
Abstract
To investigate the correlation between ApoE gene polymorphism and the risk of lower extremity arterial disease (LEAD) in T2DM patients of Han nationality in northern China. One hundred and fifty patients with T2DM and 150 patients with T2DM combined with LEAD were enrolled in the study and assigned to the control group and the case group, respectively. The results revealed that the number of epsilon 2 (ε2) genotype carriers in the case group was significantly lower than that in the control group (case vs control: 8.0% vs 15.4%), and the distribution of the ε2 allele frequency was similar to that of the genotype (case vs control: 4.0% vs 8.4%). A binary logistic regression analysis revealed that age, waist-to-hip ratio (WHR), and gender were risk factors for T2DM with LEAD and that the ApoE ε2 carriers was a protective factor (odds ratio [OR] 0.380; 95% confidence interval [CI] 0.162-0.892; P = .026). In male subjects, ε2 carriers were more common in the control group (case vs control:7.8% vs 24.1%), while epsilon 4 (ε4) carriers were more common in the case group (case vs control: 23.3% vs 8.6%); the distribution of frequency of ε2 and ε4 alleles was more common in the control group and the case group, respectively (case vs control: 3.9% vs 12.1%, 12.8% vs 5.2%). In male, age and WHR were risk factors for the disease, and being an ε2 carrier was a protective factor. Being an ApoE gene ε2 carrier is a protective factor for LEAD in male patients with T2DM that are of Han nationality in northern China.
Keywords
Introduction
China has a high incidence of diabetes mellitus, dominated by type 2 diabetes mellitus (T2DM). According to a national epidemiological survey covering 2015 to 2017, the prevalence rate of diabetes in the Chinese population over 18 years of age has reached 11.2%. 1 This suggests that China is faced with a serious situation, and the prevention and treatment of the chronic complications of diabetes are particularly important. Lower extremity arterial disease (LEAD) is one such complication, its risk being double that in non-diabetic patients, 2 and China DIA⁃LEAD study shows that the prevalence of lower limb artery lesions in type 2 diabetes patients over 50 years old in China is 21.2%. 3 It not only causes lower limb ischemic ulcers, gangrene, and amputation, but also increases the risk of cardiovascular events and ischemic stroke, 4 increasing mortality significantly. 5 Therefore, the prevention and treatment of diabetic LEAD is very important, and an in-depth analysis of the factors influencing the disease is required.
In addition to hyperglycemia, smoking, disorders of lipid metabolism, elevated blood pressure, old age and gender are all risk factors for LEAD. It has been found that type 2 diabetes is the result of a combination of non-genetic factors and genetic factors. 6 The risk of LEAD in T2DM patients is also known to vary greatly among individuals and ethnic groups. For example, the incidence of LEAD in black was significantly higher than that in white. 7 As this cannot be explained by environmental risk factors alone, the involvement of genetic factors is suggested. In recent years, Genome-Wide Association Studies (GWAS) concerning T2DM and its complications have been focused on single nucleotide polymorphisms (SNPs). For example, several common SNPs of the SLC2A10 gene have been related to LEAD in T2DM patients. 8
Apolipoprotein E (APOE) gene polymorphism is one of the most widely studied genes associated with type 2 diabetes. 9 The ApoE gene is located in band 2 of region 13 of the long arm of chromosome 19 (19q13.2), and it has two SNPs (rs429358 [p. cys112Arg] and rs7412 [p. Arg158Cys]) and three alleles, epsilon (ε)2(Cys112,158Cys), ε3(Cys112,158Arg), and ε4(Arg112,158Arg), forming six genotypes, ε2/ε2, ε3/ε2, ε3/ε3, ε4/ε2, ε4/ε3, and ε4/4ε, in total. 10 The wild genotype, ApoE ε3/ε3, is the most common, while ε2 and ε4 are two mutant alleles. APOE is a ligand of low density lipoprotein (LDL) receptor, LDL-associated protein, and chylomicron (CM) residue receptor, which is closely related to lipoprotein metabolism. 11 At the same time, ApoE is also involved in the binding process of various lipoproteins to cells, which is an important factor affecting lipid transport and digestion. 12 Researches showed that APOE gene polymorphism affects lipid levels, such as the total cholesterol level of ε4 allele carriers is higher than ε3/ε3 genotype carriers, 13 and the LDL level of ε2/ε2 genotype carriers is significantly lower than ε4/ε4 genotype carriers. 14 We know that abnormal lipid metabolism is one of the important factors of atherosclerosis. Therefore, APOE gene polymorphism is closely related to the occurrence and development of atherosclerosis.
