
Abstract
To investigate changes in coagulation during twin pregnancies. Methods: A total of 108 women with twin pregnancies and 442 women with singleton pregnancies were recruited. Coagulation tests, including fibrinogen (Fib), activated partial thromboplastin time (APTT), prothrombin time (PT) and thrombin time (TT), were performed during the course of the pregnancy. The level of fibrinogen gradually increased during singleton pregnancies, while the APTT and PT levels showed a decreasing trend with increasing gestational weeks. In twin pregnancies, the changes in PT and TT were similar, but other parameters displayed a different trend. Fibrinogen showed no significant difference between the second and third trimesters, while APTT showed an increasing trend from the second trimester to the third trimester. Compared with singleton pregnancies, the level of fibrinogen was higher in women pregnant with twins. APTT was longer in women pregnant with twins than in women with singleton pregnancies in the third trimester. PT was shorter in women pregnant with twins than in women with singleton pregnancies in the first and third trimesters. TT was shorter in women pregnant with twins than in women with singleton pregnancies in the first and second trimesters. Through this retrospective longitudinal analysis, this study presents the main coagulation parameter changes in singleton and twin pregnancies and confirms that coagulation is more enhanced in twin pregnancies than in singleton pregnancies.
Introduction
Pregnancy is a hypercoagulable state. 1 This physiological hypercoagulable state contributes to reducing postpartum hemorrhage but increases the risks of venous thromboembolism (VTE) and preeclampsia. 2,3 There have been some studies about coagulation-fibrinolysis among women with singleton pregnancies, and these studies have showed that coagulation parameters change according to gestational stage (fibrinogen showed an increasing trend, and APTT, PT and TT showed a shortened trend). 4 –6 Moreover, the coagulation-fibrinolysis parameters are different between women with singleton and twin pregnancies; for example, platelet count and antithrombin activity are likely to decrease, 7,8 and the D-dimer level is likely to increase in the late stage of twin pregnancies compared to that in singleton pregnancies.2,9 However, the longitudinal changes in coagulation parameters such as fibrinogen, APTT, PT and TT in twin pregnancies are still unclear. Therefore, in this study, we report longitudinal trimester-specific coagulation parameters in twin pregnancies.
Materials and Methods
A total of 471 and 110 women with singleton and twin pregnancies, respectively, underwent coagulation tests in the first trimester (GW 4-12+6), second trimester (GW 13-27+6) and third trimester (GW 28-41). Pregnant women were recruited from the outpatient and inpatient populations of Peking University Third Hospital from 2013 to 2018. Demographic characteristics were recorded from medical charts. Of these 581 women, 31 women were excluded because their complications may alter coagulation parameters; the reasons for exclusion are as follows: 4 with preeclampsia, and 27 with hereditary or acquired thrombophilia or anticoagulant use during pregnancy. Finally, the study was performed with data from 442 singleton and 108 twin pregnancies, and coagulation screening tests including fibrinogen (Fib), activated partial thromboplastin time (APTT), prothrombin time (PT), and thrombin time (TT) were performed at the first, second and third trimesters.
Blood samples were collected by venipuncture of an antecubital vein into vacuum tubes (Sekisui Medical Technology LTD., China) containing 3.8% sodium citrate.
Statistical analyses were performed using SPSS Version 26.0 software. The ages of subjects and the gestational weeks of pregnancy are presented as the mean ± SD. Statistical comparisons were performed with Repetitive Measure Analysis of Variance and Propensity Score Matching. In all analyses, P < 0.05 was taken to indicate statistical significance.
The research protocol was approved by the institutional Ethics Committee of the Bioscience Department of Peking University Third Hospital.
Results
The demographic characteristics of the subjects are described in Table 1. There were no significant differences in prepregnancy body mass index (BMI) between women with singleton pregnancies and those with twin pregnancies. However, women were significantly younger, gestational weeks at delivery were significantly lower and caesarean delivery was significantly more common in twin pregnancies than in singleton pregnancies. The main caesarean surgical indications of singleton pregnancy were scarred uterus (56.8%), foetal distress (13.0%) and malposition (8.1%). The gestational weeks at determination was earlier in singleton pregnancies than twin pregnancies in the first trimester and second trimester.
Characteristics of Women With Singleton and Twin Pregnancies.

