
Abstract
To investigate the effect of different pressing time on the incidence of subcutaneous hemorrhage of low molecular weight heparin (LMWH) administration by meta-analysis. Cochrane Library, PubMed, MEDLINE, CINAHL, EMbase, Springer, EBSCO, China Biomedical Literature Database, CNKI, Wanfang Database, and VIP Database were searched. To screen the literature of randomized controlled trials with different pressing time in patients with subcutaneous LMWH injection from the establishment of the database to December 2020. The quality of the literature was evaluated and the data were extracted. Meta-analysis was performed by RevMan 5.3. A total of 17 randomized controlled trials were included. Meta-analysis showed that the bleeding rate of pressing for 5 min odds ratio (OR = 3.89, 95% confidence interval [CI]: 2.68-5.64, P < .05) or pressing for 10 min (OR = 1.99, 95% CI: 1.34-2.95) was significantly lower than that of pressing for 3 min. Moreover, the bleeding rate was significantly lower in the 5 min pressing (OR = 1.47, 95% CI: 1.18-1.82) and 10 min pressing(OR = 2.12, 95% CI: 1.61-2.77) than in the no compression group. It is the most suitable time to press 5 min after subcutaneous LMWH injection, which can better control the incidence of bleeding.
Keywords
Introduction
Low molecular weight heparin (LMWH) is a widely used anticoagulant drug in clinic. Its adverse reactions mainly include subcutaneous hemorrhage, pain, thrombocytopenia, skin necrosis, and subcutaneous hemorrhage is the highest incidence of adverse reactions.1,2 In addition to the patient's own factors, the factors affecting the local bleeding of subcutaneous LMWH injection include injection site, injection mode, injection time, and pressing time after injection. Among them, improper pressing after needle extraction is an important reason for subcutaneous hemorrhage. If the pressing time is too short, it is easy to cause subcutaneous hemorrhage and form bruises. The longer the bleeding time is, the larger the area of bruises is. 3 Blood stasis refers to capillary hemorrhage in the dermis and subdermal layer of the skin, resulting in discoloration of the skin with an area ≥2 mm2. It usually reaches the peak at 48 h after injection and begins to fade 72 h after injection. 1 The ecchymosis will affect the subsequent injection operation, reduce the scope of subcutaneous injection, and cause patients' discomfort, tension, and worry, as well as their distrust of nurses. At present, Akbari et al 4 published a systematic evaluation of the injection time, pain, and subcutaneous hemorrhage of the liquid. They believed that compared with rapid injection, the pain intensity and bruises caused by slow injection were obviously reduced. Dihongyue et al's 5 meta-analysis of adverse reactions of different subcutaneous injection methods showed that LMWH vertical subcutaneous injection method was better than the traditional subcutaneous injection method. Huang et al 6 systematically evaluated whether pressing was needed after subcutaneous injection. They believed that not pressing after subcutaneous LMWH injection did not increase the incidence of local moderate-to-severe subcutaneous hemorrhage and the pressing time had a certain impact on subcutaneous hemorrhage. However, no specific pressing time was compared in this study. Therefore, this study explored the optimal pressing time after subcutaneous LMWH injection by meta-analysis, so as to provide reference for clinical injection of LMWH and reduce the occurrence of bleeding.
Data and Methods
Literature Retrieval
Randomized controlled trials (RCTs) published in English and Chinese from the database establishment to December 2020 were searched. The key words of “low molecular weight heparin,” “low molecular weight,” “heparin,” “subcutaneous,” “injection,” “oppression,” and “pressing” were searched in Chinese biomedical literature database, CNKI, Wanfang database, and VIP database. And the Cochrane Library, PubMed, MEDLINE, CINAHL, EMbase, Springer, and EBSCO databases were searched with the keywords of “Heparin,” “Low-Molecular-Weight,” “Injections,” “subcutaneous,” “hypo,” “press,” “constrict,” “stress,” “standard procedure,” and “time.”
