
Abstract
von Willebrand factor (vWF) is a multimeric glycoprotein present in blood plasma. It is synthesized in megakaryocytes and endothelial cells, secreted into circulation in the form of high-molecular-weight multimers (HMWMs), and cleaved into shorter, less active multimers by ADAMTS13. It is essential for platelet adhesion and aggregation. Previous studies have investigated the relationship between vWF levels and thromboembolic events with little regard to vWF multimeric structure. Patients with atrial fibrillation (AF) exhibit higher plasma vWF and lower ADAMTS13 levels. One hundred seven patients with AF, 51 anticoagulated and 56 nonanticoagulated, were eligible for the study. Plasma samples were analyzed for vWF antigen, vWF activity, and ADAMTS13; vWF multimers were analyzed by Western blot in 1% to 1.3% sodium dodecyl sulfate agarose gel electrophoresis. Patients with AF without oral anticoagulation (OAC) had significantly higher vWF plasma levels (154.00 [75-201] UI/dL) and vWF activity (60.00% [20%-210%]) compared to patients with OAC (133.50 [90-192] UI/dL, P = <.001; 50.00% [20%-160%], P = .02). Both were specially decreased in patients treated with acenocumarin. Patients without OAC also showed lower ADAMTS13 levels and presence of vWF HMWMs. Patients with AF show higher plasma levels and vWF activity. Moreover, treatment with traditional OAC (acenocumarin) significantly reduced vWF levels. Patients without OAC might have an increased risk of thrombotic events showing lower ADAMTS13 and higher vWF levels. Patients with stroke had higher plasma levels, vWF activity, and HMWMs. Our study suggests that increased vWF levels and presence of HMWMs could be related to cerebrovascular disease and may represent useful biomarkers for stroke in AF.
Introduction
von Willebrand factor (vWF) is a plasmatic multimeric glycoprotein produced in endothelial cells and megakaryocytes. VWF mediates adhesion and aggregation of platelets at sites of vascular injury. 1 –3
The molecule shows binding sites for coagulation factor VIII and platelet glycoproteins Ib/IX and IIb/IIIa, with 2 sites for collagen and 2 more for heparin. 2,4
vWF has 2 well-established biological functions: mediating adhesion and aggregation of platelets and acting as a carrier for factor VIII, protecting it from degradation, cellular uptake, or binding to the surface of activated platelets and endothelial cells. 2,5 Recent studies have provided evidence indicating that vWF regulates not only hemostasis and thrombosis but also the processes of angiogenesis, smooth muscle cell proliferation, tumor cell metastasis, and immune cell regulation. 2,6
Atrial fibrillation (AF) is the most commonly sustained cardiac arrhythmia and is associated with a high risk of stroke and thromboembolism. 7,8 Elevated vWF concentrations are associated with cardiovascular disease, 9 increased risk of ischemic heart disease, and the occurrence of acute ischemic stroke 10 ; these high levels of vWF are associated with the risk of stroke, even in the general population. 11
The biological function of vWF depends largely on the size of its multimers. 12 High-molecular-weight multimers (HMWMs) are the most efficient in hemostasis. Larger multimers are more likely to bind to platelets and subendothelial collagen and to promote platelet adhesion in circulating blood. Ultralarge vWF multimers (ULvWF) are also more active to induce platelet aggregation. 4,13
ADAMTS13 is a multidomain protease that is remarkably specific for vWF. 14,15 ADAMTS13 targets the A2 domain of vWF and specifically cleaves the protein between Tyr1605-Met1606, reducing the ULvWF to smaller and less active forms. 2 The failure to cleave large multimers will promote thrombosis. 16
Mean plasma level of vWF is 100 UI/dL, but the distribution among general population is broad, with 95% of values between 50 and 200 UI/dL. 17 In AF, vWF plasma concentrations have been found increased in several groups, with a mean of 146 UI/dL and values between 77 and 245 UI/dL. 18
Numerous studies have investigated the relationship between vWF levels and thromboembolic cardiovascular events; vWF is significantly predictive of adverse cardiac events, including death, but had mainly focused on vWF levels without regard to multimeric structure. Patients with AF exhibit higher plasma vWF and lower ADAMTS13 antigen levels.