From the first trimester to the third trimester, the comparison of fibrinogen, APTT, PT and TT of women with singleton and twin pregnancies is shown in Figure 1. For singleton pregnancies, the fibrinogen level showed an increasing trend with increasing gestational weeks (3.32 ± 0.54 g/L in the first trimester, 4.01 ± 0.55 g/L in the second trimester and 4.39 ± 0.60 g/L in the third trimester, respectively). The APTT and PT levels showed a decreasing trend (30.49 ± 2.89 s and 11.18 ± 0.68 s in the first trimester, 27.68 ± 2.07 s and 10.20 ± 0.45 s in the second trimester and 26.94 ± 2.21 s and 9.91 ± 0.49 s in the third trimester, respectively). TT was significantly shorter in the second trimester than in the first trimester (13.21 ± 0.81 s vs. 13.73 ± 0.91 s, P < 0.001), but there was no significant difference between the third trimester and the second trimester. The trend of PT and TT of twin pregnancies was similar to that of singleton pregnancies, while other parameters exhibited some differences in twins. Fibrinogen levels and APTT were consistent with singletons from the first trimester to the second trimester, but there was no difference between the second and third trimesters in fibrinogen (4.41 ± 0.66/L vs. 4.59 ± 0.85 g/L, P = 0.160), while APTT showed a prolonged trend from the second trimester to the third trimester (27.76 ± 2.40 s vs. 28.57 ± 2.64 s, P = 0.006).
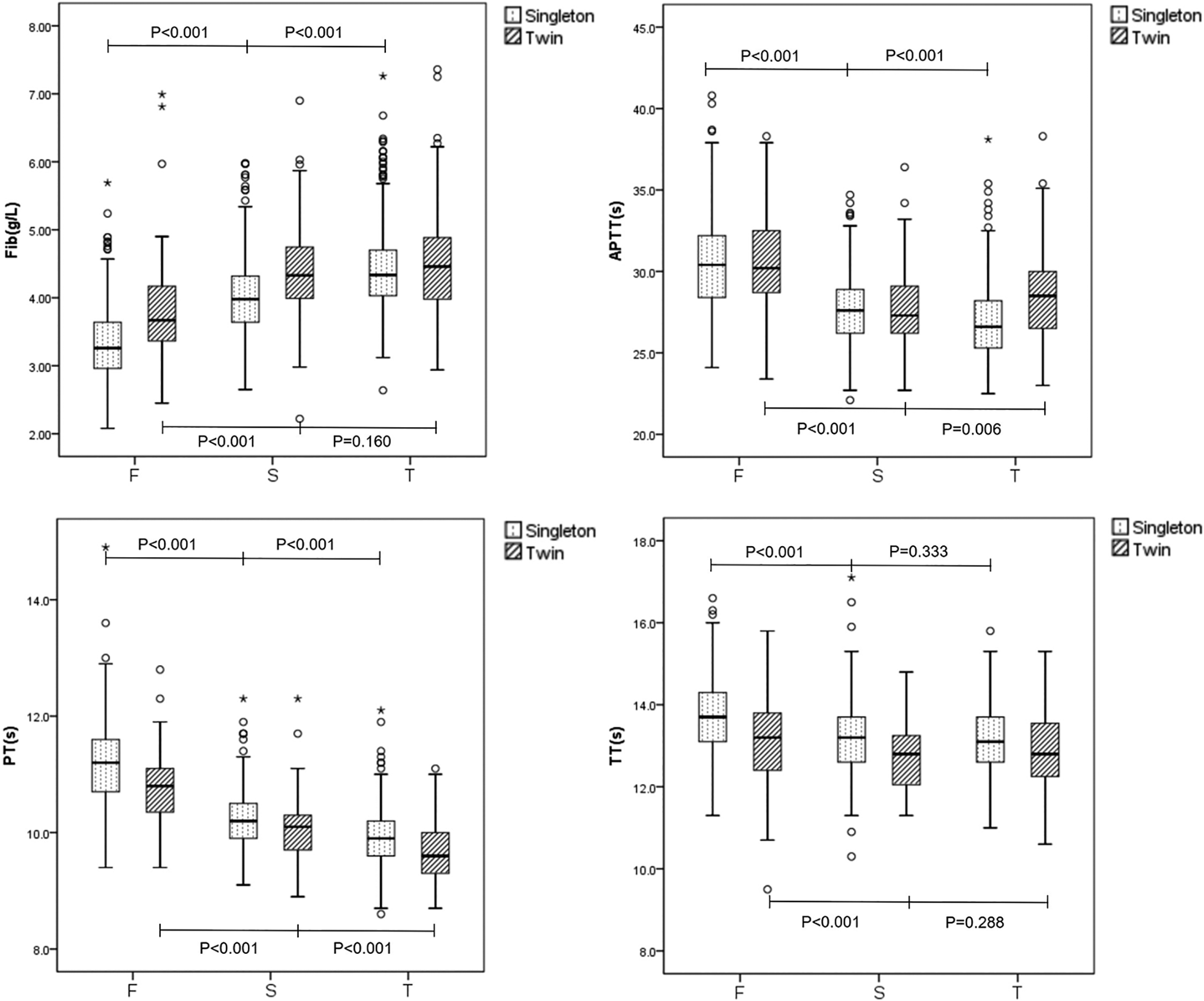