The atherosclerotic diseases of diabetes include coronary heart disease(CHD), cerebral infarction, peripheral artery disease(PAD), kidney disease and so on. At present, most studies on the correlation between ApoE gene polymorphism and T2DM combined with atherosclerotic disease are mainly focused on CHD, 15 diabetic nephropathy, 16 and ischemic stroke(IS). 17 APOE ε4 allele is an independent risk factor for coronary artery disease.11,18 APOE ε2/ε3 genotype may be associated with an increased risk of IS in patients with type 2 diabetes, a Chinese study suggests. 19 There are few studies on the relationship between APOE gene polymorphism and PAD, and the results are somewhat different.For example, Hu et al 20 found that there was no significant correlation between ApoE gene polymorphism and PAD in T2DM, while a study conducted by Koopal et al 21 showed that the ApoE ε2/ε2 variant was associated with an increased risk of PAD in patients with a high risk of cardiovascular disease. Therefore, this study investigates the correlation between ApoE gene polymorphism and the risk of LEAD in patients with T2DM that are of Han nationality in northern China.
Data and Methods
Subjects
A total of 150 patients with T2DM and 150 patients with T2DM combined with LEAD, who were being treated in the Department of Endocrinology of the First Hospital of Hebei Medical University between May 2020 and May 2021, were enrolled in this study and assigned to the control group and case group, respectively. All of them were Han Chinese from northern China, but none of them were related by blood. This study was approved by the Ethics Committee of the First Hospital of Hebei Medical University.
The inclusion criteria were as follows: (1) patients with T2DM; (2) patients ≥30 and ≤75 years old, who had had diabetes for more than five years; and (3) patients who voluntarily participated in the trial and signed the informed consent approved by the Ethics Committee.
The exclusion criteria were as follows: (1) patients with type 1 diabetes mellitus; (2) patients with acute complications of diabetes mellitus; (3) patients with acute cardiovascular and cerebrovascular diseases; (4) patients with severe heart, liver, kidney, or lung failure, or in poor general health; (5) patients with severe infections; (6) patients who had a recent major trauma or surgery; and (7) patients with autoimmune diseases or tumors.
The diagnostic criteria were as follows: (1) T2DM: in line with the 1999 World Health Organization diagnostic criteria; (2) LEAD: a lower extremity arterial ultrasound showed intima-media thickness of each artery ≥1 mm, plaque formation, or lumen stenosis; (3) hypertension: when antihypertensive drugs were not being used, blood pressure was measured more than twice in the resting state, and the average blood pressure was calculated: the systolic blood pressure was ≥140 mm Hg and/or the diastolic blood pressure was ≥90 mm Hg, or previously diagnosed with hypertension and currently using or not using antihypertensive drugs; (4) coronary heart disease: previously diagnosed as having coronary heart disease or the coronary artery stenosis indicated by angiography was >70%; and (5) cerebral infarction: with a previous clear history of cerebral infarction, or brain computed tomography or magnetic resonance imaging that suggested the existence of cerebral infarction.
The Collection of General Clinical Data and Biochemical Data
The clinical data of the subjects, including their gender, age, smoking, and family history, diabetes duration, history of cardiovascular and cerebrovascular diseases, and hypertension were gathered in interviews conducted by trained professionals.
The patients had their height and weight measured in the morning, on an empty stomach and after defecation, wearing only socks and light clothes. Body mass index (BMI) was calculated according to the formula: BMI = weight (kg)/height2 (m2). The waist and hip circumferences were also measured using a tape measure with a minimum scale of 1 mm, and the waist-to-hip ratio (WHR) was calculated according to the formula: WHR = waist circumference (cm)/hip circumference (cm).
