
Abstract
A growing researchers have suggested that fibrin monomer (FM) plays an important role in early diagnosis of thrombotic diseases. We explored the application of FM in the diagnosis and classification of acute ischemic stroke (AIS). The differences in FM, D-dimer, and NIHSS scores between different TOAST (Trial of ORG 10172 in Acute Stroke Treatment) types were analyzed with one-way ANOVA; the correlation between FM, D-dimer and NIHSS score in patients with different TOAST classification was analyzed by Pearson linear correlation. The ROC curve was utilized to analyze the diagnostic performance. 1. FM was more effective in diagnosing patients with AIS than D-dimer. 2. The FM level in cardiogenic AIS was significantly different from that in non-cardiogenic patients (P < 0.05); the NIHSS score in cardiogenic stroke was significantly higher than in atherosclerotic and unexplained stroke group. Whereas, no statistical difference was observed in the D-dimer level between these groups (P > 0.05). 3. The correlation between FM and NIHSS scores in the cardiogenic (r = 0.3832) and atherosclerotic (r = 0.3144) groups was statistically significant. 4. FM exhibited the highest diagnostic efficacy for cardiogenic AIS; furthermore, FM combined with the NIHSS score was more conducive to the differential diagnosis of cardiogenic and non-cardiogenic AIS. FM detection contributes to the early diagnosis of AIS, and is important for the differential diagnosis of different TOAST types of AIS. Moreover, FM combined with the NIHSS score is valuable in the differential diagnosis of cardiogenic and non-cardiogenic AIS.
Introduction
Acute ischemic stroke (AIS) is a type of brain tissue damage disease caused by insufficient cerebral blood supply due to cerebral arterial stenosis or blockage by thrombus. It is the most common type of stroke in clinical practice, with the characteristics of high incidence, rapid onset, high mortality and disability. Timely diagnosis and treatment of AIS is very important for patients with good prognosis and quality of later life. Therefore, both early diagnosis and individualized treatment are emphasized in worldwide treatment guidelines. Currently, the diagnosis of AIS mainly depends on the clinical manifestations of patients, neurological function tests, stroke scores, and imaging tests such as CT/MIR. In addition, platelet count, detection of coagulation routine, and D-dimer are of great significance for determining patients’ coagulation function status and guiding reperfusion therapy. 1 However, the underlying disease and the stage of AIS at the time of visit varies from patient to patient, and the patients with different etiology are treated differently (mechanical thrombectomy or intravenous thrombolysis, etc.). 2,3 Therefore, how to quickly identify the type of disease, assess the state of hypercoagulability, and personalize the intervention as soon as possible through better laboratory inspection is a challenge needs to be addressed.
Hemostatic unbalance is known to play a key role in pathophysiology of ischemic stroke. 4 A growing body of research have suggested that fibrin monomer (FM) plays an important role in early diagnosis of thrombotic diseases 5 –9 and its performance is better than traditional D-dimer. 10 –12 It has also been revealed the value of FM in etiological classification and prognosis of AIS. 13 In the present study, we investigated the level of FM in AIS patients with different TOAST classification and its correlation with National Institutes of Health Stroke Scale (NIHSS) score, and compared the diagnostic efficacy of FM with D-dimer. This study aims to provide more valuable means for the diagnosis and differential diagnosis of AIS.
Methods
Study Design and Population
A retrospective cohort approach was conducted on 162 AIS patients who were admitted to the Second Affiliated Hospital of Dalian Medical University from January 2018 to November 2019, aged between 40 and 92 years old, including 94 males and 68 females.
Inclusion criteria (refer to “China Guidelines for the Diagnosis and Treatment of Acute Ischemic Stroke 2018” 1 ): (1) aged over 18-year-old; (2) clinical symptoms and signs lasting more than several hours; (3) acute onset (admitted to hospital within 6 hours); (4) a clinical diagnosis of AIS; (5) clear new infarct lesions shown by MRI.
Exclusion criteria: (1) hemorrhagic cerebral infarction, cerebral parenchymal hemorrhage, or subarachnoid hemorrhage confirmed by CT; (2) severe heart, lung, liver and kidney dysfunction, tumor, and other serious underlying diseases; (3) focal symptoms caused by hypoglycemia, migraine with aura, epileptic seizure, multiple sclerosis and other diseases.