Trimester-specific reference ranges for fibrinogen, APTT, PT and TT. F, first trimester; S, second trimester; T, third trimester. The upper edge and the lower edge of the box indicate the 75th percentile and 25th percentile, respectively. The horizontal bar in the middle of each box plot represents the median value. The upper horizontal line and the lower horizontal line of the box plot indicate the 97.5th percentile and 2.5th percentile, respectively.
Considering the influence of age and gestational weeks on coagulation, we selected 190 specimens (95 twins and 95 singletons) to analyze the differences between twin and singleton pregnancies. The demographic characteristics are described in Table 2. Neither mean maternal age nor gestational weeks differed significantly between women with singleton and twin pregnancies. A comparison between women with singleton and twin pregnancies with respect to coagulation screening tests at the first, second and third trimesters is shown in Table 3.
Characteristics of Women With Singleton and Twin Pregnancies.

Coagulation Parameters of Women With Singleton and Twin Pregnancies.
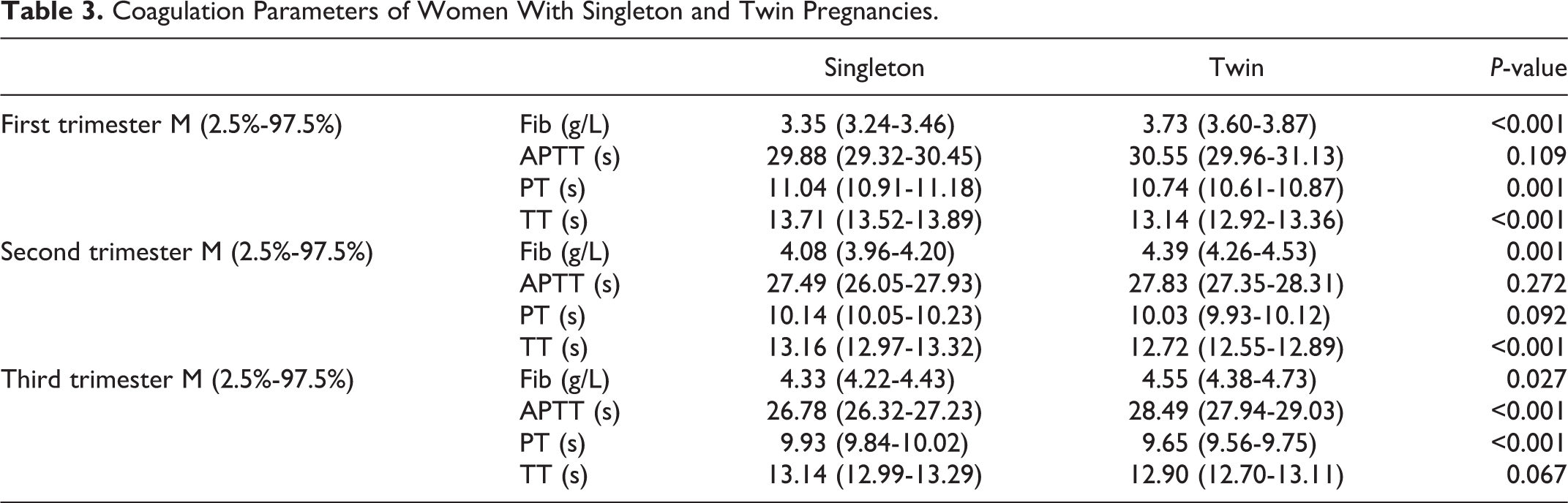
In this sample of 190 women, 38 and 26 women with singleton and twin pregnancies, respectively, had D-dimer data in the third trimester. The maternal age (34.92 ± 4.71 vs. 33.04 ± 4.05, p = 0.102) and gestational weeks at determination (35.74 ± 3.04 vs. 35.46 ± 1.63, p = 0.642) were similar, but the D-dimer level was significantly different (0.66 ± 0.46 μg/mL vs. 1.40 ± 0.96 μg/mL, p = 0.001).
