
Abstract
Apixaban is indicated for the prevention of ischemic stroke in non-valvular atrial fibrillation (NVAF), as well as for the prevention and treatment of venous thromboembolism (VTE). Dose adjustment is based on age, weight, and serum creatinine in NVAF, while there are no recommended adjustment criteria for VTE. Such adjustment is unconventional compared to other commonly used medications. The objective of this manuscript is to critically analyze each apixaban dosing adjustment criterion and its associated outcomes. PubMed articles from March 2013 to March 2020 were selected with search terms “apixaban,” and “dose adjustment,” “adjustment,” or “adjustment criteria.” Pharmacokinetic studies demonstrated increased apixaban exposure in patients >65 years of age, those with extreme body weights, and those with advanced renal impairment, though post-hemodialysis dosing may off-set the elevated apixaban exposure. However, clinical data show that among patients
Keywords
Introduction
Apixaban is a direct-acting oral anticoagulant (DOAC) initially approved in 2012 for stroke prevention in patients with non-valvular atrial fibrillation (NVAF) and for the prevention and treatment of venous thromboembolism (VTE) in 2014. The dose adjustment criteria are not consistent across indications. For NVAF, apixaban is dosed at 5 mg orally twice daily and is reduced to 2.5 mg twice daily in patients who meet 2 of the following criteria: age
Methods
PubMed was used to search for articles published between March 2013 and March 2020. Search terms included: “apixaban,” and “dose adjustment,” “adjustment,” or “adjustment criteria.” During an initial screening, 192 articles were identified and after the use of filters such as human, English, and full-text, 121 articles were screened. Studies on indications other than NVAF and VTE, studies on pediatric patients, case reports or case series, and commentaries or editorials were excluded.
Rationale for Dose Adjustment Criteria
Patients with NVAF and at least 2 of the dose adjustment criteria have demonstrated higher risk for major bleeding and all-cause death compared to patients with ≤1 dose adjustment criterion. 4 Regardless, this does not fully explain the selection of the specific dose adjustment criteria. We begin our exploration of each criterion by evaluating the pharmacokinetic data.
Clinical Pharmacokinetics of Each Dose Adjustment Criteria
Age > 80 years
An open-label study assigned 2 groups of participants to receive a single dose of apixaban 20 mg: 1) patients between 18 and 40 years of age, and 2) patients >65 years. The maximum plasma concentration (Cmax) was similar between the 2 groups, but the area under the concentration-time curve (AUC) was 32% higher among those >65 years. The mean elimination half-life was longer in those >65 years (15.45 vs. 11.98 hours). 5 Thus, patients >65 years displayed higher apixaban exposure and reduced drug clearance. This age cut-off is inconsistent with the dose adjustment criterion of ≥80 years per the drug manufacturer.
Weight ≤ 60 kg
In an open-label randomized controlled trial that enrolled patients with extremes of body weight, patients with low body weight (<50 kg) had approximately 27% higher Cmax and 20% higher AUC. Those with high body weight (
SCr > 1.5 mg/dL
In an open-label study, a 10 mg oral dose of apixaban was given to patients with normal renal function, mild renal impairment with CrCl >50 to 80 mL/min, moderate renal impairment (CrCl 30 to 50 mL/min), and severe renal impairment (CrCl <30 mL/min). The Cmax was not significantly different, but the AUC increased by 16%, 29%, and 38%, respectively, compared to those with normal renal function. 7 The manufacturer chose a different measure of renal function (SCr) for dose adjustment. Another open-label study compared a 5 mg oral apixaban dose in patients with normal renal function to those on hemodialysis (HD) in whom a 5 mg dose was given 2 hours pre-HD and a 5 mg dose was given 7 days post-HD. When apixaban was given pre-HD, the Cmax and AUC were 13% and 14% lower, respectively, versus non-HD patients. 8 When apixaban was administered post-HD, Cmax was decreased by 10%, but AUC was increased by 36% compared to non-HD patients. Although patients on HD may be at higher risk for bleeding due to heparin exposure during HD and a higher level of Von Willebrand factor, HD may offset the temporarily elevated AUC from post-HD dosing. Therefore, it may not be necessary to dose adjust in this population.
