
Abstract
To evaluate the efficacy and safety of TurboHawk plaque rotation system combined with drug-coated balloon in treating lower extremity arterial disease (LEAD) of diabetes patients, a total of 145 diabetic patients with LEAD from March 2015 to September 2016 were recruited in our study. Lower extremity arterial disease was diagnosed by ultrasound and CT angiography (CTA). According to the surgical method, 65 cases underwent TurboHawk plaque rotation combined with drug-coated balloon (group A), 80 cases underwent simple drug-coated balloon expansion (group B). The characteristics of lesion, function test, ankle-brachial index (ABI), and postoperative complications were analyzed. All the patients were followed up at 1, 3, 6, 12, and 24 months after operation. At baseline, there was no difference in all the characteristics between the 2 groups. The early postoperation minimum lumen diameter (MLD), lumen stenosis rate, and ABI in 2 groups both improved. As the follow-up time increased, patients in group A had significantly higher MLD and ABL value, as well as lower level of lumen stenosis rate, restenosis rate, late lumen loss, and target lesion revascularization (all P < .05). Accordingly, functional testing revealed the 6-minute walk distance, 6-minute claudication distance, resting ABI, and post-exercise ABI in group A were significantly higher than those in group B (all P < .05). Besides, major graft reintervention (4.62% vs 11.25%) and major adverse limb events (6.15% vs 12.5%) in group A occurred less frequently than group B (all P < .05). In conclusion, the long-term effect of the combined approach was better than only drug-coated balloon in LEAD in Chinese diabetes patients.
Keywords
Diabetes is one of the most important chronic noncommunicable diseases threatening global human health, especially in China. The prevalence of diabetes was 9.7% in Chinese aged 21 years or over, which means that 92.4 million Chinese adults are having diabetes. 1 It was also reported that up to 35% of adults in the United States had prediabetes, which is a big factor for type 2 diabetes and cardiovascular disease (CVD). 2 Elderly patients with type 2 diabetes have a 5.9-fold increased risk of major artery cardiovascular events and might be expected to have a high prevalence of the lower extremity arterial disease (LEAD). 3 Lower extremity arterial disease is a major manifestation of systemic atherosclerosis with severe associated cardiovascular, lower limb, and functional complications. It results from a partial or complete obstruction of one or more lower limb arteries. During the last decades, a large body of data had reported that LEAD was associated with increased risk of nontraumatic lower limb amputation, CVD, and mortality. 4 –6 Nowadays, LEAD has become an emerging public health burden with an endemic progression worldwide resulting from a demographic expansion, population aging, and increasing prevalence of tobacco use, hypertension, dyslipidemia, and type 2 diabetes. 7
Lower extremity arterial disease affects over 200 millions of people worldwide, including 40 millions living in Europe. 8 It is 2 to 4 times more frequent in people with type 2 diabetes than in the general population. 9,10 The key risk factors associated with LEAD include age, sex, tobacco smoking, systolic blood pressure (SBP), and plasma concentrations of lipids. 7 Many mechanisms contribute to the development of LEAD, in particular arterial stiffness, thrombotic abnormalities, low-grade inflammation, advanced glycation end-products, and oxidative stress. 7 Because of poor prognosis and complex mechanism, a lot of effort had been put into developing treatments of LEAD. The management of LEAD in patients with diabetes requires a multidisciplinary team and usually includes drug therapy, multifactorial intervention therapy, innovating treatment, lifestyle management, surgical, and endovascular revascularization treatment. Antidiabetic, antihypertensive, lipid-lowering, and antiplatelet medications may improve the cardiovascular prognosis of patients with LEAD, but few have been done to test their benefits to reduce the occurrence and the progression of LEAD as well as lower extremities adverse events.