Criteria for Inclusion and Exclusion of Literature
Inclusion Criteria: Research Design: Randomized controlled trials or quasiexperimental studies (including self-control trials). Subjects: Patients with cardiovascular and cerebrovascular diseases aged ≥18 years received subcutaneous LMWH injection during hospitalization, excluding those who with severe hemorrhagic diseases and other coagulation disorders. Intervention: After subcutaneous LMWH injection, patients were given different pressing time: 0 min (without pressing), 3 min, 5 min, and 10 min. Except pressing time, there should be no difference between the 2 groups in other processes, injection methods and pressing methods, otherwise it cannot be included. Results: Incidence of local hemorrhage 12 h after subcutaneous LMWH injection. After comprehensive literature, the ecchymosis diameter <0.5 cm was considered as no bleeding.
Exclusion Criteria: Unable to obtain data and original literature; poor quality, missing data, repetitive reports of literature; case report, literature review, and animal experiments.
Literature Quality Evaluation and Data Extraction
NoteExpress3.2 literature management software was used to deduplicate the initial test literature, the remaining literature was screened according to the topics and abstracts, and the literature that obviously did not meet the inclusion criteria was deleted. Read the full text of the remaining literatures thoroughly, screen again according to the inclusion and exclusion criteria to determine whether their subject matter, study design, outcome measures, etc, meet the inclusion criteria; trace the relevant literatures according to the references after the obtained literatures.
On the basis of the references after the obtained literature, the relevant literature was traced. The risk of bias in literature inclusion was evaluated according to the quality standard of Cochrane handbook. 7 Including 6 experimental characteristics: random sequence generation (selection bias) allocation method; the allocation concealment (selection bias) of allocation random scheme; blind method (implementation bias) was adopted for the research objects and intervention implementers; blind method (observation bias) was adopted for the result evaluators; the integrity of outcome data (attrition bias); selective reporting of research results (report bias); other bias. The quality of the literature is grade A if it does not meet the above criteria at all and has the least possibility of bias; grade B if it partially meets the above criteria and has the moderate possibility of bias; grade C if it completely does not meet the above quality standards and has the high possibility of bias. After all the documents were independently evaluated by 2 researchers (JF and GFP) according to the above evaluation criteria, the 2 researchers discussed the quality of each document according to the above evaluation criteria and reached a consensus to form the final literature quality evaluation. If there are differences in the results, it will be discussed and solved with the third researcher to form a final literature quality evaluation after reaching a consensus. Finally, a standardized data extraction table is developed according to the contents of the literature, including basic information of the literature, quality evaluation results, research methods, research objects, number of samples, outcome indicators, and conclusions.
Statistical Analysis
RevMan 5.3 software was used for meta-analysis of the data. Firstly, the heterogeneity between studies is evaluated by Q test and I2 statistics. If P > .05 and I2 < 50%, then use fixed effect model for meta-analysis; If P < .05 and I2 > 50%, then choose random effect model. If P < .05 and the source of heterogeneity cannot be determined, then the descriptive analysis will be adopted. Odds ratio (OR) for binary variables (bleeding rate) and 95% confidence interval (CI) for each score were calculated. The P < .05 is the test level of the combined analysis hypothesis.
Results
Study Selection
A total of 2108 related literature were initially detected, including 993 in Chinese and 1115 in English. Repetitive articles of 1063 and articles that did not meet the inclusion criteria were excluded, and 68 articles that did not meet the subject, research design or outcome indicators were excluded according to the title and abstract. After filtering, 17 studies were enrolled for the final evaluation.8–24 The included references were all in Chinese. And the basic characteristics of the included literature are shown in Table 1.
Basic Characteristics of Included Literature.