All the patients fasted for 12 hours and fasting venous blood was drawn the next morning. Total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C) and triglyceride (TG) levels were measured by automatic biochemical instrument TBA-2000FR (TOSHIBA, Japan). Hemoglobin A1c (HbA1c) was determined by high pressure liquid chromatography (HPLC) using a HbA1c analyzer (BECKMAN COULTER, Au5800, USA). Two ml of venous blood in the EDTA-K2 (Ethylenediamine tetraacetic acid dipotassium) anticoagulant tube was centrifuged at 3000 rpm for 10 minutes, and the blood cells were isolated and placed in a − 80 °C refrigerator.
DNA Extraction and ApoE Genotyping
Deoxyribonucleic acid (DNA) was extracted from the blood cells stored in the −80°C refrigerator using the blood sample DNA extraction kit (Nanjing Zhongkebayer). NanoDrop2000 microuv spectrophotometer was used to measure the photometric value (OD), and THE DNA purity was tested by OD260/OD280.These two SNPs (RS429358 and RS7412) were genotyped by sanger sequencing. Firstly, 500 bp sequences of upstream and downstream of the loci were found on UCSC according to the site information, and the amplification sequencing primers were designed based on this template. Sequencing primers were designed using OMIGA software, and primer synthesis was completed by Beijing Nuohe Xinkang Gene Technology Co., LTD. Amplification reaction was performed by polymerase chain reaction (PCR) :PCR began with initial denaturation at 94°C(5 min), followed by 30 cycles at 95°C(30 s), 65°C-50°C(20 s), 72°C(60 s), 10 cycles at 95°C(30 s), 50°C(20 s), 72°C60 s, and finally extended at 72°C(8 min).After PCR products were purified and sequenced, ABI 3730XL sequencer was used for electrophoresis analysis, and Chromas software was used to interpret the sequencing peak diagram.
Primer sequence (5′-3′): rs429358 (F) GAGACCATGAAGGAGTTGAAGG, (R) CTGCATGTCTTCCACCAGG; rs7412 (F) GAGACCATGAAGGAGTTGAAGG, (R) CTGCATGTCTTCCACCAGG.
These two SNPs determined the three alleles of the ApoE gene: ε2 (rs429358-T + rs7412-T), ε4 (rs429358-C + rs7412-C), and ε3 (rs429358-T + rs7412-C), forming six genotypes. (Figure 1 and 2)