Drug Interactions
The apixaban package labeling advises on the importance of drug interactions, as apixaban is a substrate of both cytochrome P450 3A4 (CYP3A4) and efflux transporter permeability-glycoprotein (P-gp). Co-administration of strong CYP3A4 and P-gp inhibitors or inducers may result in increases or decreases of apixaban exposure, respectively. 9,10 Apixaban should not be used with dual strong CYP3A4 and P-gp inducers, such as rifampin, carbamazepine, phenytoin, and phenobarbital. 11,12 Concomitant dual strong CYP3A4 and P-gp inhibitors should also be avoided or a 50% dose reduction is recommended when concurrent use is needed. 1 CYP3A4 inhibitors and inducers are thought to have a more significant drug interaction with apixaban compared to those of P-gp. With commonly used cardiology medications that are CYP3A4 inhibitors, such as amiodarone, verapamil, or diltiazem, there appear to be no clinically significant interactions. 12
Overall, pharmacokinetic data support the idea that apixaban plasma concentrations are affected by each of the NVAF dose adjustment criterion; however, the cutoffs do not appear to be consistent with those currently recommended by the manufacturer. Next, we will dive into the available clinical data focusing on subgroups of age, weight, and renal function.
Review of Clinical Trial Data as It Pertains to Apixaban Dose Adjustment Criteria
AVERROES randomized 5,599 patients with NVAF to standard dose apixaban or aspirin 81-324 mg per day. The dose adjustment criteria for reduced dose apixaban was applied. Apixaban users had significantly fewer stroke events, with no difference in major bleeding. Subgroup analyzes evaluating age and renal function, including patients ≥75 years and eGFR <50 mL/min found no significant interactions. 13
ARISTOTLE was a double-blind, randomized trial that compared apixaban to warfarin in 18,201 patients with NVAF. Stroke events and death from any cause occurred significantly less in the apixaban group compared with warfarin. Subgroup analyzes demonstrated consistent efficacy and safety with apixaban among patients age
A secondary analysis of ARISTOTLE evaluated standard dose apixaban in patients meeting 1 dose-reduction criterion versus none.
16
Among 3,966 patients with only 1 dose-reduction criterion, 41.3% were
To evaluate apixaban use for the treatment of acute VTE, 2,691 patients were randomized to receive 10 mg of apixaban twice daily for the first 7 days, then subsequently 5 mg twice daily or enoxaparin at a dose of 1 mg/kg subcutaneously twice daily for 5 days bridging to warfarin for 6 months.
19
Fixed-dose apixaban was non-inferior to conventional therapy with enoxaparin for the treatment of acute VTE and significantly reduced major bleeding. Again, the effect of apixaban on each outcome did not differ within subgroups of age, weight, or renal function though <5% of patients were >75 years of age, 231 (8.6%) weighed
Apixaban Renal Dose Adjustment
Most renal dosing recommendations are based on calculated CrCl using the Cockcroft-Gault formula, and limited drugs utilize eGFR for dosing. Interestingly, the apixaban renal dose adjustment recommendation is based on SCr, and is the only drug on the market with such dose adjustment criteria. While the most accurate and reliable index of kidney function for drug dosing is still debated, SCr is not a reliable indicator of renal function because it requires stable kidney function and can be confounded by muscle mass, age, race, gender, and tubular secretion. It is not clear why apixaban is dose adjusted based on SCr instead of CrCl or estimated GFR.