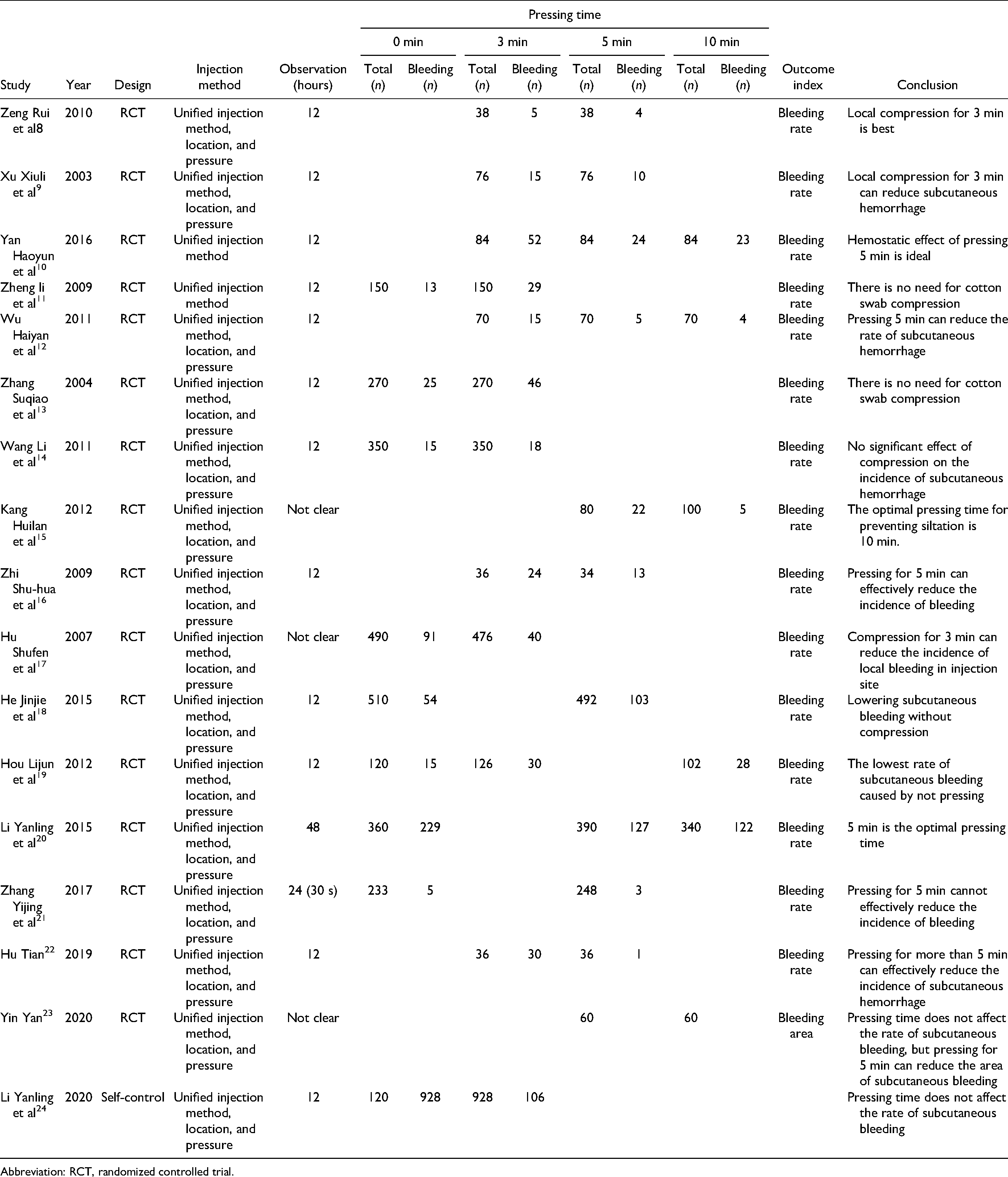
Abbreviation: RCT, randomized controlled trial.
Study Quality Assessment
The quality of the included literature was evaluated according to the Cochrane Handbook and the results showed that the quality of the included literature was B grade (Table 2).
Included in the Literature Quality Evaluation Table.

Clinical Characteristics of Included Studies
A total of 6432 subjects were included in the 17 articles (Table 1). Different studies set different pressing times for comparison. One study 21 concluded that pressing for a short time (30 s) after injection did not increase the risk of local bleeding; 3 concluded8,9,11 that pressing for 3 min was appropriate; 6 believed10,12,16,20,22,23 that pressing for 5 min was the best time; 1 believed 14 that pressing for 10 min could prevent the occurrence of bleeding, and 6 believed11,13,14,18,19,24 that pressing was not necessary.
