
Abstract
Heparin-induced thrombocytopenia (HIT) and heparin-induced thrombocytopenia with thrombosis (HITT) are rare but potentially limb- and life-threatening complications of heparin therapy. Continuation of heparin or low-molecular-weight heparin is contraindicated due to platelet activation in the presence of (heparin-dependent) HIT antibodies. Primary treatment options currently include argatroban, fondaparinux, or bivalirudin. However, the parenteral administration routes and interference of argatroban with traditional coagulation markers complicate management. The goal of this review is to assess the viability of direct oral anticoagulants as an alternative treatment option in patients with HIT/HITT. Their use in HIT/HITT is reasonable, given absent cross-reactivity preformed with HIT antibodies. Furthermore, their rapid onset of action and induction of effective anticoagulation provide a favorable basis for their use in this condition. Herein, we summarize 3 studies and 8 case reports comprising 56 patients in whom direct oral anticoagulants were used in the treatment of HIT/HITT.
Keywords
Introduction
Heparin-induced thrombocytopenia (HIT) is an immunologic drug reaction capable of inciting an intensely prothrombotic state and occurs in up to 4.9% of patients treated with unfractionated heparin (UFH). 1 This risk is modified based upon patient category (surgical > medical), UFH source (bovine > porcine), sex (female > male), and is lower with low-molecular-weight heparin (LMWH). 2 For instance, HIT occurs among 1% of hospitalized patients receiving heparin and 4.8% and 0.6% of orthopedic surgery patients receiving postoperative UFH and LMWH, respectively. 3 Pathologic antibodies directed against a Platelet Factor 4 (PF4)-heparin neoepitope bind and activate FcγIIa receptors located on platelets and monocytes. 4 Further enhanced by endothelial cells, the activation of platelets and monocytes increases thrombin generation. 5 Increased activation of thrombin and platelet causes clinical problems. Testing provides additional diagnostic information and generally comes in the form of antigen assays, which detect potentially pathologic antibodies, and functional assays, which detect platelet activation in the presence of patient sera. 6 Calculation of the HIT 4Ts (i.e., degree of Thrombocytopenia, Timing of thrombocytopenia vs heparin, Thrombosis, and other causes of Thrombocytopenia) score aids in the decision to convert to therapeutic doses of a nonheparin-based anticoagulant, 7,8 which typically needs to be done prior to availability of laboratory test results due to the high rate of thrombosis among untreated patients. HIT can be associated with devastating thromboembolic complications, including pulmonary embolism (PE), ischemic limb necrosis necessitating limb amputation, acute myocardial infarction, and stroke. 9
Historically, treatment has proceeded with a parenteral direct thrombin inhibitor such as argatroban. Once the platelet count has stabilized, the patient can be bridged to warfarin and thromboses treated typically for 3 to 6 months. 8 Due to its “niche” indication for use in HIT, argatroban is infrequently used by clinicians, making dosing and monitoring requirements more challenging. Even the appropriate monitoring of argatroban can potentially lead to treatment failure, as HIT-associated coagulopathies may lead to misinterpretations of Partial Thromboplastin Time (PTT) monitoring (a problem known as “PTT confounding”), resulting in inaccurate dosage adjustments. 10,11 For example, one report described an HIT-positive patient with a pretreatment PTT range of 38 to 41 seconds who was treated with agartroban. 10 After treatment initiation, the PTTs rose to more than 100 seconds, prompting treatment reduction and interruption. This patient subsequently died of ischemic stroke as a result of HIT progression. A treatment strategy that does not rely on PTT (or other laboratory) monitoring, such as direct oral anticoagulant (DOAC) therapy, should avoid this important limitation of argatroban therapy.