Over the last decade, the development of new techniques encouraged the implementation of endovascular therapy in patients with LEAD. The different options of revascularization depend on several factors including anatomical location, extension, and length of arterial lesions; general health condition of each patient and comorbidities, as well as surgeon experience. Different types of endovascular revascularization procedures could provide better choice for patients with short stenosis or occlusion of iliac arteries, long or bilateral lesions and severe comorbidities, and allow for good long-term patency . 11,12 Balloon angioplasty was the most common endovascular arterial intervention performed in the patients with LEAD. Poor long-term patency was the main factor leading to the development of drug-eluting balloons, in which drug diminishes or eliminates smooth cell proliferation and thus significantly reduces the incidence of recurrent stenosis. 13 TurboHawk plaque rotation system was a new kind of atherectomy device, which could be classified as excisional atherectomy (removal of plaque) and ablative atherectomy (disintegration or vaporization of plaque without removal) device. However, there was little research evaluating the effect of TurboHawk plaque rotation system combined with drug-eluting balloons on LEAD. Considering the unsatisfactory therapeutic effect of the current procedure, we conduct this study to evaluate the efficacy and safety of TurboHawk plaque rotation system combined with drug-coated balloon in treating diabetic patients with LEAD.
Materials and Methods
Participants
A total of 145 diabetic patients with LEAD treated with TurboHawk were recruited in our study from March 2015 to September 2016. Type 2 diabetes was diagnosed according to 2012 American Diabetes Association standards. Lower extremity arterial disease was diagnosed by ultrasound and CTA. Exclusion criteria included type 1 or specific types of diabetes mellitus, acute complications of diabetes, renal dysfunction (glomerular filtration rate < 60 mL/min/1.73 m2), osteomalacia, history of cerebral infarction, and degenerative changes in cervical vertebra. According to the surgical method, there were 65 cases undergoing TurboHawk plaque rotation combined with a drug-coated balloon (group A) and 80 cases undergoing simple drug-coated balloon expansion (group B). The characteristics of lesion, improvement of symptoms, ankle-brachial index (ABI), and postoperative complications were analyzed. Every patient recruited in the study signed the informed consent. The study was approved by the Human Research and Ethics Committee of General Hospital of Ningxia Medical University with adherence to the tenets of the Declaration of Helsinki.
Surgical Procedure
Preoperative angiography was used to evaluate vascular stenosis and plaque and the surgical method was selected according to the status of vascular stenosis. Patients in group A underwent TurboHawk plaque rotation combined with a drug-coated balloon. In brief, after satisfactory local anesthesia with 2% lidocaine, the femoral artery was retrogradely inserted with the 5F vascular sheath and 4000 U heparin was administered intravenously. After the guide wire and catheter successfully reached the contralateral external iliac artery, angiography showed the lesion site of the artery and arterial protection umbrella was placed. The TurboHawk plaque transluminal extraction system was placed along the umbrella guide wire and plaque resection was performed in multiple quadrant of artery. A suitably sized balloon was placed in the narrowed vessel and dilated at pressure for 2 minutes. After exiting the balloon dilatation catheter, the angiography indicated that the residual stenosis was less than 30%. The excision process was smooth without any dissection or rupture of the artery. Capture emboli could be gathered in the arterial umbrella. Patients in group B underwent only drug-coated balloon expansion.
Clinical Measurement
Information on age and history of smoking, drinking, diabetes, hypertension, coronary artery disease, dyslipidemia, and using-drugs were obtained from questionnaires. Before surgery, height, weight, waist circumference, hip circumference, and blood pressure of every patient were measured. The body mass index was calculated as the weight (kg) divided by the square of height (m). Waist:hip ratio was calculated as the waist circumference (cm) divided by the hip circumference (cm). Blood pressure was measured by the same nurse using mercury sphygmomanometer 3 times and averaged.
The ABI was measured using a Nicolet VersaLab SE Vascular Doppler Systems (San Carlos, California) with appropriate cuff inflators for brachial circumference, in accordance with international standards. 14 The patient’s ABI was determined by the lower value of the 2 sides of ABI. Lower extremity arterial disease was determined on the basis of ABI lower than 0.9.
Biochemical Analysis
Blood samples were collected from an antecubital vein and measured by an enzymatic method using an automatic biochemical analyser (7600-020; Hitachi, Inc., Tokyo, Japan) to determine total cholesterol, triglyceride, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, blood urea nitrogen, serum creatinine (Cr), and uric acid. Fasting plasma glucose and 2 hours postprandial blood glucose were estimated by a glucose oxidase method (Automatic Biochemistry Analyser; Beckman Coulter, Brea, California). Glycosylated hemoglobin (HbA1c) was performed by high-pressure liquid chromatography, using the Variant II machine (Bio-Rad, Hercules, California). Glycosylated serum albumin was determined by the liquid enzymatic method, using the Glamour 2000 automatic biochemical analyser (MD Inc, Silicon Valley, California).