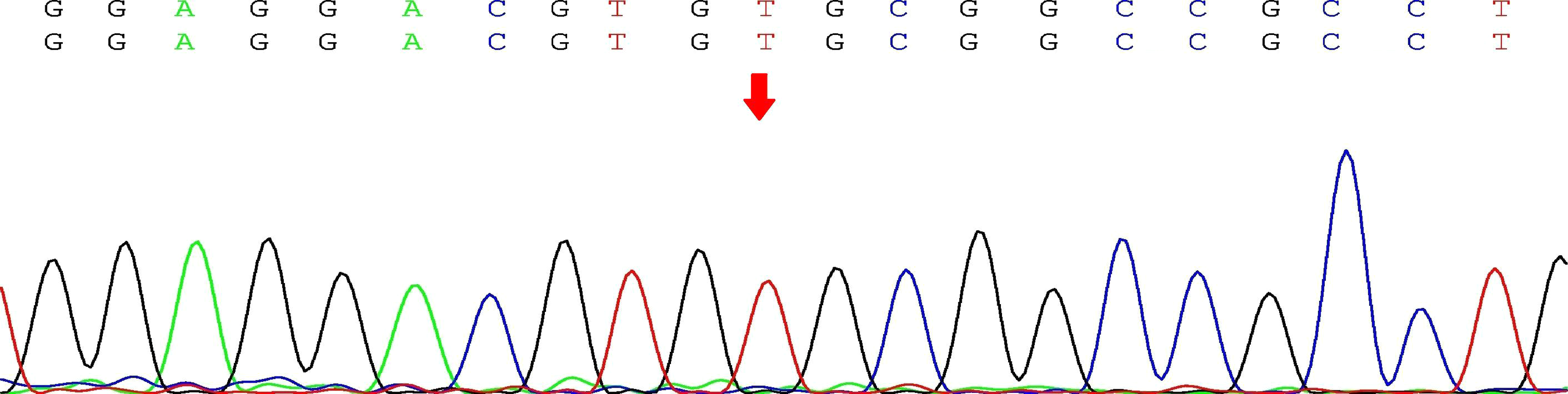
Sequencing peak of rs429358
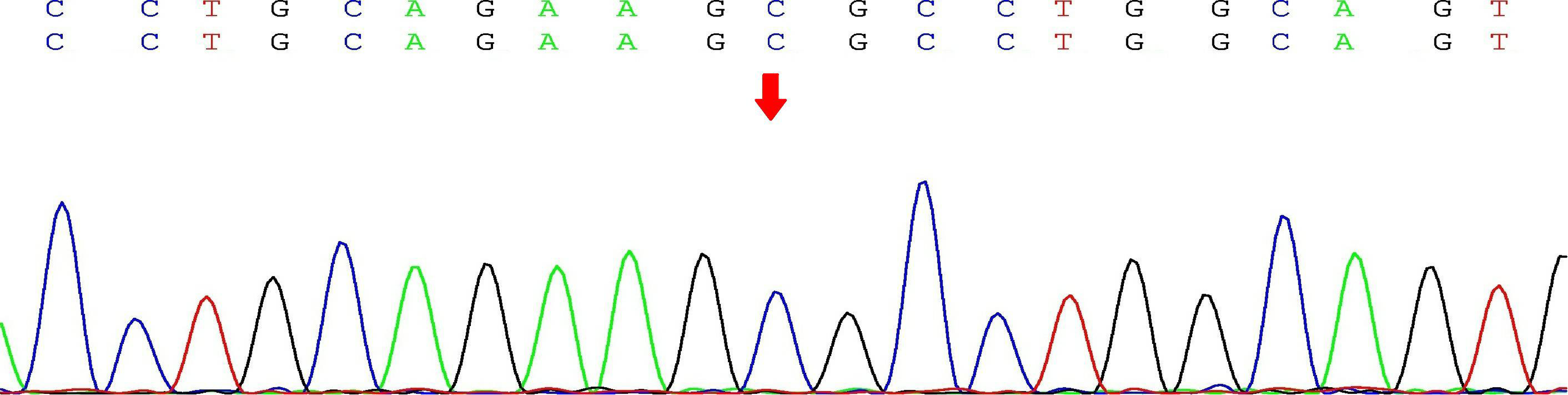
Sequencing peak of rs7412
Statistical Analysis
The data analysis was performed using the SPSS 23.0 statistical software package. If the clinical data, biochemical indexes, and other measurement data of the case group and the control group were normally distributed, they were expressed as the mean ± standard deviation (X ± SD), and comparisons between the two groups were made using an independent sample t-test. The non-normally distributed measurement data were expressed as the median and interquartile range, and the two groups were compared using the nonparametric Mann–Whitney U test. The count data of the two groups were compared using the χ2 test. The relative risk was expressed as the odds ratio (OR) and its 95% confidence interval (95% CI). A binary logistic regression analysis was used to correct the influence of the confounding factors. For all statistical tests, it was set as α = 0.05, and P < .05 was considered statistically significant.
Results
The General Clinical Characteristics and Biochemical Parameters of the Study Population
There were significant differences in gender, age, smoking history, WHR, and duration of diabetes between the case group and the control group (P < .05); however, there were no significant differences in BMI, family history, and the presence of complicated hypertension, CHD, cerebral infarction, and carotid artery disease. In terms of biochemical indexes, there were no differences in HbA1c, TC, HDL-C, and TG between the two groups, but there was a difference in the level of LDL-C (P < .05). The details are noted in Table 1.
Comparison of clinical data and biochemical parameters between T2DM patients and T2DM patients with LEAD

Note: T2DM: type 2 diabetes mellitus; BMI: body mass index; HbA1c: glycosylated hemoglobin; TC: total cholesterol; LDL-C: low density lipoprotein cholesterol; HDL-C: high density lipoprotein cholesterol; TG: triglyceride *P < .05.