However, even in the setting of strict monitoring of argatroban, the HIT-mediated thrombophilia may remain quite intractable. This was borne out in the original argatroban clinical trials, ARG-911 and ARG-915, representing historically controlled prospective studies. Both trials used the same historical control group of patients with HIT and HIT-associated thrombosis (HITT), in whom the rates of a composite primary end point comprising all-cause death, all-cause amputation, or new thrombosis were 38.8% and 56.5%, respectively. 12,13 The ARG-911 study demonstrated that the primary composite end point still occurred in 25.6% of patients with HIT (hazard ratio [HR] 0.60, 95% confidence interval [CI] 0.40-0.89, P = .010) and 43.8% of patients with HITT (HR 0.57, 95% CI 0.36-0.90, P = .014). Similarly, the ARG-915 showed the occurrence of primary end points in 28.0% (patients with HIT; HR 0.64, 95% CI 0.43-0.93, P = .02) and 41.5% (patients with HITT; HR 0.56, 95% CI 0.36-0.85, P = .008). This may be related to high rates of premature treatment discontinuation of argatroban or absence of longer-term anticoagulation in the ARG-911 and ARG-915 studies—10% and 13%, respectively. 14
The American College of Chest Physicians provide evidence-based guidelines for management of forward anticoagulation in patients with acute HIT or HITT. 15 Currently, oral anticoagulation with vitamin K antagonist (VKA) therapy for a minimum period of 4 weeks in isolated HIT and 3 months in HITT is recommended. 15 Premature transition to VKA therapy is not recommended due to significant risk of warfarin-induced skin necrosis or development of venous limb gangrene. 15 Most clinicians transition to oral warfarin when the platelet level reaches 150 × 109/L.
Avoidance of a VKA mechanism of action and favorable pharmacokinetic profiles therefore support immediate or bridged introduction of a DOAC as an option for HIT. The DOACs are currently approved for prophylaxis and treatment of VTE and for reduction of stroke risk in nonvalvular atrial fibrillation. 16 Rapid onset of action of these agents represents a favorable pharmacokinetic attribute. 17 Recently, there has been a growing number of case reports and studies in the medical literature supporting the use of DOACs as primary or secondary treatment of HIT. Given the emergence of this off-label use of DOACs, we conducted a literature review to gain additional insight into the use of DOACs for treatment of HIT.
Preclinical Rationale for Management of HIT With DOACs
Unlike heparin, DOACs do not interact and complex with PF4 and are not recognized by preexisting HIT antibodies. Walenga et al demonstrated that apixaban did not interact with preformed HIT antibodies as determined by 14C-serotonin assay (serotonin release assay [SRA]), similar to fondaparinux. 18 As a result, platelet aggregation was not observed by platelet aggregation assay. 18 Similarly, dabigatran and rivaroxaban did not cause any platelet activation in the presence of HIT antibodies even at therapeutic concentration as demonstrated by the absence of platelet microparticle formation and platelet P-selectin upregulation. 19,20 Furthermore, they did not interact with PF4 and had no effect on antibody binding to PF4/heparin complexes as indicated by its unchanged anti-FXa activity before (control) and after incubation with purified PF4. 20 In contrast, the antithrombin activity of heparin and anti-FXa activity of enoxaparin was decreased by 43% and 23%, respectively, relative to the control. 20 These preclinical data provide rationale for treatment of HIT with DOACs.
Clinical Experience in Management of HIT With DOACs
A total of 56 reported cases of patients with HIT/HITT treated with DOACs were found, which included 12 patients from a prospective study, 34 patients from 2 case series, and 10 patients from case reports (Tables 1 and 2). Mean (range) age was 70 (46-87). Among the 44 patients in whom gender was reported, 61% were male. Thirty-two (57%) patients had HIT-related thrombosis (HITT). At the time of HIT/HITT diagnosis, a nonheparin parenteral agent was initiated in 42 (75%) of 56 patients. Among these 42 patients, the initial parenteral choice was argatroban in 28 (67%), bivalirudin in 6 (14%), fondaparinux in 7 (17%), and danaparoid in 1 (2%). Of the total 56 reported, rivaroxaban, apixaban, and dabigatran were utilized in 54%, 29%, and 18% of cases, respectively. The cumulative duration of DOAC follow-up represented by 54 of 56 patients for whom it was reported was 4587.25 person days. There were 2 (4%) instances of recurrent thrombosis with DOAC therapy, yielding an incidence of 0.43/1000 person days. 21 Platelet count recovery was documented in 55 (98%) of 56 patients. In the 1 (2%) case where the platelet count did not recover, the patient ultimately died of metastatic gastric cancer at day 21. 21 Major bleeding occurred in 3 patients who did not appear to be on DOAC therapy at the time of bleed. 21,22 The reviewed literature is summarized in Tables 1 and 2.