Functional Measures
Patients performed measures of exercise performance until symptom-limited claudication, exhaustion, or completion of study protocol: a 6-minute walk and a standardized graded Skinner-Gardner exercise treadmill test. During the treadmill test, total treadmill exercise time, symptom-limited VO2, and pre-/post-exercise ABI were measured in all patients.
End Points and Follow-Up
The primary end point was the efficacy of the relay puncture technique, as indicated by the acute technical success and post-procedure clinical improvement of critical limb ischemia symptoms. The secondary end point was the safety of this technique, as indicated by the number or severity of complications associated with this procedure. The primary safety end point was the composite of major amputation, major graft reintervention, procedure-related death, and major adverse limb events.
Ankle-brachial index evaluation, Color Doppler ultrasonography, and/or computed tomography angiography were performed at 1, 3, 6, 12, and 24 months or when symptoms recurred after discharge. Blood test and functional measurement were performed annually for all the patients. Vascular parameters follow-up mainly included minimum lumen diameter (MLD), lumen stenosis rate, restenosis rate, late lumen loss (LLL) and target lesion revascularization (TLR). Vascular ultrasound or lower limb CTA was used to measure the vascular diameter of the stenosis and the normal vessel diameter. Stenosis rate (1 − [stenosis artery diameter ÷ normal artery diameter] × 100%) was calculated. Stenosis rate higher than 50% was diagnosed as vascular restenosis. Late lumen loss was defined as the difference between MLD of the target vessel taken after the operation immediately and that taken at follow-up. Target lesion revascularization rate was defined as the ratio of target vascular receiving cavity treatment again afterward.
Statistical Analysis
Software SPSS version 16.0 (SPSS Inc, Chicago, Illinois) was used for statistical analysis. Figures were created by GraphPad Prism version 5.0 (GraphPad Software, Inc, San Diego, California) and city and country [other than USA] for the supplier “GraphPad Software, Inc.”]. Data were expressed as mean ± standard deviation for continuous variables and percentages (%) for categorical variables. Differences between the groups were analyzed by Student or χ2 test as appropriate for measurement data or categorical values. Multiple logistic regression analysis was performed to evaluate the odds ratio and associated factors. A 2-tailed P < .05 was considered to be statistically significant.
Results
Between March 2015 and September 2016, the trial enrolled 145 diabetic patients with atherosclerotic occlusion of LEAD treated with TurboHawk. The study population (n = 145, 71 men and 74 women) had a mean age of 58.43 ± 11.07 years, having type 2 diabetes for 9.41 ± 6.24 years. According to the surgical method, patients were divided into 2 groups: group A underwent TurboHawk plaque rotation combined with a drug-coated balloon (n = 65, 33 men and 32 women) and group B underwent simple drug-coated balloon expansion (n = 80, 38 men and 42 women). The baseline patient characteristics for all groups are presented in Table 1. The mean time to the 12th-month visit was 389 ± 58 days and 373 ± 74 days later for 24th month.
Patient Characteristics at Enrollment According to Treatment Group.

Abbreviations: ABI, ankle-brachial index; BMI, body mass index; BUN, blood urea nitrogen; CAD, coronary artery disease; Cr, serum creatinine; DBP, diastolic blood pressure; FBG, fasting blood glucose; GA, Glycosylated serum albumin; HbA1c, glycosylated hemoglobin; HDL-C, high-density lipoprotein cholesterol; 2hPG, 2-hour post-meal blood glucose; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride; UA, uric acid.
Baseline Characteristics
The demographics and clinical characteristics at baseline were reported in Table 1 and were comparable for the 2 treatment groups. The mean baseline ABI was 0.55 ± 0.13 among all the patients. There was no significant difference in all the parameters between 2 groups (all P > .05).