Information on NIHSS score and TOAST classification of the cases was available by reviewing the medical records. Among 162 AIS patients, 61 were atherosclerotic stroke, 55 were cardiogenic stroke, 30 were lacunar stroke, and 16 were unexplained stroke. In addition, blood samples and clinical data from 162 healthy subjects derived from the physical examination center were served as negative controls.
Sample Collection and Testing
The sodium citrate anticoagulant specimens from the first venous extraction of patients (before thrombolytic or mechanical thrombectomy) upon admission to the hospital were collected and centrifuged at 4,000 rpm for 10 min. Two to three milliliters of plasma were transferred to EP tubes and stored at −80°C for further testing.
Before detection, the plasma samples were placed in a water bath at 37°C for 15 min, and STA-R evolution automatic coagulation analyzer (Stago, France) was used for FM and D-dimer detection. All operations were performed in accordance with the manufacturer’s instructions of STA-Liatest FM (Stago, France) and D-dimer Kit (Shanghai SUNBIO, China). The detection limit of FM is 5 µg/ml and the assay working range is 5-150 µg/ml. The linearity range of D-dimer is 0.25-30 μg/ml and the clinical reportable range is 0-30 μg/ml. For samples whose test results were beyond the range reported by the instrument (FM > 150 μg/ml), the test was repeated after manual dilution with normal saline.
Statistical Analysis
The data normality test was performed using the K-S normal test. Data conforming to the normal distribution were expressed as mean ± standard deviation (x ± SD). The independent sample t-test was used for the comparison between two groups, one-way ANOVA followed by LSD post hoc was used for the comparison between multiple groups of measurement data, chi-square (χ2) test was used for comparison between multiple groups of counting data. Pearson linear correlation was used for correlation analysis. The Receiver Operating Characteristic (ROC) curve was applied to evaluate the diagnostic efficacy of FM and D-dimer for AIS, the diagnostic efficacy of FM for different TOAST types of AIS, and the diagnostic efficacy of different indicators for differential diagnosis of cardiogenic and non-cardiogenic AIS. The data were analyzed by SPSS 24.0 software, and P < 0.05 was considered statistically significant. GraphPad Prism 5.0 software was used to draw the graph.
Results
The Clinical Characteristics of AIS Patients
The clinical characteristics of different groups based on TOAST classification are shown in Table 1. Except that the proportion of stroke history in unexplained group was significantly lower than that in other groups (P < 0.05), there was no significant difference in baseline characteristics (age, gender) and underlying diseases (hypertension, diabetes, hyperlipidemia) between groups (P > 0.05).
Comparison of Clinical Characteristics in AIS Patients With Different TOAST Classification.

The Values present numbers (percentages). Statistical analyses were conducted using χ2 test.
*P < 0.05 compared with cardiogenic, atherosclerotic, and lacunar AIS groups.
Level of FM and D-Dimer in AIS Patients and Healthy Group
As shown in Figure 1, compared with the healthy group, the FM level of AIS patients (23.90 ± 35.16) was significantly higher than the healthy group (4.45 ± 1.10, P < 0.0001), as was the D-dimer level (1.05 ± 1.67; 0.45 ± 0.20, P < 0.0001).

Comparison of the level of FM and D-dimer between AIS patients and healthy group.
Diagnostic Efficacy of FM and D-Dimer for AIS
The sensitivity and specificity of FM and D-dimer in the diagnosis of 162 AIS patients are analyzed with ROC curve (Figure 2). The respective Area Under Curve (AUC), cut-off value, sensitivity and specificity are shown in Table 2. According to these results, the diagnostic efficacy of FM for AIS is higher than that of D-dimer.

ROC curves of FM and D-dimer for diagnosis of AIS. Comparison of sensitivity and specificity of FM and D-Dimer for AIS diagnosis. Red curve is FM, green curve is D-Dimer.
The AUC Value, Cut-Off Value, Sensitivity, and Specificity of FM and D-Dimer in the Diagnosis of AIS Patients.