Summary of Prospective and Retrospective Series on DOACs in HIT/HITT.
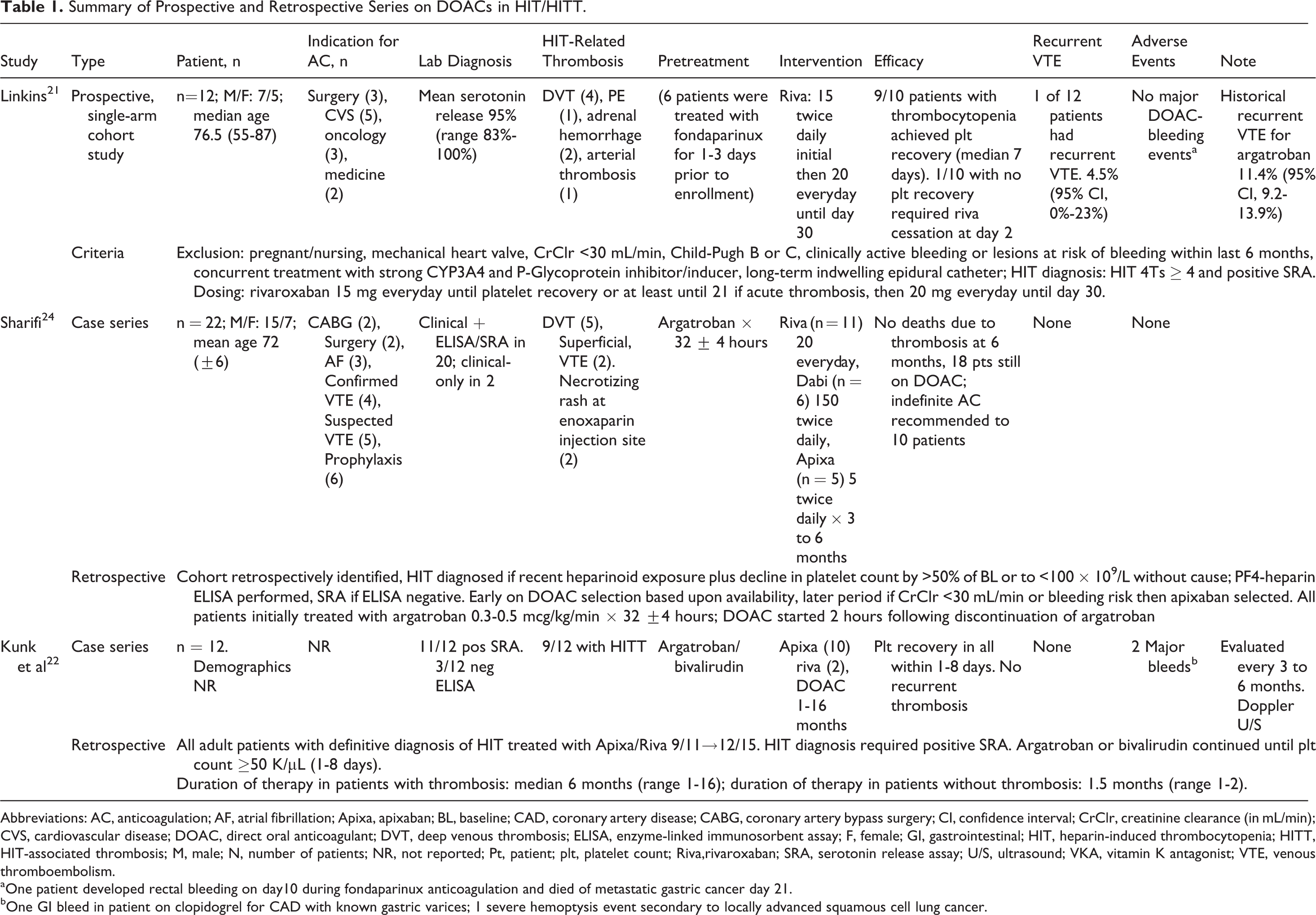
Abbreviations: AC, anticoagulation; AF, atrial fibrillation; Apixa, apixaban; BL, baseline; CAD, coronary artery disease; CABG, coronary artery bypass surgery; CI, confidence interval; CrClr, creatinine clearance (in mL/min); CVS, cardiovascular disease; DOAC, direct oral anticoagulant; DVT, deep venous thrombosis; ELISA, enzyme-linked immunosorbent assay; F, female; GI, gastrointestinal; HIT, heparin-induced thrombocytopenia; HITT, HIT-associated thrombosis; M, male; N, number of patients; NR, not reported; Pt, patient; plt, platelet count; Riva,rivaroxaban; SRA, serotonin release assay; U/S, ultrasound; VKA, vitamin K antagonist; VTE, venous thromboembolism.
