
Abstract
Patients with von Willebrand disease (VWD) often require treatment with supplemental von Willebrand factor (VWF) prior to procedures or to treat bleeding. Commercial VWF concentrates and more recently recombinant human VWF (rVWF) have replaced cryoprecipitate as the mainstay of therapy. In comparison with cryoprecipitate, the VWF content and multimer distribution under current manufacturing processes of these commercial products has not been reported. We measured the factor VIII (FVIII:C), VWF antigen (VWF:Ag), VWF collagen-binding activity (VWF:CB), VWF platelet-binding activity by GPIbM enzyme-linked immunosorbent assay (VWF:GPIbM), and percentage of high-molecular-weight (HMWM) VWF in 3 pools of group A and O cryoprecipitate, 3 vials of VWF concentrate (Humate-P), and 1 lot of rVWF (Vonvendi). We found that both group O and group A cryoprecipitate have significantly higher ratios of VWF:GPIbM activity and FVIII:C activity relative to VWF:Ag and have better preservation of HMWM than Humate-P. Although not compared statistically, rVWF appears to have more HMWM VWF and a higher ratio of VWF:GPIbM to VWF:Ag than Humate-P and cryoprecipitate. The estimated acquisition cost for our hospital for treating one major bleeding episode was more than 4-fold higher with Humate-P and 7- to 10-fold higher with rVWF than with cryoprecipitate.
Keywords
Introduction
von Willebrand disease (VWD) is a common inherited bleeding disorder characterized by quantitative or qualitative defects in von Willebrand factor (VWF), a large multimeric plasma glycoprotein that supports platelet adhesion to the subendothelium and protects factor VIII (FVIII) from cleavage in the blood through noncovalent bonding.
Treatment of VWD focuses on restoration of VWF and FVIII levels through release of endogenous VWF and FVIII with desmopressin, or replacement with exogenous VWF and FVIII for prophylaxis to prevent bleeding, when bleeding occurs, or prior to invasive procedures. Adjuvant treatments (such as antifibrinolytic therapies) that promote hemostasis without altering factor levels are also used. The majority of patients with type 1 VWD respond to treatment with desmopressin; however, treatment for patients with more severe types includes replacement of VWF and FVIII, as well as use of adjuvant therapies. Replacement therapy is first-line treatment for patients with type 3 VWD (in whom VWF production is completely absent) and most patients with type 2 VWD (who produce qualitatively defective VWF), as well as other patients who are unresponsive to or unable to receive desmopressin.
Historically, cryoprecipitate, which has higher concentrations of fibrinogen, FVIII, and VWF than plasma, was used as factor replacement in patients with VWD. 1 Treatment with cryoprecipitate was shown to normalize FVIII levels and VWF antigen levels and stop bleeding. 2 –4 However, with concerns in the 1980s about transfusion-associated infections, virus-inactivated plasma-derived concentrates, which contain VWF and FVIII, became preferred for factor repletion. 5 Over the past 20 years, these concentrates have become the standard of care, and recent treatment guidelines for VWD often fail to mention cryoprecipitate as a potential therapy 6 or suggest its use only when concentrates cannot be obtained. 7,8
More recently, recombinant human von Willebrand factor (rVWF) was developed to overcome several of the limitations of plasma-derived concentrates, specifically the variability of VWF:Ag-to-FVIII:C ratios between different products and between lots of the same product, the invariable loss of ultra-large-high and high-molecular-weight von Willebrand multimers (ULM and HMWM-VWF) 9 and the residual infectious risks associated with plasma-derived therapies. Other proposed benefits of rVWF are longer half-life compared with plasma-derived VWF concentrates and the independent titration of VWF and FVIII levels during treatment of VWD, as patients treated with either plasma-derived factor replacement or cryoprecipitate may develop elevated levels of FVIII, a potential risk for thromboembolic complications. 10 –12 Endogenous FVIII is stabilized with replacement of VWF and thus normalization of both levels can occur with VWF treatment alone. 13
In clinical trials, treatment for VWD with cryoprecipitate, plasma-derived concentrates, and rVWF have all resulted in high rates of excellent hemostatic response and these treatments are all generally well tolerated with low rates of adverse events. 4,14 –17 Thus, the optimal therapy remains uncertain. Restoration of HMWM VWF multimers, the most hemostatically active multimers, has been considered one important component of effective therapy, although in vivo data demonstrating the necessity of restoring HMWM VWF for effective hemostasis have varied. Initial characterization of VWF in commercial concentrates and cryoprecipitate found significant differences in HMWM VWF concentration. 18 However plasma processing methods, which affect VWF yields, have evolved since those early studies. Recent studies, which directly compared VWF concentrates and rVWF, did not include cryoprecipitate. 19,20 In the modern era of nucleic acid screening of blood donors, the risk of transfusion-transmitted infections of known pathogens has become negligible, 21 and thus, the role of cryoprecipitate in the treatment of VWD deserves reconsideration.