FM, D-dimer Levels and NIHSS Scores in AIS Patients With Different TOAST Classification
As shown in Table 3, the level of FM in cardiogenic stroke patients was significantly higher than that in the other groups. The NIHSS score in cardiogenic stroke patients was significantly higher than that in atherosclerotic and unexplained stroke group. However, there was no significant difference in D-dimer levels between four groups.
Comparison of FM, D-Dimer Levels and NIHSS Scores in AIS Patients With Different TOAST Classification.
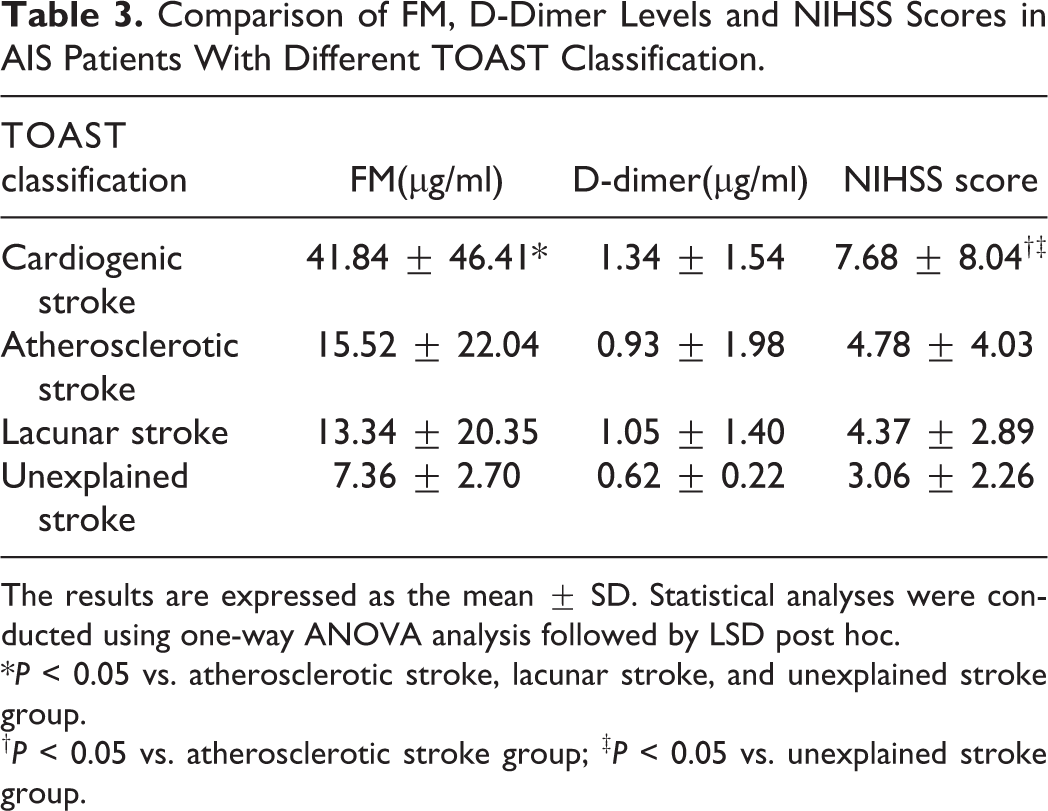
The results are expressed as the mean ± SD. Statistical analyses were conducted using one-way ANOVA analysis followed by LSD post hoc.
*P < 0.05 vs. atherosclerotic stroke, lacunar stroke, and unexplained stroke group.
† P < 0.05 vs. atherosclerotic stroke group; ‡ P < 0.05 vs. unexplained stroke group.
Correlation Between Level of FM, D-Dimer and NIHSS Score in AIS Patients With Different TOAST Classification
For cardiogenic stroke and atherosclerotic stroke patients, the level of FM was significantly correlated with NIHSS score (r = 0.3832, r = 0.3144). However, D-dimer was not statistically correlated with NIHSS score in either groups (Table 4).
Correlation Between Level of FM, D-Dimer and NIHSS Score in AIS Patients With Different TOAST Classification.