All trials leading to apixaban approval excluded patients with SCr >2.5 mg/dl or CrCl <25 mL/min. Apixaban is excreted in both feces and urine as metabolites (27% of total clearance). 5 Thus, in patients taking apixaban with renal impairment, less drug clearance may cause more anticoagulant effects and a higher risk of bleeding; however, this was not seen clinically. 17 Additional literature challenges the role of renal impairment for apixaban dosing. 21 –23
An inpatient retrospective cohort study compared apixaban (n = 73) to warfarin (n = 73) in patients with severe renal impairment (CrCl of <25 mL/min or SCr of >2.5 mg/dL), including patients on peritoneal dialysis (n = 4) or HD (n = 38). 22 Patients receiving continuous renal replacement therapy (CRRT) were excluded. Indications for apixaban included NVAF (72.6%) and VTE (26%). Approximately 62% received the reduced dose of apixaban 2.5 mg twice daily, 37% received apixaban 5 mg twice daily, and 1.4% received apixaban 10 mg twice daily. No statistically significant differences were seen for bleeding or stroke/systemic embolism. Seven of 39 patients who were taking apixaban before admission were taking an inappropriate dose (e.g. dose reduction for VTE treatment).
Another retrospective cohort study compared the safety and efficacy of apixaban vs warfarin in dialysis patients. 21 Patients with acute kidney injury and those on CRRT were excluded. Among inpatient end-stage renal disease (ESRD) patients (n = 124) on peritoneal dialysis or HD who received apixaban (n = 74) or warfarin (n = 50), 34 (46%), 29 (39.2%) and 11 (14.9%) patients received apixaban for VTE, NVAF, and prophylaxis of VTE, respectively. Almost 80% of patients were on the standard apixaban dose for either VTE treatment or NVAF, while the remaining patients were on the reduced apixaban dose (20.3%) and met criteria for either dose reduction (n = 4) or lifelong prophylactic anticoagulation dosing (n = 11). Apixaban users had a non-significantly lower VTE recurrence rate and significantly fewer bleeding events compared to warfarin users. Thus, standard dose apixaban appears to be safe and effective in patients with ESRD on dialysis.
A larger retrospective cohort study evaluated the safety and effectiveness of standard dose apixaban (n = 1,034) versus reduced apixaban dose (n = 1,317) in ESRD patients on dialysis for NVAF only. 23 Only the standard dose apixaban was associated with a significantly lower risk of stroke or systemic embolism compared to warfarin. Both apixaban doses showed a significantly greater reduction in major bleeding compared to warfarin. Notably, standard dose apixaban demonstrated greater reduction in thromboembolic events and mortality in ESRD patients compared to the reduced apixaban dose suggesting again that standard dosing of apixaban is safe in these patients.
These studies of apixaban in renal impairment demonstrated the safety of apixaban use in this population compared to warfarin. 21 –23 Importantly, when compared with reduced dose apixaban, standard dose apixaban not only significantly reduced the stroke rate, but was also associated with reduced mortality. 23 Overall, it appears that apixaban dose adjustment for severe renal impairment, including those on dialysis, may not be necessary and available literature suggests that SCr or CrCl should not be considered for dose adjustment.
More recently, a retrospective cohort study was conducted in patients with NVAF and ESRD on dialysis. Interestingly, compared to no anticoagulation, apixaban use was not associated with a lower rate of stroke or systemic embolism (HR 1.24, 95% CI 0.69 to 2.23), but was associated with a higher rate of fatal or intracranial bleeding (HR 2.74, 95% CI 1.37 to 5.47). 24 This study suggests that apixaban use in this patient population should be re-evaluated to determine the net clinical benefit.