To address this, we performed a pilot, blinded, direct comparison study of the content and quality of VWF and FVIII in cryoprecipitate, a plasma-derived commercial VWF concentrate, and rVWF (Vonvendi). Humate-P was used in the study as the plasma-derived commercial VWF concentrate because it contains the highest ratio of VWF:RCo activity relative to FVIII:C of commercial concentrates available in the United States and is routinely used at our institution for the treatment of VWD. The purpose of this pilot study was to establish the basis for further work evaluating the potential role of cryoprecipitate and the importance of HMWM VWF replacement in the treatment of VWD.
Materials and Methods
Laboratory Evaluation
Pooled cryoprecipitate (5 units per pool) was obtained from the American Red Cross and stored at −25°C. Aliquots were taken approximately 4 hours after thawing. Three pools of group A and 3 pools of group O cryoprecipitate were sampled. Aliquots from 3 vials of Humate-P were sampled. All Humate-P samples were reconstituted according to the manufacturer’s instructions. All cryoprecipitate and Humate-P aliquots were stored at −80°C, coded, and subsequently sent frozen to the Hemostasis Reference Laboratory at the Versiti Blood Center of Wisconsin (Milwaukee, Wisconsin) for testing. A single lot of rVWF was reconstituted according to the manufacturer’s instructions at the Hemostasis Reference Laboratory and underwent a freeze–thaw cycle. All samples were thawed and prediluted before being assayed. Prior to the study, the laboratory validated that levels of VWF:GPIbM, VWF:Ag, and VWF:CB are preserved through 3 freeze–thaw cycles. VWF:Ag was performed by enzyme-linked immunosorbent assay. 22 FVIII:C activity was performed by a one-stage clotting assay. 23 Ligand binding assays were performed as previously described, including VWF:CB 22 and VWF:GPIbM. 24,25 Because only a single lot of rVWF was available, it underwent repeat testing for each assay. The VWF multimers were separated by sodium dodecyl sulfate agarose gel electrophoresis and quantified using monoclonal antibodies with chemiluminescent detection and densitometry analysis (samples were adjusted to VWF:Ag content). The HMWM VWF were defined as multimers that migrated slower than the smallest 10 bands on gel electrophoresis, corresponding to molecular weight of greater than 6000 kd. 26
Cost Analysis
The cost of cryoprecipitate and Humate-P was determined by the acquisition cost of the product to the Blood Transfusion Service of Massachusetts General Hospital on March 1, 2018. Cost of rVWF was determined by an acquisition estimate given to Blood Transfusion Service in November 2018 as the product is not in the hospital’s inventory. Additional costs of storage (freezer for cryoprecipitate, refrigerator for Humate-p and rVWF), thawing, or reconstitution of products were not included as all products require similar storage and preparation time.