aOne patient developed rectal bleeding on day10 during fondaparinux anticoagulation and died of metastatic gastric cancer day 21.
bOne GI bleed in patient on clopidogrel for CAD with known gastric varices; 1 severe hemoptysis event secondary to locally advanced squamous cell lung cancer.
Reported Cases of DOAC Use in HIT/HITT.
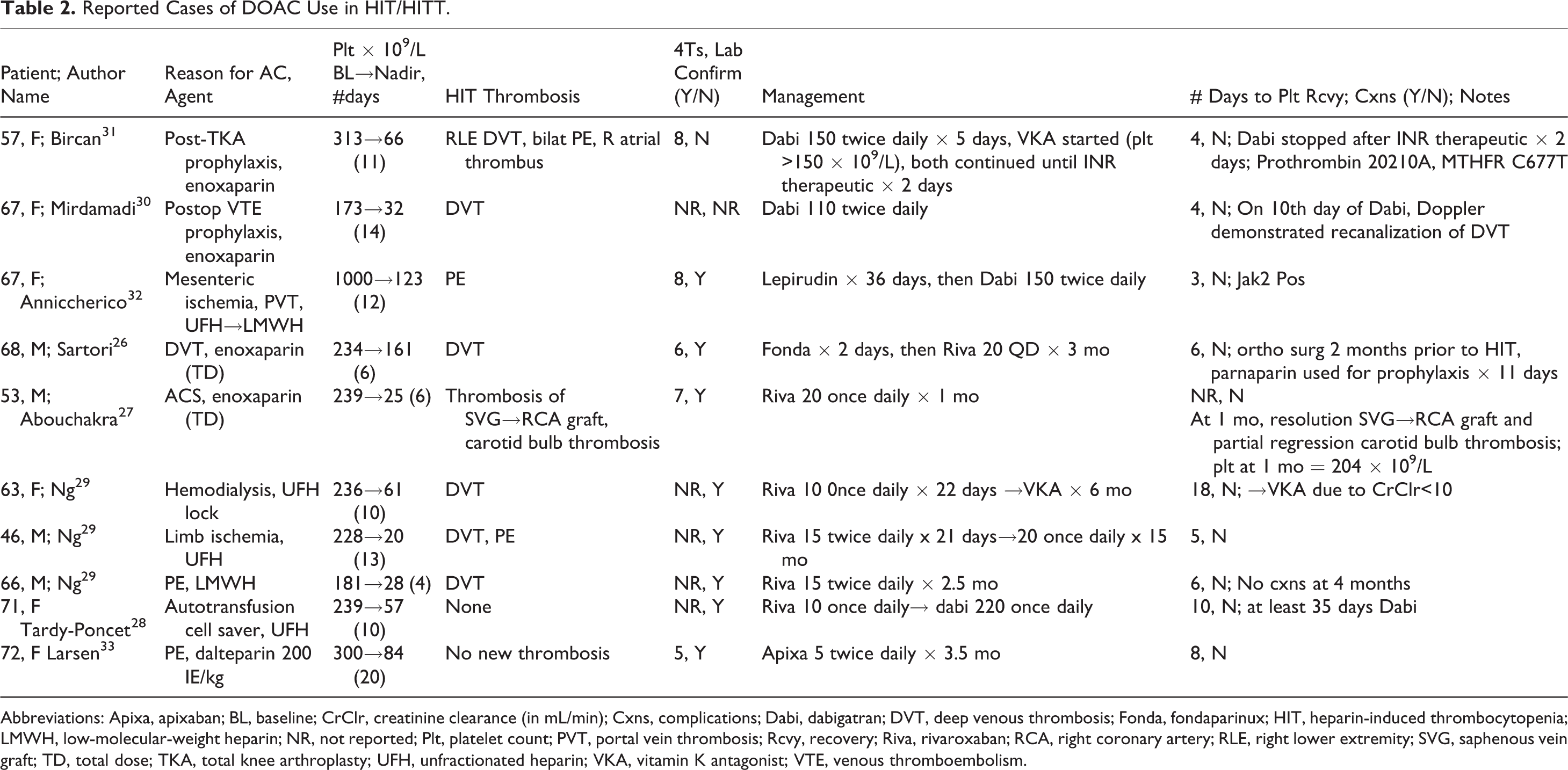
Abbreviations: Apixa, apixaban; BL, baseline; CrClr, creatinine clearance (in mL/min); Cxns, complications; Dabi, dabigatran; DVT, deep venous thrombosis; Fonda, fondaparinux; HIT, heparin-induced thrombocytopenia; LMWH, low-molecular-weight heparin; NR, not reported; Plt, platelet count; PVT, portal vein thrombosis; Rcvy, recovery; Riva, rivaroxaban; RCA, right coronary artery; RLE, right lower extremity; SVG, saphenous vein graft; TD, total dose; TKA, total knee arthroplasty; UFH, unfractionated heparin; VKA, vitamin K antagonist; VTE, venous thromboembolism.
Rivaroxaban
Of the approved DOACs, rivaroxaban has become the most studied for HIT treatment. Linkins et al conducted a multicenter, single-arm, prospective cohort study of patients with suspected or confirmed HIT to evaluate the efficacy and safety of rivaroxaban (Table 1). 21 About 527 patients were screened for the study and 22 enrolled. The most common reasons screened patients did not proceed to enrollment were HIT 4Ts score <4 (n = 325) and creatinine clearance <30 mL/min (n = 131). Of the 22 enrolled, HIT was ultimately excluded by negative SRA in 10, leaving 12 patients in the final study group, with a mean serotonin release of 95% (range 83%-100%). 21 The planned sample size of 200 was based upon previous data supporting that confirmation of HIT by SRA will ensue in 6% of patients in whom HIT is suspected, thus allowing a final sample of 10 to 30 patients with confirmed HIT. 23 Poor enrollment led to early discontinuation of the study, and available data were reported.