The clinical characteristics and biochemical indexes of the male and female patients were compared in terms of gender, and there were significant differences in age, WHR, TC, LDL-C, and cerebral infarction between the male case group and the control group (P < .05). However, the results for the female patients were different, with significant differences in age, WHR, disease duration, and HbA1c (P < 0.05). There were no significant differences between the case group and the control group in the other indexes. The details are noted in Table 2.
Differences in clinical characteristics and biochemical parameters between case group and control group by gender
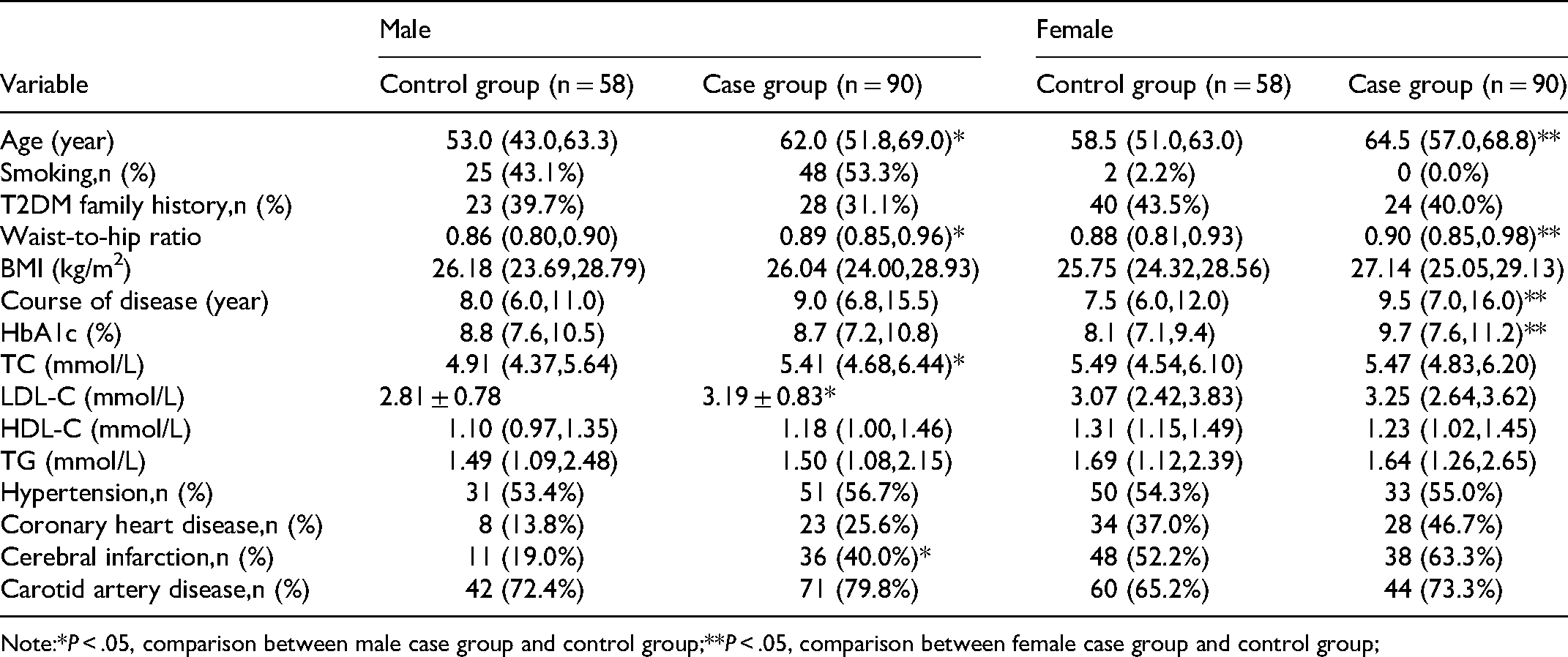
Note:*P < .05, comparison between male case group and control group;**P < .05, comparison between female case group and control group;
The Distribution of Frequency of ApoE Genotypes and Alleles
Due to the small number of people carrying some genotypes (eg, ε2/ε2 and ε4/ε4), the genotypes were combined and analyzed according to the characteristics of the ApoE gene coding proteins. Additionally, the two alleles carried by the genotype ε2ε4 had opposite effects, so one patient with this genotype was excluded. Allele frequencies were estimated by gene counting. The distribution of the frequency of the ApoE genotypes and alleles is given in Table 3. The genotype distribution of all the patients was in accordance with the Hardy–Weinberg equilibrium.