Statistical Analysis
Cryoprecipitate and Humate-P data were evaluated by one-way analysis of variance. The mean ratio of VWF:CB to VWF:Ag, VWF:GPIbM to VWF:Ag, and FVIII:C to VWF:Ag, and the percentage of HMWM VWF were compared between Group O cryoprecipitate, Group A cryoprecipitate, and Humate-P. When statistically significance differences were found (P ≤ .05), results were compared pairwise with Tukey post hoc test to determine significant pairwise differences (P ≤ .05). The rVWF was not included in this statistical analysis because only a single lot of rVWF was tested. This was a pilot study and sample size considerations were not undertaken. Comparisons between rVWF and the other products are descriptive only.
Results
Comparison of In Vitro Assays of Cryoprecipitate, Humate-P, and rVWF
The FVIII:C activity, VWF:Ag, VWF:CB, VWF:GPIbM, and distribution of VWF multimers were measured in 3 samples of Humate-P, 3 pools of blood group A cryoprecipitate, 3 pools of blood group O cryoprecipitate, and 1 lot of rVWF. Table 1 gives the mean ratio of VWF:CB to VWF:Ag, VWF:GPIbM to VWF:Ag, FVIII:C to VWF:Ag, and the percentage of HMWM of the 3 lots of cryoprecipitate and Humate-P. Because only a single lot of rVWF was tested, the mean value of repeat tests on the same lot is given. We used the ratio of each functional assay to VWF:Ag to normalize for the different concentrations of VWF:Ag in each product. The VWF:GPIbM activity assay measures binding of VWF to mutant GPIbM without ristocetin. We used this assay because while it assesses the platelet binding activity of VWF similarly to the VWF:RCo assay (with excellent correlation between the assays), 27 it is considered more precise and sensitive. 28
Hemostatic Parameters in Cryoprecipitate, Humate-P, and Recombinant von Willebrand Factor (rVWF).a

Abbreviations: FVIII:C, factor VIII; HMWM VWF, high-molecular-weight von Willebrand factor; rVWF, recombinant von Willebrand factor; VWF:Ag, VWF antigen; VWF:CB, collagen binding; VWF:GPIbM, mutant glycoprotein Ib.
a Data are reported as mean ± standard deviation.
b Mean values of repeat testing of one lot of rVWF are presented in this column. FVIII:C activity was not tested because rVWF does not contain FVIII.
c P < .05, compared with Humate-P.
d P < .01, compared with Humate-P.
e P < .001, compared with Humate-P.
The results show that the mean ratio of VWF:GPIbM to VWF:Ag and the percentage of HMWM in blood group A (P < .01 for both comparisons) and O cryoprecipitate (P = .03, P < .01, respectively) were significantly higher than in Humate-P. Both cryoprecipitate groups also contained significantly more FVIII:C relative to VWF:Ag than Humate-P (P < .001 for both blood groups). There were no significant differences in the ratio of VWF:CB to VWF:Ag between cryoprecipitate and Humate-P. There were no significant differences between group O and group A cryoprecipitate; however, group A cryoprecipitate had a nonsignificantly higher average VWF:GPIbM to VWF:Ag ratio and VWF:CB to VWF:Ag ratio, which is consistent with known correlations between blood group and amount of plasma VWF. As shown in Figure 1, VWF multimer analysis demonstrated superior preservation of HMWM in cryoprecipitate compared with Humate-P.