Among the 12 participants, 10 patients had thrombocytopenia and 6 had HIT-associated thrombosis at the time of study. Seven patients were treated with either fondaparinux or danaparoid for 1 to 3 days, and 5 patients were immediately started on rivaroxaban. Nine of 10 patients with baseline thrombocytopenia achieved platelet recovery, with mean and median times to recovery of 11 and 7 days, respectively. 21 In this study, 11 of the 12 patients had resolution of HIT-related thrombosis. One HIT-positive participant had symptomatic recurrent venous thromboembolism (VTE) presenting as extension of a previously diagnosed, apheresis catheter-related thrombosis. The authors note that a repeat ultrasound was not performed at study entry, so the possibility exists that the thrombus extension preceded initiation of rivaroxaban—the catheter was removed, rivaroxaban continued, and complete resolution of symptoms and thrombocytopenia ensued. Although not considered as a recurrent thrombosis on DOAC by the authors, one patient developed acute ischemia requiring bilateral amputation—to be conservative, we have added this to the total tally of recurrent thrombotic events. None of the patients in the current study experienced any major bleed while on rivaroxaban. Four patients died of non-HIT-related causes (sepsis, end-stage chronic obstructive pulmonary, and gastric cancer). 21 The results of this study suggest that DOACs were effective in patients with HIT regardless of whether they were started immediately or first bridged with an alternate agent.