ApoE genotype and allele frequency distribution of subjects

Note:*P < .05, comparison between all subjects in the case group and control group; **P < .05, comparison between male case group and control group; ε2 carriers include carriers of ε2/ε2, ε2/ε3 genotypes; ε3/ε3 refers to carriers of ε3/ε3 genotype; ε4 carriers include carriers of ε3/ε4, ε4/ε4 genotypes.
In all subjects, the ε3/ε3 genotype and the ε3 allele were the most common. There were significant differences between the case group and the control group in the genotype distribution of the ε2 carriers; ε2 carriers were decreased significantly in the case group (P < 0.05). The frequency of ε2 allele in the case group was also significantly lower than that in the control group (P < 0.05).
An analysis was carried out based on gender stratification. Among the male subjects, there were significant differences between the two groups with respect to the ε2 carriers and ε4 carriers. That is to say, the ε2 carriers were more common in the control group, and ε4 carriers were more common in the case group. This was also reflected in the ε2 and ε4 allele frequency distributions (P < 0.05 for all). However, among the female subjects, there was no difference between the two groups in the genotype or the allele frequency distribution.
The Correlation Between ApoE Gene Polymorphism and LEAD in T2DM Patients
In all subjects, compared with the genotype ε3/ε3, which is common in the general population, ε2 carriers and ε4 carriers were not associated with risk for LEAD in T2DM. Although the distribution of ε4 carriers and ε2 carriers was significantly different between the case group and the control group, there was no risk of disease(unadjusted OR = 1.658, 95% CI 0.989-2.782, P = .039). There was a statistically significant difference between the two groups in the distribution frequency of the ε3 and ε2 alleles,but the ε2 allele did not appear to be a risk factor of LEAD (unadjusted OR = 0.623, 95% CI 0.387-1.003, P = .023).Compared to the ε2 allele, the ε4 allele increased the risk of LEAD in T2DM (unadjusted OR = 1.770, 95% CI 1.054-2.974, P = .019) (Table 4).
Correlation between ApoE gene polymorphism and risk of LEAD in T2DM (unadjusted).
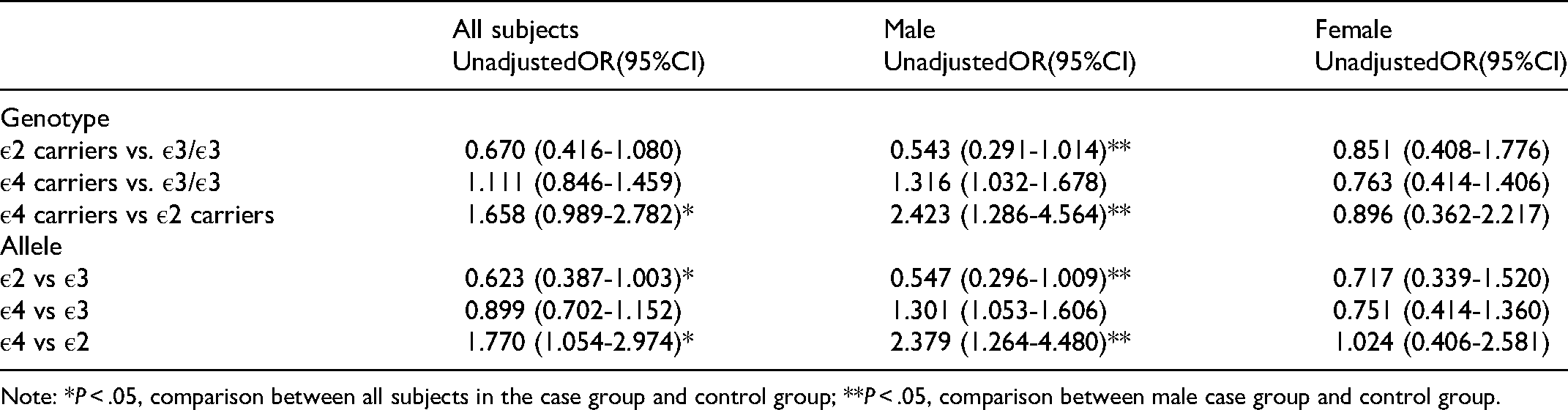
Note: *P < .05, comparison between all subjects in the case group and control group; **P < .05, comparison between male case group and control group.