Effect Evaluation of Different Pressing Time on Incidence of Subcutaneous Hemorrhage
Among the 17 articles included, heterogeneity between studies was lager for all subgroups (I2 > 50%, P < .05) and were analyzed separately using a random effects model. The combined results showed that the bleeding rate of pressing for 5 min was significantly lower than that of pressing for 3 min (OR = 3.89, 95% CI: 2.68-5.64; Figure 1A, P < .05). And the bleeding rate of pressing for 10 min was significantly lower than that of pressing for 3 min (OR = 1.99, 95% CI: 1.34-2.95; Figure 1B, P < .05). However, there was no significant difference in the effect of pressing for 10 and 5 min (OR = 1.09, 95% CI: 0.84-1.41) (Figure 1C, P > .05) and no pressing and pressing for 3 min on the bleeding rate (OR = 1.04, 95% CI: 0.87-1.24; Figure 1D, P > .05). The bleeding rate of pressing for 5 min (OR = 1.47, 95% CI: 1.18-1.82; Figure 1E, P < .05) and pressing for 10 min (OR = 2.12, 95% CI: 1.61-2.77; Figure 1F, P < .05) was significantly lower than that of nonpressing.

Forest plot of bleeding incidence at different times after subcutaneous LMWH injection, (A) press 3 and 5 min effect analysis; (B) press 3 and 10 min effect analysis; (C) effect analysis of pressing for 5 and 10 min; (D) effect analysis of pressing for 0 and 3 min; (E) the effect analysis of pressing 0 and 5 min; (F) effect analysis of pressing for 0 and 10 min.
Discussion
The anticoagulant LMWH has the advantages of good injection absorption, long half-life, high bioavailability, better clinical efficacy, and low incidence of complications such as bleeding and thrombocytopenia, which is more widely used in clinical practice. However, LMWH is easy to cause subcutaneous hemorrhage and local pain at the injection site, and the incidence of subcutaneous hemorrhage is related to the injection method, injection site, injection time, and pressing time. 25 In the present study, all the 17 RCTs included had uniform inclusion criteria for the subjects, and the baseline consistency was analyzed. There were uniform injection methods, sites, compression intensity, observation time, and measurement criteria. In addition, according to the basic characteristics of the included literature, it can be found that there are also differences in bleeding time after subcutaneous LMWH injection. Palese et al 26 believed that ecchymosis reached its peak at 48 h and began to fade after 72 h, so 48 h of subcutaneous injection was taken as the observation time point. Most of the domestic literature takes subcutaneous injection for 12 h as the observation point, only 1 literature 20 takes 48 h as the observation point. The quality of the included literature was evaluated, and the data results were complete, but the quality evaluation results of the included research methodology were medium. The main problems were as follows: only 1 paper 20 was clearly randomized by random number table method, 4 were8,13,14,18 self-control, and the other were not stating random methods. Only 1 document 20 clearly explained the hidden methods of allocation schemes; no blind method was used for the surveyors.
In our mate-analysis, we found that the comparison of different pressing times presented different results. The rate of subcutaneous bleeding was lower after subcutaneous LMWH injection by pressing for 5 or 10 min than without pressing or pressing for 3 min, and the pressing time extended to 10 min did not reduce the subcutaneous bleeding rate. In addition, Yin et al 23 demonstrated that pressing for 5 min after subcutaneous LMWH injection also reduced the area of subcutaneous hemorrhage. These results suggest that the appropriate duration of compression can better control the occurrence of subcutaneous bleeding rate of subcutaneous LMWH injection.
However, there are still some limitations in this study. The quality of included research is not high and there are possibilities of selective bias, implementation, and measurement bias and loss bias to varying degrees. This weakens the conclusion strength of this study. This also suggests that higher quality RCTs are needed to verify the appropriate pressing time after subcutaneous LMWH injection. On the other hand, the patients included in this study were all patients receiving anticoagulant therapy in the department of cardiology. The types of subjects were not subdivided and the disease types and departments of patients were not considered. In the future, the pressing time and bleeding rate required by patients with different diseases can be compared and analyzed.
In conclusion, pressing 5 min after subcutaneous LMWH injection is the most appropriate time to reduce the incidence of subcutaneous hemorrhage. This will reduce unnecessary workload for clinical nurses and improve patient compliance.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.