Real-World Apixaban Dosing
A retrospective cohort study of 27 patients who received apixaban 2.5 mg twice daily for VTE treatment (15%) and for NVAF or atrial flutter (85%) was conducted. 25 More than half of the patients had 1 dose-reduction criterion leading to a manufacturer-recommended dose adjustment adherence rate of about 10% in NVAF patients. Most of the adjustments were made due to history of bleeding, renal dysfunction, and concomitant medications such as nonsteroidal anti-inflammatory drugs or other agents that increase bleed risk. In contrast, in a multicenter trial, 420 patients were given standard dose apixaban, and 136 received reduced dose apixaban for NVAF. 2 Adherence to apixaban dosing recommendations per the manufacturer was 87%, illustrating the variability in adherence to manufacturer-recommended dose adjustment in real life. Reasons for deviating from the manufacturer-recommended dose were continuation of home dose (38.9%), perception of increased bleeding risk (25%), unspecified (20%), history of gastrointestinal bleeding (5.6%), dosing error (5.6%), and anticipated need for dose-reduction in the future (4.2%). It seems that lower-than-recommended dosing is clinician-specific and not standardized.
When dosed according to the package labeling, some have identified large overlap in plasma apixaban levels between those receiving 5 mg twice daily and those reduced to 2.5 mg twice daily dosing, suggesting appropriateness of dose adjustment criteria, even among those deemed to be at high-risk for bleeding. 26,27 However, those receiving the lower dose off-label had median trough apixaban levels almost half that of patients receiving the lower dose according to manufacturer recommendations (66 vs 102 ng/ml, P = 0.014). 26 The clinical relevance of decreased apixaban exposure in those receiving the lower dose off-label remains uncertain. To capture real-world data on use of lower doses, a Danish database included 88,141 patients of which 69.9% of patients received warfarin, 7.9% received apixaban 2.5 mg twice daily, 15.9% received dabigatran 110 mg twice daily, and 6.3% received rivaroxaban 15 mg daily. 28 In contrast to the previous trials, patients receiving apixaban demonstrated a trend toward increased ischemic stroke and no difference in bleeding when compared to warfarin. However, patients receiving apixaban were older (mean age 83.9 vs. 73.9 years) with more comorbidities and higher mean scores for CHA2DS2-VASc (4.3 vs. 3.3) and HAS-BLED (2.8 vs 2.4). Sensitivity analyzes of cohorts with an indication for dose reduction and patients ≥80 years of age showed reduced bleeding, but did not differ from an efficacy standpoint. With the lack of reporting on weight or SCr, it remains difficult to assess whether the dose adjustment criteria are clinically necessary, though it is plausible that 2.5 mg may be too low of a dose for adequate stroke prevention.
