
Abstract

Prekallikrein (PK) deficiency is a rare defect of the contact phase of blood coagulation. 1 Patients with this defect show no bleeding tendency. On the contrary, sporadic or preliminary studies indicate that they may present an increased incidence of atherosclerotic and thrombotic events. 2
The defect seems to concern mainly African-Americans who present a higher incidence of PK deficiency 3 –5 as compared to Caucasian-Americans. 4
Since African-Americans (AA) suffer frequently of Cardiovascular Disorders (CVD), the role of PK deficiency could be maintained to act as a contributory causal effect. 6 –8
Nevertheless, other environmental, nutritional and genetic factors may also be involved. 5
Sporadic reports of PK deficiency in other Africans have also appeared. 9,10 Unfortunately, no large clinical or genetic study is available.
We thought it worth trying to correlate this high prevalence of PK deficiency seen in AA with CVD as compared with Caucasian-Americans with the same condition.
AA with PK deficiency and CVD are gathered in Table 1. 11 –24 It has to be noted that for a few papers dealing with PK defects, no ethnic background is indicated. It is likely that at least some of them may also involve AA. In the few instances we have succeeded in demonstrating it by direct or indirect contact with the Authors of the papers involved. Such cases are indicated with a) in Table 1.
African-Americans With PK Deficiency and Hypertension or Other CV Disorders.

M.I = Myocardial Infarction; CHF = congestive heart failure; CAD = coronary arterial disease; UA = unstable angina; CABG = coronary artery bypass graft; LMWH = low molecular weight heparin.f.s. = frame shift.
There are at least 16 AA patients with PK deficiency and CVD.
Since we do not know the total number of AA subjects with PK deficiency in the USA, we cannot draw general conclusions. On the basis of the available data, it would appear that about 50% of the reported AA patients with PK deficiency present CVDisordes. 4 On the contrary, the prevalence among Caucasians-Americans is only about 20%. 25 –27
The incidence of CVD in Caucasian-Americans with PK deficiency is shown in Table 2. The difference is statistically significant (p = 0.01). This is based on the reported cases and therefore has limitations. Unfortunately, there is also no available study on the prevalence of PK deficiency in the Caucasian-American population.
Number of African-Americans (AA) With PK Deficiency and Cardiovascular Disorders (CVD) Versus Caucasian-Americans (CA) With PK Deficiency and CVD.
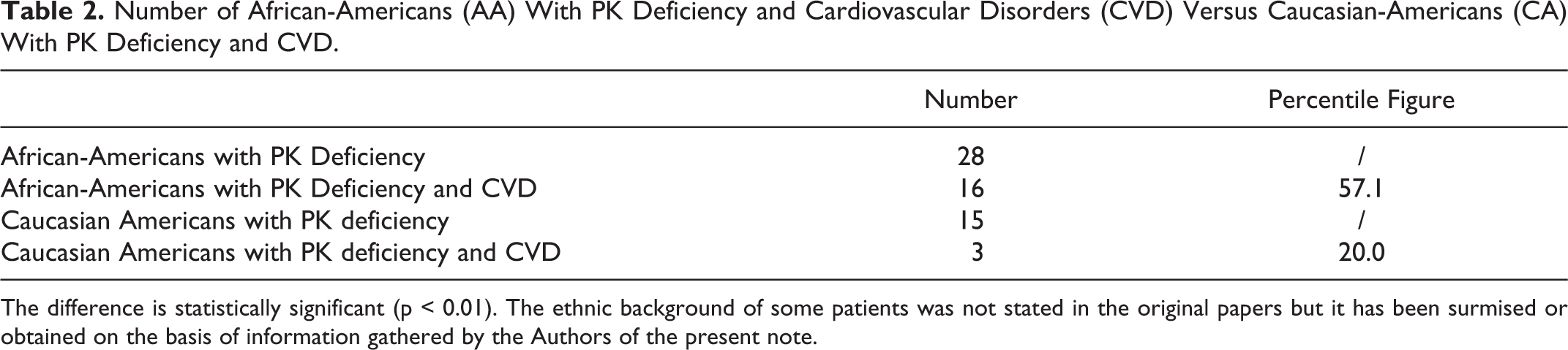
The difference is statistically significant (p < 0.01). The ethnic background of some patients was not stated in the original papers but it has been surmised or obtained on the basis of information gathered by the Authors of the present note.
The incidence of CVD seen in reported cases of AA with PK deficiency seems higher than that seen in the remaining population of the USA with PK deficiency (Table 2).
It would seem that PK deficiency is more severe in AA as compared to Caucasian-Americans with the same defect. Alternatively, it could suggest that other predisposing causes favoring CVD are present in the AA population.
This is intended only to indicate that PK deficiency may play a role in the genesis of these disorders and it does not exclude the role and/or the co-existence of other causes.