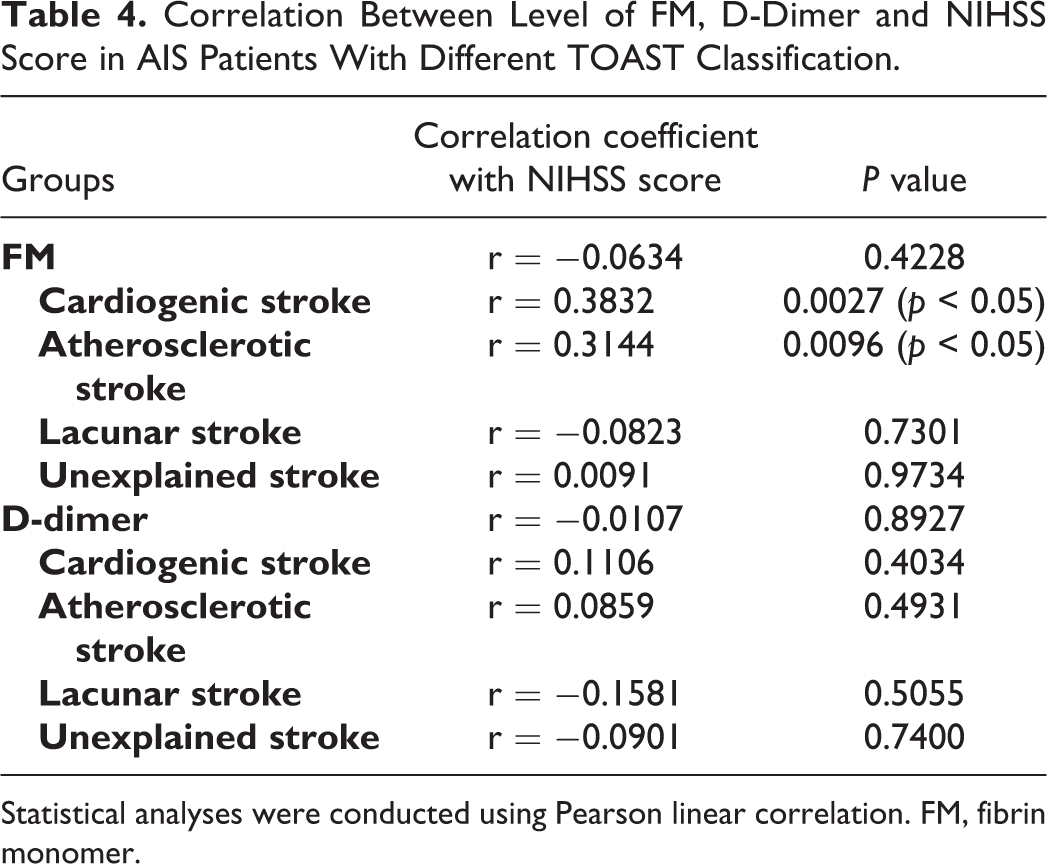
Statistical analyses were conducted using Pearson linear correlation. FM, fibrin monomer.
The Diagnostic Efficacy of FM for AIS With Different TOAST Classification
As shown in Table 5 and Figure 3, the diagnostic efficacy of FM for patients with cardiogenic AIS is higher than that for non-cardiogenic AIS.
The AUC Value, Cut-Off Value, Sensitivity, and Specificity of FM in the Diagnosis of AIS Patients With Different TOAST Classification.


ROC curves of FM for diagnosis of AIS patients with different TOAST classification. Comparison of sensitivity and specificity of FM for diagnosis of AIS with different TOAST classification. The red curve is cardiogenic stroke, the green curve is atherosclerotic stroke, the blue curve is lacunar stroke, and the purple curve is unexplained stroke.
Efficacy of Different Indicators to Distinguish Cardiogenic and Non-Cardiogenic AIS
The results in Table 6 and Figure 4 suggested that FM combined with NIHSS score was most valuable in differential diagnosis of cardiogenic and non-cardiogenic AIS.
The Efficacy of FM and D-Dimer Combined With NIHSS Scores in the Differential Diagnosis of Cardiogenic and Non-cardiogenic AIS.

Abbreviations: NA, not applicable.