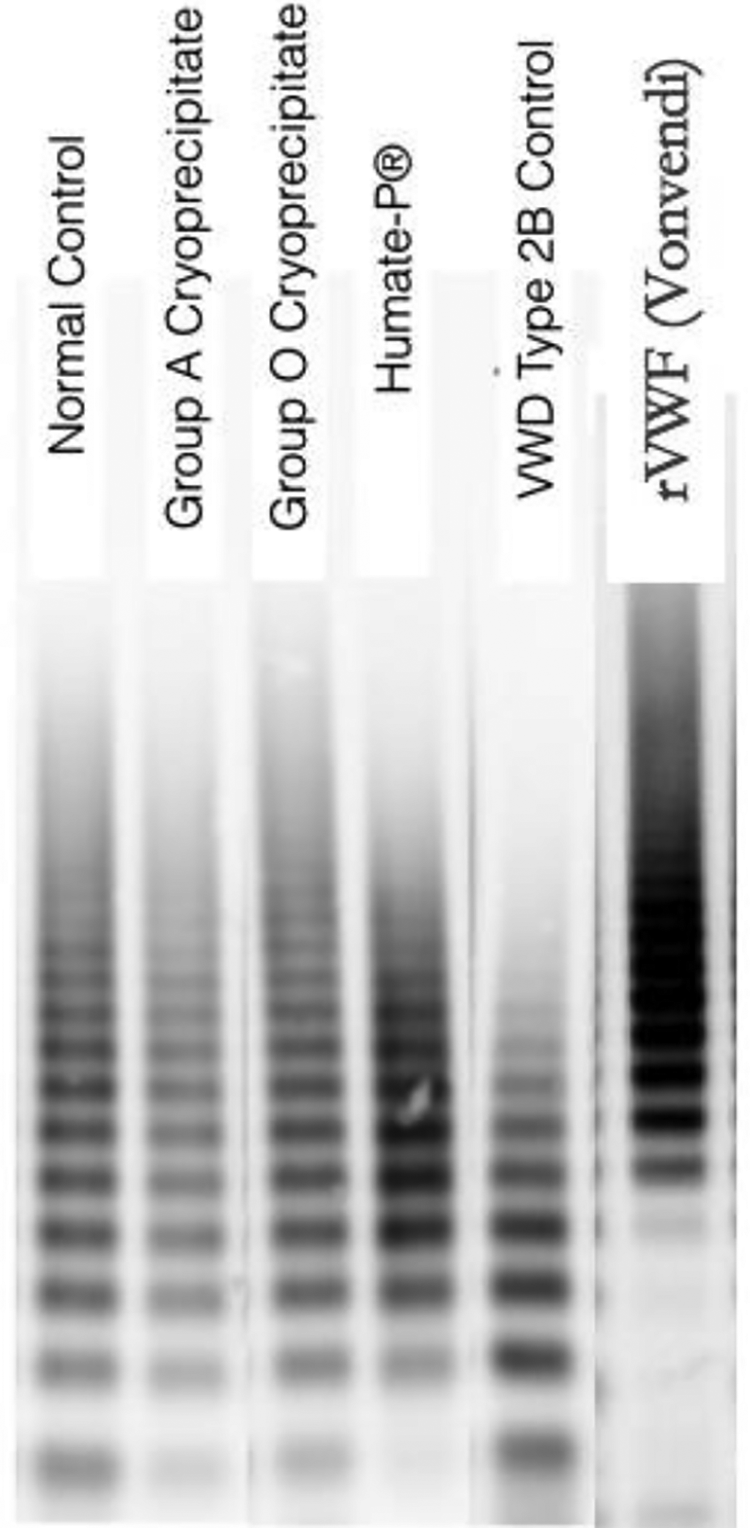
Multimer analysis of von Willebrand factor in normal plasma, group A and O cryoprecipitate, Humate-P, patient with type 2B von Willebrand disease, and recombinant von Willebrand factor (Vonvendi).
Because only a single lot of rVWF was assayed, we did not statistically compare the measured differences between rVWF and the other products; however, the mean ratio of VWF:GPIbM to VWF:Ag and the percentage of HMWM in rVWF was greater in the lot tested than in cryoprecipitate and Humate-P (Table 1). This is consistent with recent comparisons of Humate-P and rVWF and the known preservation of ULM and HMWM VWF in rVWF because the protein is not exposed to ADAMTS13 during its manufacturing.
Cost Evaluation
Table 2 shows the acquisition cost of cryoprecipitate, Humate-P, and rVWF for treatment of a 70-kg patient with type 2 or 3 VWD presenting with a minor (a single dose of 40 IU VWF:RCo/kg) and major bleed (3-day course: 60 IU VWF:RCo/kg loading dosing, followed by 50 IU VWF:RCo/kg every 12 hours for 72 hours). These treatment schedules were derived from the recommended dosing for a minor or major bleed in patients with type 2 or type 3 VWD in the Humate-P and rVWF package inserts. Of note, dosing for major bleeding according to the prescriber information for Humate-P is a 7-day course, while rVWF prescriber information recommends treatment for 2 to 3 days.