In a retrospective study of 22 patients with HIT, 11 were treated with rivaroxaban 24 (Table 1). The diagnosis of HIT required history of recent exposure to heparin products and a >50% decline in platelet count or to <100 × 109/L without other explainable causes. With suspicion of HIT, all heparin products were discontinued and argatroban initiated, with DOAC (apixaban if CrClr < 30 mL/min) started 2 hours after argatroban discontinuation. 24 Ultimately, 20 of 22 patients had additional confirmation of HIT diagnosis with positive enzyme-linked immunosorbent assay (ELISA) or SRA; in 2 of 22, therefore, the diagnosis was solely clinical. The number of patients with positive SRA was not reported in this study. It is known that for patients having positive ELISA without SRA, about 50% of ELISA+ patients probably do not have true HIT. 25 Five of 22 had new deep venous thromboses. Superficial vein thromboses were detected in 2 additional patients. All patients received a short course of argatroban (mean of 32 ± 4 hours) prior to initiation of DOACs. Eleven patients received rivaroxaban, 6 patients received dabigatran, and 5 patients received apixaban. The mean platelet levels at baseline, nadir, and day of discharge were 168.8 ± 87.1 × 109/L, 82.1 ± 38.6 × 109/L, and 188.4 ± 52.5 × 109/L, respectively. At 19 months of follow-up, 6 patients had died of nonthrombotic causes. By 6 months, 18 patients were still on DOAC therapy. There were no bleeding or recurrent VTE events in any patient. 24 Although the retrospective nature of the study did not allow for the same degree of diagnostic certainty for HIT as in Linkins et al, 21 platelet recovery and absence of recurrent thromboses or bleeding support its efficacy and safety.
Multiple case reports provide further evidence to support the role of rivaroxaban in HIT management 26 –29 (Table 2). Sartori et al reported the case of a 68-year-old male with recent orthopedic procedure who came to the ED for suspected lower extremity deep venous thrombosis (DVT). He received weight-based enoxaparin but developed thrombocytopenia 6 days later. His 4Ts score was 6, and an immunoglobulin G (IgG)-specific ELISA was positive (Optical Density = 1.548). The presence of HIT was confirmed by a heparin-induced platelet aggregation (HIPA) test (52% with 1 IU/mL UFH). After enoxaparin discontinuation, the patient was treated with fondaparinux for 2 days prior to initiation of rivaroxaban. He completed a total of 3 months of anticoagulation therapy with no bleeding or recurrent thrombotic complications. Other case reports are summarized in Table 2.
Dabigatran
The data for dabigatran in the treatment of HIT are less robust than rivaroxaban but supportive. Of the 22 patients evaluated by Sharifi et al, 6 patients were treated with dabigatran. 24 The study did not specify the outcome of patients who were taking dabigatran. However, no patients had recurrence of thrombosis or bleeding, suggesting that dabigatran was efficacious.
Mirdamadi described a 67-year-old woman who developed HIT-related DVT from enoxaparin prophylaxis about 2 weeks after orthopedic surgery. 30 Her platelet count decreased from 173 × 109/L at baseline to 32 × 109/L at nadir. She was started on dabigatran 110 mg twice a day by mouth, with resolution of thrombocytopenia in a few days and canalization of thrombosis after 10 days. Bircan et al reported a 57-year-old Turkish female who received 11 days of prophylactic enoxaparin after knee replacement. 31 She presented to the hospital with a massive pulmonary embolism (PE) with right ventricular strain. She also had associated atrial thrombus and DVT. Thrombophilia workup was positive for heterozygous mutations for both prothrombin 20210A and methylenetetrahydrofolate reductase (MTHFR) C677T. Her platelet count decreased to 66 × 109/L from a baseline count of 313 × 109/L. She was diagnosed with HIT based on a 4Ts score of 8 and started on dabigatran 150 mg twice daily. Thrombocytopenia improved within days and upon achieving a count of 150 × 109/L was bridged to warfarin. Although the long-term outcome of this patient is unknown, this case demonstrates rapid clinical improvement with dabigatran even in the setting of hypercoagulable state (HIT, prothrombin 20210A, and MTHFR). In another case report, dabigatran treatment was associated with rapid reversal of HIT-related thrombosis in a patient with essential thrombocythemia. 32
Tardy-Poncet and colleagues present an interesting case of a patient with remote (>100 days) heparin exposure who developed thrombocytopenia upon exposure to heparinized autotransfusion product during orthopedic surgery; there were no other heparin exposures. 28 Postoperative thromboprophylaxis was initiated with daily rivaroxaban (10 mg) started 8 hours following wound closure after right knee replacement and continued through day 21. Baseline platelet count was 239 × 109/L falling to 57, 56, and 58 × 109/L by days 17, 18, and 20, respectively. Because the platelet count was failing to rise, rivaroxaban 10 mg daily was converted on day 21 to daily dabigatran (220 mg), with platelet count improvement to 100 × 109/L by day 27 (dabigatran day #6), 140 × 109/L by day 31 (dabigatran day #10), and 150 × 109/L by day 35 (dabigatran day #14). The authors did not specify the reason for dabigatran switch, which was presumably due to the concern of persisting HIT in the presence of rivaroxaban. However, the patient was only on the prophylactic dose of rivaroxaban, and increasing rivaroxaban to the therapeutic dose could theoretically lead to HIT resolution. It is unclear as to why the prophylactic dose of dabigatran was effective in this case.