ROC curves of different indicators for differentiating cardiogenic and non-cardiogenic AIS. Comparison of sensitivity and specificity of FM, D-Dimer, NIHSS score or FM combined with NIHSS score for the differential diagnosis of cardiogenic stroke and non-cardiogenic stroke. The gray curve is FM combine with NIHSS score, the yellow curve is NIHSS score, the green curve is D-Dimer, and the red curve is FM.
Discussion
The incidence of stroke has been increasing year by year, with an annual increase of 8.7 percent. It has become the leading cause of death for Chinese population. 14 –16 AIS accounts for about 70% of all strokes, 1 among which atherosclerosis and cardioembolic strokes are two common pathological types in clinical practice, according to the international TOAST classification widely used. Different physiological and pathological changes may have different responses to their individualized treatment (mechanical thrombectomy and intravenous thrombolysis), hence early diagnosis and individualized treatment are very important for the treatment effect and long-term prognosis of patients.
FM is the product of fibrinogen being cut off peptide chains A and B under the action of thrombin. The plasma concentration of FM reflects the activity of thrombin, and its generation is earlier than D-dimer and fibrinogen degradation product (FDP). Researchers have found that FM level rises earlier than other indicators in predicting thrombotic events. 17 –21 In this study, FM and D-dimer of 162 AIS patients who were admitted within 6 hours of onset without arteriovenous thrombolysis or mechanical thrombectomy were detected. We found that FM and D-dimers were significantly higher in AIS patients than in normal subjects. Moreover, ROC curve analysis showed that the area under the FM curve was 0.882, the area under the D-dimer curve was 0.739, thus FM is more sensitive and specific than D-dimer in the diagnosis of AIS.
The NIHSS score was widely quoted to assess the degree of neurological impairment in AIS patients. Fischer et al conducted digital subtraction angiography and NIHSS scores in patients with superearly ischemic stroke as early as 2005, and found that the NIHSS score was associated with intracranial arterial stenosis. 22,23 In the present study, no significant correlation between FM, D-dimer level and NIHSS scores in 162 AIS patients was found, which is consistent with the results obtained by Koji et al and Hirano et al. 13 However, when the correlation analysis was conducted in AIS patients with different TOAST classifications, we found that FM was correlated with NIHSS scores in cardiogenic and atherosclerotic stroke, suggesting that the NIHSS score can reflect the intracranial arterial stenosis in patients with these two pathological types.
Among cardiovascular events, cardiogenic stroke is the most serious complication in patients with atrial fibrillation. 24 Some scholars have suggested that the FM test is helpful for the differential diagnosis of cardiogenic stroke and non-cardiogenic stroke, 25 –27 and the NIHSS score in patients with cardioembolic stroke is higher than that of atherosclerotic type. 28 It has been suggested that the collateral circulation of atherosclerotic AIS is more abundant. The reason may be that in the process of the atherosclerotic AIS, the relatively slow progression of vascular stenosis and occlusion allow sufficient time for formation of collateral circulation. The incidence of intracranial arterial occlusion in patients with cardioembolic stroke is higher, which may also be related to the progression rate of vascular stenosis and occlusion. Cardioembolic AIS has a faster vascular stenosis and occlusion rate, resulting in a higher incidence of arterial occlusion. 29 –31 Furthermore, it has been reported that the NIHSS score of cardiogenic AIS is different from those of atherosclerotic, lacunar, and unexplained types. 17 Here, we compared the FM, D-dimer, and NIHSS scores in patients with different TOAST classifications, and the results showed that the FM level of the cardiogenic group was significantly different from that in other groups, while there was no significant difference in the level of D-dimers between groups. ROC curve analysis further revealed that FM can effectively differentiate patients with cardiogenic AIS and non-cardiogenic AIS. Based on the role of NIHSS score in distinguishing cardiogenic and non-cardiogenic stroke, we performed ROC curve analysis on both the single index and the combined index, and verified that FM combined with NIHSS score has higher suggestive significance for the diagnosis of cardiogenic AIS.
In summary, FM detection combined with NIHSS score is of great significance for the diagnosis and classification of AIS patients. However, there are some shortcomings in this experiment, such as the limitation of sample size, lack of information on the physical condition and medication status of the patients, and so on. Therefore, more large-scale prospective studies are still needed in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.