Comparison of Vascular Recanalization
There was no significant difference in primary patency rate between the 2 surgical methods. Representative digital subtraction angiography (DSA) images of patients in group A is shown in Figure 1. Vascular parameters over time in both 2 groups are discussed in Table 2. Early postoperation MLD, lumen stenosis rate, and ABI value in 2 groups both improved and there was no difference in these 3 parameters. After 3 months, the LLL (mm) in group A (0.12 ± 0.06) was significantly lower than that in group B (0.25 ± 0.11; P < .05). After 6 months, the patients in group A had significantly higher level of MLD (mm, 3.67 ± 0.44 vs 3.27 ± 0.48) and ABI value (0.98 ± 0.15 vs 0.88 ± 0.23) compared to group B, as well as lower level of lumen stenosis rate (%, 16.95 ± 9.51 vs 21.44 ± 14.06), restenosis rate (%, 1.54 vs 11.25), and LLL (mm, 0.22 ± 0.10 vs 0.53 ± 0.41; all P < .05). Besides, at 12 and 24 months, the TLR in group A were both significantly lower than those in group B (both P < .05).

Representative digital subtraction angiography images of patients in group A before (A) and after (B) treatment showing improvement in the appearance of artery stenosis (arrows).
Vascular Parameters Over Time.
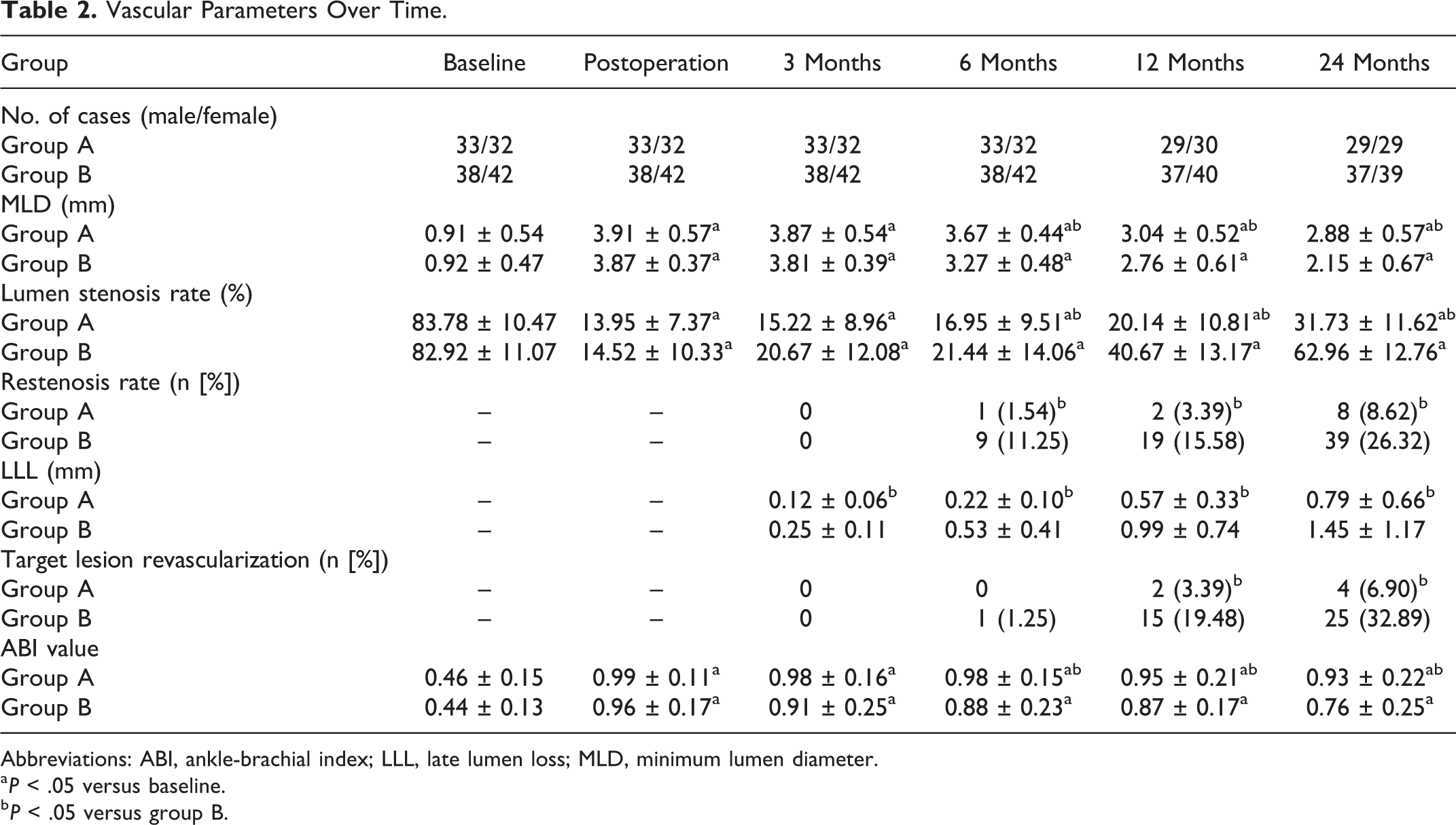
Abbreviations: ABI, ankle-brachial index; LLL, late lumen loss; MLD, minimum lumen diameter.