Apixaban
Retrospective data suggest safety and efficacy of apixaban in HIT management. As discussed earlier, 5 of 22 patients in Sharifi et al were on apixaban, and no patients in the study had recurrence of thrombosis or bleeding complications. 24 In a retrospective study of 12 patients in whom clinical HIT was confirmed by SRA, 10 patients were transitioned to apixaban (and 2 to rivaroxaban) after platelet recovery (to >50 × 109/L) on initial treatment with argatroban or bivalirudin (Table 1). 22 Seven patients with thrombosis were on apixaban for a median of 6 months (range 2-13 months), whereas the 3 patients without thrombosis were treated with apixaban for median of 1.5 months (range 1-2 months). 22 There were no recurrent thromboses, but 1 patient on apixaban had major gastrointestinal hemorrhage leading to therapy discontinuation. Of the remaining 9 patients, safe and effective anticoagulation with apixiban was noted for up to 16 months without adverse effects. The authors concluded that DOACs provide safe and effective outpatient anticoagulation for patients with HIT but that further prospective studies are needed before they could be accepted as standard of care.
A 72-year-old female undergoing treatment for metastatic pulmonary adenocarcinoma developed acute pulmonary embolism and was treated with dalteparin 200 IE/kg.
33
A decline in platelet count from baseline >200 × 109/L to 84 × 109/L by day 20 and HIT 4Ts score of 5 raised suspicion for HIT. Dalteparin was continued for an additional several days until confirmatory tests returned: heparin-PF4 ELISA “highly positive” and positive HIPA. At that point, she was switched over to apixaban 5 mg twice daily. The patient experienced clinical improvement after 3 days and reported no adverse reactions to the treatment. Platelets rapidly increased and
Discussion
The DOACs present a promising alternative for the management of HIT/HITT. Preliminary evidence from our review of the literature provides support for this treatment avenue. Currently, there are no randomized controlled data that support the role of DOACs in the management of HIT/HITT, and randomized controlled trials have proven difficult to conduct in HIT given its rarity. 34 Heparin-induced thrombocytopenia may be confirmed in only 6% of those in whom it is initially suspected. 23 Even when pretest probability is increased through the use of 4Ts scoring, less than a quarter of patients with 4Ts score >4 will have a positive 14C SRA. 7
Our review of the literature uncovered only a single prospective study, which was discontinued prematurely due to poor enrollment. 21 Nonetheless, power analysis confirmed that an acceptable number of patients were enrolled, allowing the authors to conclude that rivaroxaban appeared effective for patients with confirmed HIT. Two other studies comprising 34 patients were retrospective in nature. 22,24 The remainder were comprised of case reports. 26,28 –30,33 Reporting bias is therefore a concern.
There was some variability in the rigor required for HIT diagnosis. Some studies required confirmatory SRA testing, whereas others allowed ELISA-based testing combined with clinical criteria. A minority of patients were diagnosed solely on clinical grounds. Although this may reduce scientific validity, it is fairly representative of real-world conditions and therefore should not necessarily be considered a major detriment.