Hospital Acquisition Cost of Humate-P, Cryoprecipitate, and rVWF for Treatment of a 70-kg Patient.
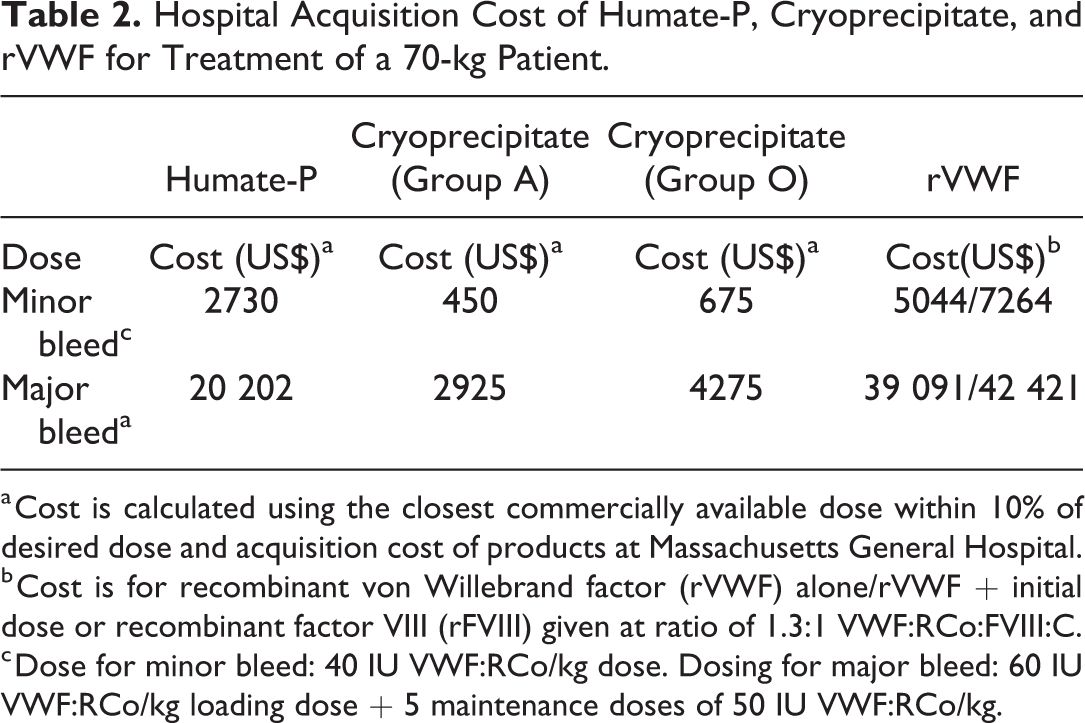
a Cost is calculated using the closest commercially available dose within 10% of desired dose and acquisition cost of products at Massachusetts General Hospital.
b Cost is for recombinant von Willebrand factor (rVWF) alone/rVWF + initial dose or recombinant factor VIII (rFVIII) given at ratio of 1.3:1 VWF:RCo:FVIII:C.
c Dose for minor bleed: 40 IU VWF:RCo/kg dose. Dosing for major bleed: 60 IU VWF:RCo/kg loading dose + 5 maintenance doses of 50 IU VWF:RCo/kg.
