the study population was taking inappropriate NOAC doses. This finding was consistent with other international studies where prescription errors were 26% and 28% for inappropriate drug choice.22,23 When we look at NOAC agents, specifically, dabigatran was less inadequate, while edoxaban was a higher prescription error. This finding could arise from considering both the 110- and 150- mg doses could be used in states of renal impairment (eGFR <80 mL/min). 24 Additionally, edoxaban has less class B interaction than other NOACs, but this did not seem to influence the mortality or preliminary results. As demonstrated in patients taking apixaban, underdosed NOAC patients have an increased risk of thromboembolic events (5-fold increased risk of stroke). 25 Another important finding was that inappropriate NOAC dosing rate was the most contributing part to the mortality. Consistent with the literature, we found an OR of ∼2.0 for the presence of mortality for inappropriate dosage. 26 The exact mechanism is still unclear, but it may be explained by 2 factors: drug-related and patient-related components. Incorrect dosing could decrease the advantage of NOACs; both bleeding and thrombosis could increase death events. Patient-related factors such as senility, fragility, and multiple comorbid diseases could decrease the tolerance of inappropriate dosing and increase mortality. A further study with more focus on inappropriate NOAC dose and mortality is therefore suggested. Another finding was the duration of edoxaban usage was lowest than other NOACs. This is mainly caused by the limited postlicensing period of edoxaban.
NOACs have less drug interaction potential than vitamin K antagonists, but some recent reviews revealed that cytochrome p450 (CYP450) isozyme inducers, P-glycoprotein (P-gp) could be implicated in drug interaction mechanisms. 27–29 As highlighted in the reviews, we also found that most of the class X interaction mechanisms depend on inducers of CYP3A4 and P-gp, such as carbamazepine, phenytoin, and rifampicin, 30 having a potential effect on NOACs 31 (see the Supplemental Material). Among mentioned drugs, carbamazepine could require long-term use. Moreover, it cannot be easily switched to alternative drugs. We found 14 epilepsy patients taking carbamazepine in our study population. More attention is needed to drug interactions in the management of older patients with AF and epilepsy.
In reviewing the literature, we found only 3 cohort studies that evaluated the drug interactions with NOACs in AF. 31–33 Nevertheless, these studies did not test mortality and examined only specific drug interactions by generic drugs that result in bleeding. The most frequently interacting drugs in these 3 large studies were phenytoin, nonsteroidal antiinflammatory drugs (NSAIDs), diltiazem, amiodarone, rifampicin, and verapamil. 31–33 Our research found carbamazepine, phenytoin, rifampicin, and enzalutamide in the severe interaction group (class X), and the most frequent class D interacting agents were diclofenac, dexketoprofen, naproxen, acetylsalicylic acid, clopidogrel, and propafenone in the moderate interaction group. In our study, the clinical relevant interaction was level was 20%, lower than the previous cohort study reported by Bezahbe et al 33 Different drug interaction assessment methods could explain this. Some medications were classified into different interaction groups with each NOACs by Lexicomp® application. For example, diltiazem has no interaction with edoxaban and dabigatran (class A) while moderately interacting with apixaban (class C).
A novel aspect of this research is considering the drug interaction intensity. An advantage of the DII is a numerical measure of the drug interaction intensity in total medications. It was hypothesized that DII as a parameter, including the drug numbers and interaction rate, could affect mortality prediction. Moreover, the present data shows that DII with a 0.167 cutoff value could predict mortality for the first time. The observed association between DII and mortality might be due to older patients with AF tend to have more comorbidity and complex comedications; these situations create a foundation for more severe drug interactions. Prior reports showed that drug interactions with NOACs were relatively common in patients aged over 65.34,35 Classic examples of severe drug interactions with NOACs were antidepressants, NSAID, antiplatelets, amiodarone, rifampicin, and carbamazepine. These medications require long-term use in chronic diseases. Receiving continual multiple interacting agents could cause significant alteration in NOAC plasma levels and the benefits could be lost. This mechanism could be responsible for all-cause mortality in our study. Thus, our study reveals an important aspect of treating older patients with AF receiving NOAC and need to exercise special caution in elderly patients on polypharmacy.
However, these results need to be interpreted with caution because the present study has several limitations. Firstly, due to the study's retrospective observational nature, only associations can be drawn, and causal relationships cannot be inferred. Secondly, the DII is structured to measure interaction with NOACs, but we do not know comedications’ interactions with each other. Thirdly, we only tested for mortality and did not evaluate bleeding or ischemia, reflecting anticoagulant effects. Another limitation we only determined all-cause mortality; cardiovascular deaths are not known.
Moreover, we examined drug interactions only from 1 online application. It could be argued that other drug interaction software like Micromedex, iFacts, Medscape, and Epocrates could have different results. However, several reports have shown that Lexicomp® was the most accurate and comprehensive software among the drug interaction software.36,37 Nevertheless, we did not measure NOAC plasma levels. It is not a full pharmacokinetic and pharmacodynamic assessment. A final inherent limitation of this study was that DII does not consider dose-based NOAC interaction. So, this study does not fully consider the problems that can appear in real situations. However, it does demonstrate the need for further research.
Conclusion
To the best of our knowledge, this is the first study that evaluated the mortality risk associated with drug interaction intensity in older patients with AF prescribed NOACs. Moreover, the new DII 0.167 cutoff value showed an association with mortality. There was no difference in clinically relevant drug interactions among older patients with AF taking various NOACs. Therefore, NOAC treatment should be guided by drug interaction applications to reduce mortality in geriatric AF patients.
Supplemental Material
sj-docx-1-cath-10.1177_10760296211038685 - Supplemental material for Novel Drug Interaction index and Risk of Mortality in Older Patients With Atrial Fibrillation Receiving Non Vitamin K Oral Anticoagulants (NOEL Drug)
Supplemental material, sj-docx-1-cath-10.1177_10760296211038685 for Novel Drug Interaction index and Risk of Mortality in Older Patients With Atrial Fibrillation Receiving Non Vitamin K Oral Anticoagulants (NOEL Drug) by İbrahim Ersoy in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
This article did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
Ibrahim Ersoy spoken at an educational meeting sponsored by Pfizer, a non vitamin K oral anticoagulant manufacturer.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.