It remains unclear whether an initial parenteral treatment course is necessary. We observed that 75% of reviewed courses included a parenteral treatment phase. The overall efficacy of a 5- to 6-day course of intravenous argatroban in the ARG 911 and ARG 915 trials did not appear to provide absolute protection against recurrent thromboembolism. However, the inpatient setting often demands the flexibility afforded by bivalirudin (t½ [half-life]: 25-40 minutes) or argatroban (t½: 40-50 minutes). 35 The DOACs, on the other hand, have longer half-lives—with factor Xa inhibitors in the realm of 6 to 12 hours. Duration of effect is roughly comparable between dabigatran (t½: 12-17 hours) and fondaparinux (t½: 17-21 hours) and both require renal adjustment. 35,36 In 25% of observed reports, however, apparently effective anticoagulation was carried out with direct initiation of DOAC-based anticoagulation, even in patients with HIT and other hypercoagulable conditions such as prothrombin 20210A, MTHFR, Essential Thrombocytosis, and active malignancy. 31 –33 As studied in clinical trials and recommended in their respective package inserts, a lead-in period with parenteral anticoagulation is utilized during treatment of acute VTE with dabigatran or edoxaban. Conversely, rivaroxaban and apixaban trials did not employ a lead-in period with parenteral therapy. 37 These latter 2 agents may therefore be reasonable options for the management of HIT/HITTs and also represented the bulk of management options presented in our review (83%).
Compared to argatroban and bivalirudin, fondaparinux is subcutaneously dosed, thus allowing potential cost savings in the areas of reduced length of stay as well as overall drug costs. 38,39 The DOACs represent an additional nonparenteral option with similar potential benefits. As experience has grown with fondaparinux for HIT, off-label use has become fairly common. 40,41 We anticipate that the use of DOACs in HIT/HITT will follow a similar trend, particularly since the literature basis for fondaparinux is comprised predominantly of retrospective and case report-level data as opposed to prospective studies. 42
Additional study is required, however, to provide additional confidence in the safety and efficacy of DOACs in HIT/HITT. For example, would clinicians feel comfortable in the initial management of massive or submassive pulmonary embolism, limb-threatening arterial thrombosis, vena caval thrombosis, or cerebral thrombosis with DOAC therapy as opposed parenteral agents? In our review, a patient with HIT-related thrombosis of a coronary artery graft experienced resolution of this thrombus (as well as partial regression of a carotid bulb thrombosis) after 1 month of rivaroxaban therapy. 27 In another patient, however, extensive VTE comprising bilateral DVT, bilateral PE, and right atrial thrombus was managed only with a brief period of dabigatran prior to transitioning to warfarin. 31
The optimal duration of therapy with DOAC-based treatment for HIT/HITT is not known. Outside the prospective study environment, and excluding patients transitioned from DOAC to warfarin, we observed a 3-month median duration of therapy for patients receiving DOAC-based treatment of HIT/HITT. 22,26 –29,33 Furthermore, Sharifi et al reported safety and efficacy among 18 patients followed at least up to 6 months on extended DOAC-based therapy. 24 While the ideal duration remains unclear, current practices as well as ACCP Guidelines recommend at least 3 months of anticoagulation for patients with HIT-related thrombosis.
In terms of practicality, those using warfarin as longer-term management of HITT have available 4-factor prothrombin concentrate as an evidence-based reversal agent. 43,44 Currently, only dabigatran has an available target-specific antidote in the form of idarucizumab. 45 Although there is optimism for future approval of andexanet alfa as well as ongoing development of ciraparantag as reversal agents for the factor Xa inhibitors, 46 target-specific antidotes for these agents are as yet unavailable. This could represent an obstacle toward adoption of factor Xa inhibitors for off-label use. Keeping the limitations of available data in view, major bleeding events did not appear to be a major risk associated with DOAC therapy. If anything, HIT incites such an intense prothrombotic state that underanticoagulation would likely be of greater concern.
Footnotes
Authors’ Note
PNT performed the initial literature search and extracted relevant data, PNT and M-HT contributed equally to critical review of extracted data and to drafting and revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.