Conclusion
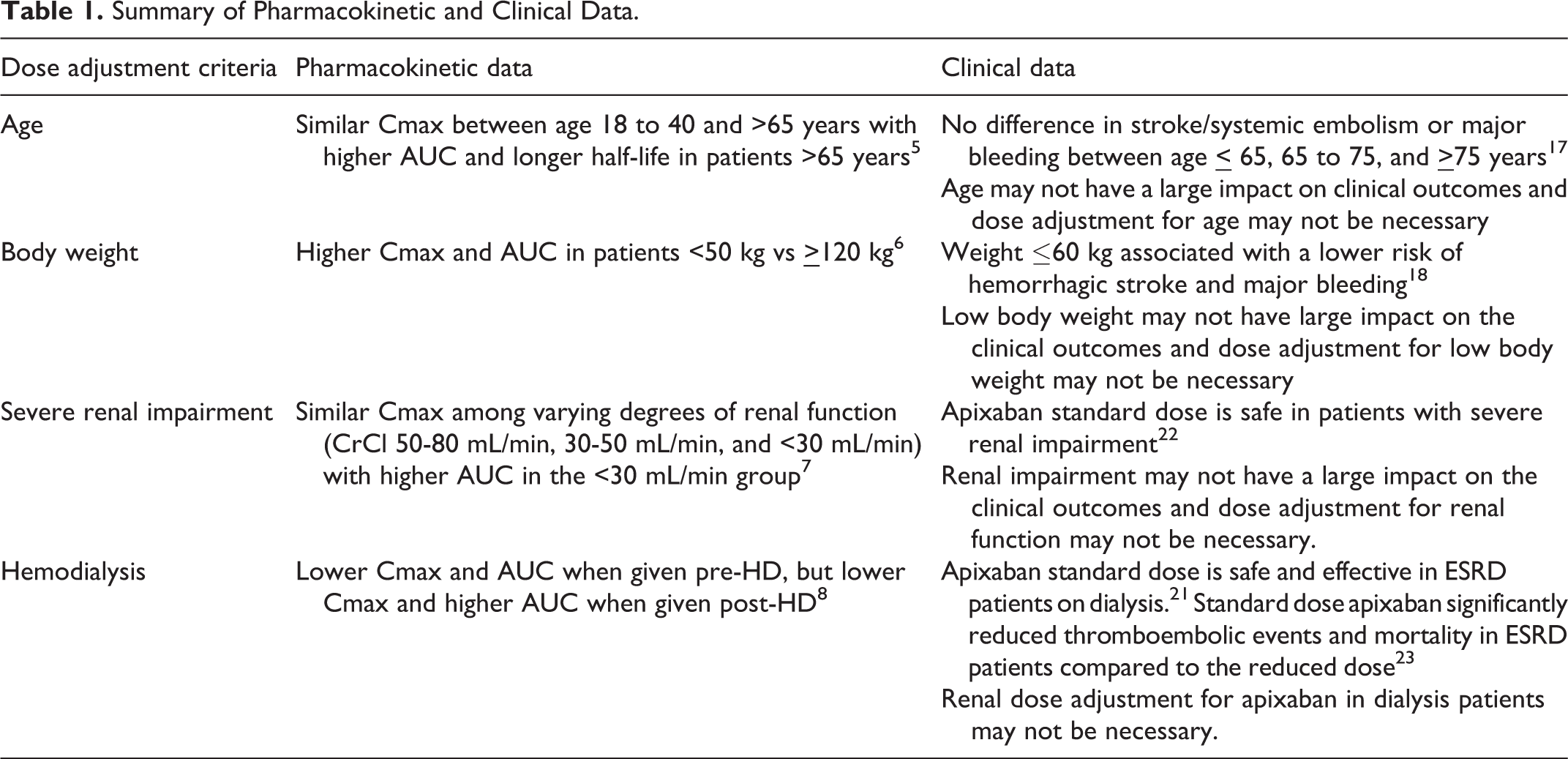
Dosing apixaban can be complicated and the appropriateness of its dose adjustment criteria remains unclear. Current package labeling generally recommends reduced-dose apixaban based on older age, lower weight, and higher SCr, and only when prescribed for NVAF. The rationale provided by the manufacturer is that patients with these characteristics are anticipated to have higher apixaban drug exposure. 15 After a thorough literature review including both PK and clinical data, the clinical relevance of applying such criteria requires additional analysis (summarized in Table 1), and is difficult to evaluate given the discordance between dose adjustment criteria and reported cut-points within studies. In real-world utilization, the dose may be reduced in patients presumed to have a higher bleeding risk and this is not standardized in clinical practice. Though renal function may not be a relevant criterion for dose adjustment, the net clinical benefit of anticoagulation in HD patients must be re-examined. Overall, the clinical significance of dose reducing apixaban may require further investigation and confirmation in well-designed randomized controlled trials.
Summary of Pharmacokinetic and Clinical Data.
While apixaban fixed dosing is advantageous, there is clear need for improvement from the standpoint of criteria for dose adjustment. As we continue to learn more about what role certain criteria or specific drug interactions play in the dosing of apixaban, we can optimize dosing for each patient. We are also still learning about the role of coagulation test monitoring as there are limited data evaluating anti-FXa assays and the association with clinical outcomes. 29 –32 The lack of routine monitoring is another benefit to using DOACs and perhaps there are certain criteria that warrant closer monitoring, but the therapeutic index of DOACs has yet to be fully elucidated. When these aspects are clear, we will be able to individualize and optimize apixaban therapy.
Footnotes
Authors’ Note
Our institution did not require ethical approval. Informed consent for patient information to be published in this article was not obtained because human subject research was not conducted for this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.