The costs of Humate-P and rVWF were estimated by using acquisition costs of the closest available commercial dose (within 10% of the recommended IU of VWF:RCo). Because VWF:RCo content is not labeled on cryoprecipitate and VWF:RCo is labeled on Humate-P and rVWF, in our calculations, we assumed the measured VWF:GPIbM content was equivalent to the VWF:RCo content. In our cost estimation for rVWF, we report 2 costs, one for the cost of rVWF alone and the second including a single initial dose of rFVIII because for bleeding episodes coadministration of rFVIII with the first dose of rVWF is recommended when a patient has a known secondary deficiency of FVIII or baseline levels of FVIII are unknown. The dose of rFVIII was based on dosing used in clinical studies of rVWF in bleeding, in which rVWF and rFVIII were administered at a ratio of 1.3:1 (VWF:RCo:FVIII:C). 17
At our institution, the cost for treatment of VWD with Humate-P is more than 4-fold greater and with rVWF (without rFVIII) more than 7-fold greater than treatment with cryoprecipitate. For a minor bleed, this translates into more than US$2000 difference between cryoprecipitate and Humate-P and US$4400 between cryoprecipitate and rVWF (US$6,500 when including the cost of rFVIII) and for a major bleed into almost US$16 000 and US$34 000 (US$38 000 with rFVIII) difference respectively.
Discussion
In this pilot study characterizing the in vitro VWF content of cryoprecipitate, Humate-P, and rVWF under current manufacturing processes, we found that cryoprecipitate has significantly higher ratios of VWF:GPIbM activity and FVIII:C activity relative to VWF:Ag and has better preservation of HMWM compared with Humate-P. Although not compared statistically, our characterization of Humate-P and rVWF agrees with recent comparisons of the products, which demonstrated that rVWF has significantly more HMWM VWF and a higher ratio of VWF:RCo:VWF:Ag. 20 We also found that rVWF appears to contain more HMWM VWF and has a higher ratio of VWF:GPIbM activity to VWF:Ag than cryoprecipitate. Interestingly, despite these in vitro differences and incomplete correction of bleeding time in many patients, treatment with each of these therapies appears to be effective for most patients with VWD.
However, the costs of each therapy are not equal and treatment with Humate-P or rVWF is associated with a dramatically higher acquisition cost. When considering the best treatment, the decision is not based on cost alone but is multifactorial including safety, efficacy, ease of administration, and other factors. In treatment of VWD, restoration of more normal VWF multimer distribution has been one aspect used to identify more optimal therapies as the hemostatic potential of VWF is related to multimer size. With loss of HMWM VWF, there is a concomitant decrease in VWF function (even with normal VWF Ag levels). While it was shown in early assessments of concentrates (including Humate-P) that they had reduced levels of the HMWM multimers compared to cryoprecipitate or plasma, 29 –31 the importance of HMWM in the treatment of VWD remains uncertain. Normalization of plasma multimers does not consistently result in normalization of bleeding time, 32,33 and some studies suggest that platelet levels of VWF may correlate better with bleeding time than plasma levels. 3,34
Our study has several limitations. As a pilot study, the sample size is small and larger studies are required to confirm these results. It is possible that, prior to laboratory analysis, degradation of VWF or FVIII occurred and therefore our result might underestimate the actual level of VWF. Furthermore, we only analyzed plasma-derived VWF concentrate from one manufacturer. The clinical implications of these in vitro results are uncertain and therefore clinical outcomes looking at these treatments would be of great value in helping clinicians decide how to treat patients with VWD. Finally, our cost estimates are based on the dosing schedule recommended in the product insert, while real-life dosing may be adjusted by monitoring factor levels of patients on therapy. Monitoring may result in dose reductions (or increases) and therefore actual costs may differ from our estimates.
In summary, several options exist for VWF replacement. In the modern era of nucleic acid screening of blood donors, the risk of transfusion-transmission of known infections has become negligible; however, the risk of unknown pathogens may be reduced by viral inactivation methods used in preparation of plasma-dervied VWF products and is eliminated with the use of rVWF. However, our preliminary findings show that cryoprecipitate supplies greater amounts of HMWM VWF than commercial concentrates and would be expected to restore VWF and FVIII levels at an appreciably lower cost than Humate-P and rVWF. Ultimately, our results highlight the need for new studies comparing the clinical response following treatment with different products capable of replacing VWF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.