a P < .05 versus baseline.
b P < .05 versus group B.
Comparison of Blood
We compared the indices of blood of all the patients annually. The results were summarized in Table 3. The Cr level in both groups was significantly higher than baseline after 2-year follow-up (both P < .05). Besides, the Cr level in group A was significantly lower than that in group B (P < .05). There was no other significant difference in blood parameters.
Comparison of Blood Parameters Over Time.

Abbreviations: CAD, coronary artery disease; Cr, serum creatinine; DBP, diastolic blood pressure; FBG, fasting blood glucose; GA, Glycosylated serum albumin; HbA1c, glycosylated hemoglobin; HDL-C, high-density lipoprotein cholesterol; 2hPG, 2-hour post-meal blood glucose; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride; UA, uric acid.
a P < .05 versus Baseline.
b P < .05 versus group B.
Functional Testing
After operation, the indicators of functional testing in all the patients were significantly improved (P < .05). Results are reported in Table 4. At 12 and 24 months, the 6-minute walk distance (ft) in group A (12 months: 1189 ± 388; 24 months: 1078 ± 317) were significantly longer than those in group B (12 months: 968 ± 377; 24 months: 976 ± 299; P < .05). Similar results were found in 6-minute claudication distance. Besides, resting ABI were higher in group A at 12 months (0.95 ± 0.21) and 24 months (0.93 ± 0.22) than those in the group B (0.87 ± 0.17; 0.76 ± 0.25), respectively. The post-exercise ABI in group A was also higher than those in group B both at 12 and 24 months (all P < .05). There was no significant difference in treadmill exercise time, treadmill time to claudication, and VO2 between 2 groups.
Function Text Over Time.

Abbreviation: ABI, ankle-brachial index.
a P < .05 versus baseline.
b P < .05 versus group B.
Safety end points: The primary safety end point of major graft reintervention and adverse limb events was superior in group B through 2 years of follow-up. Major graft reintervention occurred in 3 (4.62%) of 65 patients in group A compared to 9 (11.25%) of 80 patients in group B (P < .05; Table 5). Major adverse limb events occurred in 4 (6.15%) of 65 patients in group A, compared with 10 (12.5%) of 80 patients in group B (P < .05; Table 5). There was no other significant difference in safety end points between the 2 groups.
Safety End Points in Patients Between Group A and B at 2 Years.

Abbreviation: MALE, major adverse limb event.
Discussion
In this study, we aimed at evaluating the efficacy and safety of TurboHawk plaque rotation system combined with a drug-coated balloon in treating diabetic patients with LEAD. A total of 145 diabetic patients with atherosclerotic occlusion of LEAD treated with TurboHawk were recruited in our study. After postoperative effect evaluation and 2-year follow-up, it was revealed that there was no significant difference in primary patency rate between the 2 surgical methods. However, after 6 months, the patients in TurboHawk combined with drug-coated balloon group had significantly higher level of MLD and ABI value, as well as lower level of lumen stenosis rate, restenosis rate, and LLL, compared to simple drug-coated balloon group. Besides, at 12 and 24 months, the patients in TurboHawk combined with drug-coated balloon group had significantly lower rates of TLR. These results demonstrated that TurboHawk combined with drug-coated balloon had significantly better long-term treatment effect on lower extremity arterial in diabetic patients with LEAD. In addition, major graft reintervention and major adverse limb events occurred significantly less in patients receiving treatment of TurboHawk combined with drug-coated balloon in 2 years. This 2-year follow-up study showed that compared to drug-coated balloon, treatment combined with TurboHawk plaque rotation system could help diabetic patients with LEAD acquire more clinical benefit and lower safety risk for long term.