In the male subjects, compared with the ε2 carriers, the ε4 carriers were at a significant pathogenic risk (unadjusted OR = 2.423, 95% CI 1.286-4.564, P = .001), and, compared to the ε2 allele, the pathogenic risk of the ε4 allele was increased to 2.379 times (unadjusted OR = 2.379, 95% CI 1.264-4.480, P = .001). In the female subjects, the results did not indicate that any genotype or allele may lead to LEAD in T2DM (Table 4).
The risk factors in clinical data and biochemical parameters of patients in the previous results and APOE genotypes were included in binary Logistic regression analysis. The results showed that in all subjects, age (OR = 1.054, 95% CI 1.026-1.082, P < 0.001), WHR (OR = 1.072, 95% CI 1.038-1.108, P < .001), and gender (OR = 2.891, 95% CI 1.540-5.428, and P = .001) were independent risk factors for T2DM with LEAD. Gender was the most important factor, and the pathogenic risk in males was increased by 2.891 times. Among the genotypes, only being an ε2 carrier was a protective factor of the disease (OR = 0.380; 95% CI 0.162-0.892; P = .026), and ε4 carriers were at no pathogenic risk (OR = 1.033, 95% CI 0.511-2.088, P = .929) (Table 5). In male subjects, age (OR = 1.057, 95% CI 1.016-1.100, P = .06) and WHR (OR = 1.066, 95% CI 1.012-1.122, P = .015) were independent risk factors for LEAD, and among the genotypes, being an ε2 carrier was a protective factor (OR 0.260; 95% CI 0.078-0.872; P = .029) (Table 6). In female subjects, age (OR = 1.072, 95% CI 1.029-1.117, P = .001), HbA1c (OR = 1.321, 95% CI 1.096-1.591, P = .003), and WHR (OR = 1.062, 95% CI 1.014-1.112, P = .012) were independent risk factors, and none of the genotypes of ApoE showed a pathogenic risk (Table 7).
Binary logistic regression analysis of risk factors for LEAD in T2DM (all subjects)

Note: * means statistically significant.
Binary logistic regression analysis of risk factors for LEAD in T2DM (male subjects)

Note: * means statistically significant.
Binary logistic regression analysis of risk factors for LEAD in T2DM (female subjects)

Note: * means statistically significant.
Discussion
The diagnosis of LEAD in patients with diabetes usually refers to lower extremity atherosclerotic disease, and the prevalence of LEAD in T2DM patients over the age of 50 in China is as high as 21.2%. 3 However, the diagnosis and treatment of the disease are currently characterized by a low awareness rate, a low treatment rate, and a high disability rate, and the missed diagnosis rate can be as high as 55.7%. 3 The research has increasingly shown that the occurrence and development of T2DM and its complications are the results of the combined action of numerous environmental and genetic factors. As one of the candidate genes for diabetes mellitus, ApoE gene polymorphism can affect the processes of the synthesis, metabolism, and transport of blood lipids, all of which are directly related to premature atherosclerosis. The ε4 allele of the ApoE gene is known to be related to the development of cardiovascular disease. 11 Therefore, considering that both LEAD and coronary artery disease are both atherosclerotic diseases and have a common pathophysiological basis, it is reasonable to speculate that ApoE gene polymorphism may be related to LEAD in patients with T2DM.