Discussion
The coagulation system of women during pregnancy is different from that of nonpregnant women because of the physiological need to prevent postpartum hemorrhage. In the studies of Cui and Liu, fibrinogen showed an increasing trend, and APTT, PT and TT levels showed a decreasing trend with increasing gestational weeks in women with singleton pregnancies. 4,10 From Figure 1, the trend of fibrinogen, APTT, PT and TT during singleton pregnancies was consistent with the results of earlier studies and reflected coagulation system enhancement through the first to the third trimester. Moreover, a limited number of studies have shown that coagulation is more enhanced in women with twin pregnancies than in women with singleton pregnancies. 8 This exaggerated coagulation during twin pregnancies is thought to be related to higher risk of thrombosis or prothrombosis, such as venous thromboembolism and preeclampsia. This study analyzed coagulation parameters in twin pregnancies longitudinally and confirmed this difference between singleton and twin pregnancies.
Compared with singleton pregnancies, fibrinogen was higher and did not increase from the second trimester to the third trimester in women pregnant with twins. Yamada et al. found that the fibrinogen level of women with twin pregnancies decreased in the last few weeks of pregnancy. 11 Perhaps the reason is that fibrinogen is consumed in the presence of enhanced coagulability in twin pregnancies. In this study, the D-dimer level was significantly higher in the third trimester in women with twin pregnancies than in women with singleton pregnancies, confirming increased coagulation in women with twin pregnancies. Moreover, the increase in the D-dimer level in twins during the second and third trimesters was mentioned in the study of Bar. 9
From Figure 1 and Table 3, APTT showed a decreasing trend from the first trimester to the second trimester and an increasing trend from the second trimester to the third trimester in twin pregnancies, which is different from the findings in singleton pregnancies. The increase of APTT in third trimester may be caused by the lower fibrinogen level in the late stage of twin pregnancies. In the study of Hammerova, Factor XI decreases as gestational weeks increase, 12 which may also influence APTT. But other studies showed Factor XI levels is slightly increased or unchanged during pregnancy, 13 –15 further studies would be needed to figure out the increase of APTT. In this study, PT was shorter in women with twin pregnancies than in women with singleton pregnancies, especially in the first and third trimesters, but the trend during pregnancies was consistent with women with singleton pregnancies. TT was also shorter in women with twin pregnancies, especially in the first and second trimesters. The different levels of PT and TT are thought to be influenced by the enhanced coagulation system in twin pregnancies.
This study analyzed coagulation parameters in twin pregnancies longitudinally and compared them with the respective parameters in singleton pregnancies. However, there were some limitations in our study. Because of the deficiency of D-dimer data, we did not analyze D-dimer in detail. Moreover, the number of participants was not large enough in our study.
Conclusion
This study confirms that coagulation is more enhanced in women with twin pregnancies than in women with singleton pregnancies, especially in the late stage, and establishes the trend of coagulation parameters (fibrinogen, APTT, PT and TT) in twin pregnancies. Moreover, this study demonstrates APTT level increases from second trimester to third trimester in twin pregnancies, which is different from singleton pregnancies.
Footnotes
Authors’ Note
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article. Ethical approval to report this case series was obtained from Ethics Committee of the Bioscience Department of Peking University Third Hospital (No. IRB00006761-2016145).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Key Research and Development Program of Reproductive Health & Major Birth Defects Control and Prevention (2016YFC1000400).