In recent years, with an aging population and the improvement of living standard, the prevalence of type 2 diabetes has been keeping rising. The latest epidemiological findings demonstrated that the number of adult with diabetes in China accounts for one-third of the number of the world and the prevalence rate has reached as high as 10.4%. 15 Diabetes has become one of the most important chronic diseases threatening the health of Chinese people. Lower extremity arterial disease was an important component of diabetes macrovascular complications, manifested as hardening, plaque formation, stenosis, or occlusion of lower extremity arteries. According to the 2013 guidelines for diabetes prevention and treatment in China, diabetic patients aged over 50 years accompanied by high blood lipids, hypertension, and other risk factors should be annually screened for LEAD. Lower extremity arterial disease occurred in patients with diabetes usually involved small arteries such as the profunda femoris artery and the anterior tibial artery. The vascular atherosclerosis, sometimes accompanied by microvascular lesions or peripheral neuropathy further led to lower limb ischemia, necrosis, and even amputation, which was the main cause of disability in patients with diabetes. In the retrospective study recruited in 308 hospitalized amputees in 17 major cities of China, Wang et al showed that amputations caused by diabetic feet accounted for 27.3% of all cases with amputation. 16 To determine the incidence and clinically relevant risk factors for diabetic amputation, Jiang et al conducted a cohort study and investigated a total of 669 diabetic foot ulceration patients. 17 Their results showed that the overall amputation rate among diabetic foot patients was 19.03%, and the major and minor amputation rates were 2.14% and 16.88%, respectively. 17 Lower extremity arterial disease seriously threatens the quality of life and health of patients with diabetes. However, the screening technique and prevalence of LEAD were not encouraging. It was revealed that from 1991 to 2000, the overall prevalence of LEAD in 30 provinces of China was 5.0%. And in 2010, this number went up to 24.66% in outpatients with type 2 diabetes, using ABI screening.
Common risk factors of LEAD included age, SBP, and duration of diabetes. The previous study reported that as the age, SBP, or duration of diabetic patients increased, the prevalence of LEAD significantly increased. 18 Aging caused a series of changes in the structure of arterial wall, including endothelial dysfunction, increased collagen, and decreased elastin, thickened intima, and increased vascular stiffness, and thus lead to hypertension and atherosclerosis. 19 Hypertension could further aggravate vascular endothelial dysfunction and increase the permeability of vascular endothelial to plasma protein and monocytes. Along with the prolonged duration, exposure of vascular lesion risk factors increased. Increased blood viscosity, glycosylation end products, and oxidative stress response finally led to vascular endothelial injury, thrombosis, and stimulation of vascular smooth muscle cell proliferation. 20 Nowadays, ABI assays and peripheral ultrasound are the most commonly used methods for noninvasive screening and diagnosis of LEAD. Peripheral vascular ultrasound could monitor the morphology and hemodynamics of vascular wall directly but requires professional ultrasound specialists. Another technology ABI detection currently becomes an important method to screen the risk of lower limb arteriosclerosis, with high sensitivity and specificity of ABI <0.9 in 95% and 99%, respectively. 21 As the gold standard in the diagnosis of peripheral vascular lesion, DSA could clearly display the vessel wall and detect the presence of occluded lesion and collateral circulation. Till now, there was no breakthrough in the drug treatment of LEAD, mainly including anticoagulant therapy, vasopressor, or prostaglandin. However, oral medicine could only relieve symptoms without reversing vascular lesions. Traditional lower limb artery bypass grafts surgery is narrowly applied because of difficulty in finding a suitable graft in patients with diabetes. As a new therapeutic technique, interventional therapy has the characteristics of less occurrence in trauma or complications, which is gradually widely used in clinic. Percutaneous balloon dilatation was the earliest clinical application of glycosuria interventional therapy for patients with LEAD. With the development of interventional materials and surgical methods, treatments nowadays mainly included bare metal stents, drug-coated stents, drug-coated balloons, and plaque rotation. 22 –24 Werk et al. conducted a randomized multicenter study to evaluate the effectiveness and safety in paclitaxel-coated balloon. 