In terms of the traditional risk factors for LEAD, previous studies have found that age, smoking, dyslipidemia, and hypertension were associated with PAD.22–24 That's a little different from what we found. In our study,although there were statistically significant differences in age, gender, smoking, WHR, duration of diabetes, and LDL-C level between the case group and the control group, after adjusting these risk factors, only age, gender, and WHR showed pathogenic effects. In other words, older men with abdominal obesity are more likely to have lower limb artery lesions in type 2 diabetes. However, in T2DM female patients, in addition to the influence of age and WHR, the higher the HbA1c level (the poorer the blood glucose control), the more the patients were prone to lower extremity arterial complications. Previous related studies have shown that abdominal obesity is closely related to the increased prevalence of PAD. One study found that if WHR exceeds 0.9, the prevalence of PAD could be doubled. 25 It is also known that WHR is an index of fat accumulation in abdominal organs. Visceral adipocytes may produce and secrete a variety of substances, 26 such as coagulation factors, proinflammatory factors, and lower levels of adiponectin, 27 thus affecting the internal environment of the vascular wall. In addition, the factors produced by adipocytes could affect the gene expression and function of cells maintaining vascular homeostasis, such as endothelial cells, smooth muscle cells, monocytes, and macrophages. 28 These are all mechanisms by which abdominal obesity may lead to atherosclerosis.
In terms of ApoE gene polymorphism, one previous study observed that the frequency of the ε3 allele of ApoE (the wild type) in the Chinese Han population was the highest, and ε2 and ε4 were mutant. 29 This is consistent with the results of this study (ε3 allele frequency was 84.8%). This study established that there was a statistically significant difference in the genotype distribution in male patients alone, that is, there were more ε4 carriers and less ε2 carriers in the case group than in the control group. It was also found that the risk of LEAD was 2.423 times more in male ε4 carriers than in male ε2 carriers. After further control of the nonhereditary risk factors (the clinical characteristics and biochemical parameters), it was seen that ε2 carriers were protected from the disease, but there was no correlation between ε4 carriers and disease. In female patients, the ApoE gene showed no distribution difference; it also did not show any association with LEAD in T2DM. Previous studies on the relationship between ApoE gene polymorphism and diabetic macrovascular complications are mainly focused on CHD and ischemic cerebrovascular disease. For example, one study of the Chinese population revealed that the ApoE ε4 allele was a risk factor for T2DM with CHD and progressive cerebral infarction. 30 However, as one of the macrovascular complications of type 2 diabetes mellitus, there are few studies on the association between LEAD and APOE polymorphism so far. Another study on the Chinese population found that ApoE gene polymorphism was not associated with PAD in T2DM. 20 This is different from the results of our study.The reason for the difference between the findings of that study and the current one may be related to the different gene frequencies caused by the different geographical locations of the study populations, and it may also be related to the limited sample size.
T2DM is thought to be the result of the interaction of various genetic and environmental factors, and this study showed that the OR value of the significant risk factors did not increase significantly, supporting the idea that LEAD in T2DM is not caused by a single factor but a superposition of multiple factors.
In terms of its limitations, the research population of the present study only consisted of T2DM patients, and, therefore, the findings may not be applicable to healthy people or people with other diseases. Secondly, this study collected samples from the Han population in northern China, and the genetic association that was found may not extend to other regional or ethnic populations. Finally, although there are, at present, few studies on the relationship between ApoE gene polymorphism and LEAD in T2DM, the results of this study differ from the previous findings, possibly due to its limited sample size. Consequently, further research with a larger sample size is necessary.
Conclusion
In summary, this study found that, in male patients with T2DM that are of the Han population in northern China, being an ApoE gene ε2 carrier can be a protective factor against developing LEAD. However, in female patients with T2DM, ApoE gene polymorphism was not found to be associated with LEAD. These findings mean that, by combining ApoE gene test results with traditional risk factors, a clinical prediction model that will enable the early prediction and prevention of LEAD in male patients with T2DM can be developed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The study was supported by The Science and Technology project of the People's Livelihood in Hebei Province (20377707D), Special Funding for Local Science and Technology Development Guided by the Central Government (199477139G), Natural Science Foundation of Hebei Province (H2020206224 and H2018206358), Projects of introducing foreign intelligence into Hebei Province (2019YX007A) and Medical Science Research Project of Hebei Province in 2022 (NO.20221810).
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of the First Hospital of Hebei Medical University (No: 20190444). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for Publication
All participants signed a document of informed consent.