22 The 6-month follow-up angiography showed less LLL in the coated balloon group and the number of TLRs was lower in the paclitaxel-coated balloon group than in the control subjects. Besides, improvement in Rutherford class was significantly greater in the coated balloon group. The difference in TLRs between paclitaxel-coated balloon and uncoated balloon groups was maintained up to >18 months. No adverse event related to balloon coating was assessed in their study. 22 However, the drug-coated balloon has no obvious effect on the existing intimal plaque, hyperplasia intimal tissue, or severe calcification. 25 Due to the difference in length or degree of vascular stenosis, the uneven pressure during balloon dilatation could increase the risk of vascular rupture and the formation of restrictive interlayer. 25 Plaque rotary surgery used a high-speed rotating carbon cutting blade to cut the plaque or thrombus in the vascular lumen to increase the lumen volume and enlarge the lumen diameter. 26 It was revealed that cumulative patency rates were 75% one month after using percutaneous mechanical thrombectomy in treating acute and subacute occlusions of peripheral arteries and bypasses alone, 71% after 6 months, 38% after 12 months, 33% after 18 months, and 30% after 24, 30, 36, and 42 months when using percutaneous mechanical thrombectomy in treating acute and subacute occlusions of peripheral arteries and bypasses alone. 27 Although long-term patency rate of percutaneous mechanical thrombectomy was relatively low, the success in immediate blood flow recovery could help drug-coated balloon play a better effect on target blood vessels surface. Plaque rotation system combined with drug-coated balloon could overcome their limitations, greatly reduce the rate of intraoperative salvage stent placement, and increase the rate of postoperative lumen patency. 28 In our study, at baseline, there was no difference in all the demographics and clinical characteristics between the 2 groups. After 3 months, the LLL (mm) in TurboHawk plaque rotation system combined with drug-coated balloon group (0.12 ± 0.06) was significantly lower than that in drug-coated balloon group (0.25 ± 0.11). After 6 months, the patients underwent plaque rotation with drug-coated balloon had significantly higher level of MLD (mm, 3.67 ± 0.44 vs 3.27 ± 0.48) and ABI value (0.98 ± 0.15 vs 0.88 ± 0.23) compared to patient in another group, as well as lower level of lumen stenosis rate (%, 16.95 ± 9.51 vs 21.44 ± 14.06), restenosis rate (%, 1.54 vs 11.25), and LLL (mm, 0.22 ± 0.10 vs 0.53 ± 0.41). Besides, at 12 and 24 months, the TLR in TurboHawk plaque rotation system combined with a drug-coated balloon group were both significantly lower than those in the drug-coated balloon group. Accordingly, functional testing revealed the 6-minute walk distance, 6-minute claudication distance, resting ABI, and post-exercise ABI in combination group were significantly higher than those in the drug-coated balloon group. In the aspect of safety, major graft reintervention (4.62% vs 11.25%) and major adverse limb events (6.15% vs 12.5%) occurred less frequently in TurboHawk plaque rotation system combined with drug-coated balloon group compared to drug-coated balloon group.
Some limitations of this study should also be considered. First, the number of patients underwent interventional therapy in this single-center study was relatively small, especially in TurboHawk plaque rotation system combined with a drug-coated balloon group. Besides, it was a 2-year single-center analysis, lacking the long-term fellow-up outcome of survival in patients undertook 2 types of surgery. What is more important, there was a shortage of nondiabetic population as control group underwent interventional therapy in this study.
In this study, we compared the efficacy and safety of 2 kinds of interventional therapy in treating Chinese diabetic patients with LEAD. The postoperative outcomes and followed up vascular recanalization in 2-group matched population revealed that compared to applying a drug-coated balloon alone, TurboHawk plaque rotation system combined with a drug-coated balloon could help patients acquire better long-term patency and less major adverse limb events.
Footnotes
Authors’ Note
K.W. participated in the design of the study, conducted the experiments, and drafted the manuscript. X.R. designed the study, revised the manuscript, and is responsible for authenticity of data. Y.L., F.G., H.G., and X.R. collected and analyzed the data. All authors read and approved the final manuscript. The study was approved by the Human Research and Ethics Committee of General Hospital of Ningxia Medical University with adherence to the tenets of the Declaration of Helsinki. Informed consent was obtained from all participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.