Methods
Study Patients
Between January 2014 and December 2015, patients with nonvalvular AF and at least 1 risk factor for stroke were enrolled in this study. We included ambulatory patients with AF who had been previously evaluated by a specialist outpatient clinic and were treated with oral anticoagulation (OAC) at the Hospital General “Dr Miguel Silva.” Exclusion criteria were inflammatory or neoplastic disease; patients younger than 45 years; hematologic, renal, or hepatic impairment; and any acute infection. Accordingly, 107 patients were eligible for the study.
All patients underwent complete clinical evaluation. Blood samples were obtained from all patients and plasma was separated for analysis. Informed consent was obtained from each patient, and the study was performed according to the ethical principles for medical research stipulated in the Declaration of Helsinki and local guidelines and approved by the local ethics committee.
Diagnosis of AF was made based on an electrocardiographic report with AF at least 2 times (with at least 2 weeks between both reports). Echocardiographic monitoring was used to rule out valvular abnormalities. The AF was defined according to the consensus 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society guideline for the management of patients with AF. 19 Clinical risk factors were recorded, and risk scores were calculated. 20 In brief, Congestive heart failure, Hypertension, Age 75 years, Diabetes, previous Stroke (CHADS2) and CHA2DS2-Vascular disease, Age 65-74 years, sex category (CHA2DS2-VASc) were calculated as an index of risk of stroke in patients with AF, ranging from 1 to 6 and 1 to 9, respectively, with higher scores indicating a greater risk of stroke.
Patients were divided into 2 groups, those receiving OAC and newly diagnosed patients with AF who were still not anticoagulated; patients with acute stroke and AF who arrived to the emergency department were also included in this group. Furthermore, the OAC group was divided according to the drug that was prescribed such as rivaroxaban (15-20 mg/d according to renal function) or acenocumarin (adjustable dosage for a target international normalized ratio [INR] of 2.0-3.0) groups. The anticoagulant for each patient was prescribed according to the treating physician’s criteria.
Blood Sampling and Laboratory Analysis
Blood was sampled on the day of the examination. Whole blood samples were collected by venipuncture into tubes containing 3.8% sodium citrate and centrifugated at 3500 rpm for 10 minutes at room temperature. Plasma was immediately separated and stored at −80°C until assayed (approximately 6-8 months). Commercially available enzyme-linked immunosorbent assay (ELISA) kits were used to measure vWF plasma levels (IMUBIND vWF ELISA; Sekisui American Diagnostics, Stamford CT), vWF activity (IMUBIND Activity ELISA; Sekisui Diagnostics, Stamford CT), and ADAMTS13 levels (IMUBIND ADAMTS13 ELISA; Sekisui Diagnostics, Stamford CT). Normal plasma from a pool of healthy donors (NPP) was used as the standard for vWF multimer analysis.
von Willebrand Factor Multimer Analysis
vWF multimers were separated by electrophoresis using a 1% stacking and a 1.8% running separating sodium dodecyl sulfate agarose gel in a vertical MiniProtean Cell (BioRad, USA). The same concentration of vWF antigen was loaded for each sample, based on vWF plasma levels for each patient. Subsequently, proteins were transferred to a polyvinylidene fluoride nylon membrane using semidry transfer conditions (Tans-Blot SD SemiDry Transfer Cell; BioRad), and the multimers were detected using a polyclonal rabbit antihuman vWF antibody (Dako, Glostrup, Denmark) and polyclonal swine antirabbit horseradish peroxidase–labeled immunoglobulins (Dako). The HMWMs were visualized by chemiluminescence using Image Lab software 5.2.1. The multimers were determined and compared with NPP multimers. Finally, the multimeric pattern was evaluated by densitometric analysis.
Statistical Analysis
SPSS 18.0 for Windows was used for statistical analysis. Continuous variables are expressed using mean, standard deviation, median, minimum, and maximum values; categorical variables are expressed using frequencies and percentages. Shapiro-Wilk test was used for normality test. Kruskal-Wallis test was used for comparison of 3 or more groups, and Mann-Whitney U test was used for group comparisons unless otherwise stated. The Spearman correlation coefficient was calculated to determine the relationship between 2 parameters. A P value <.05 was considered to be statistically significant.
Results
One hundred seven patients were enrolled in this study. Patients were classified into 2 groups based on OAC or non-OAC treatment. A total of 51 (47.66%) patients received OAC; of these, 68% were treated with acenocumarin (INR 2.12 [±0.866]) and the remaining 32% with rivaroxaban. Fifty-six (52.3%) patients did not receive OAC. Clinical and demographic characteristics of the study population are shown in Table 1.
Clinical and Demographic Characteristics.a
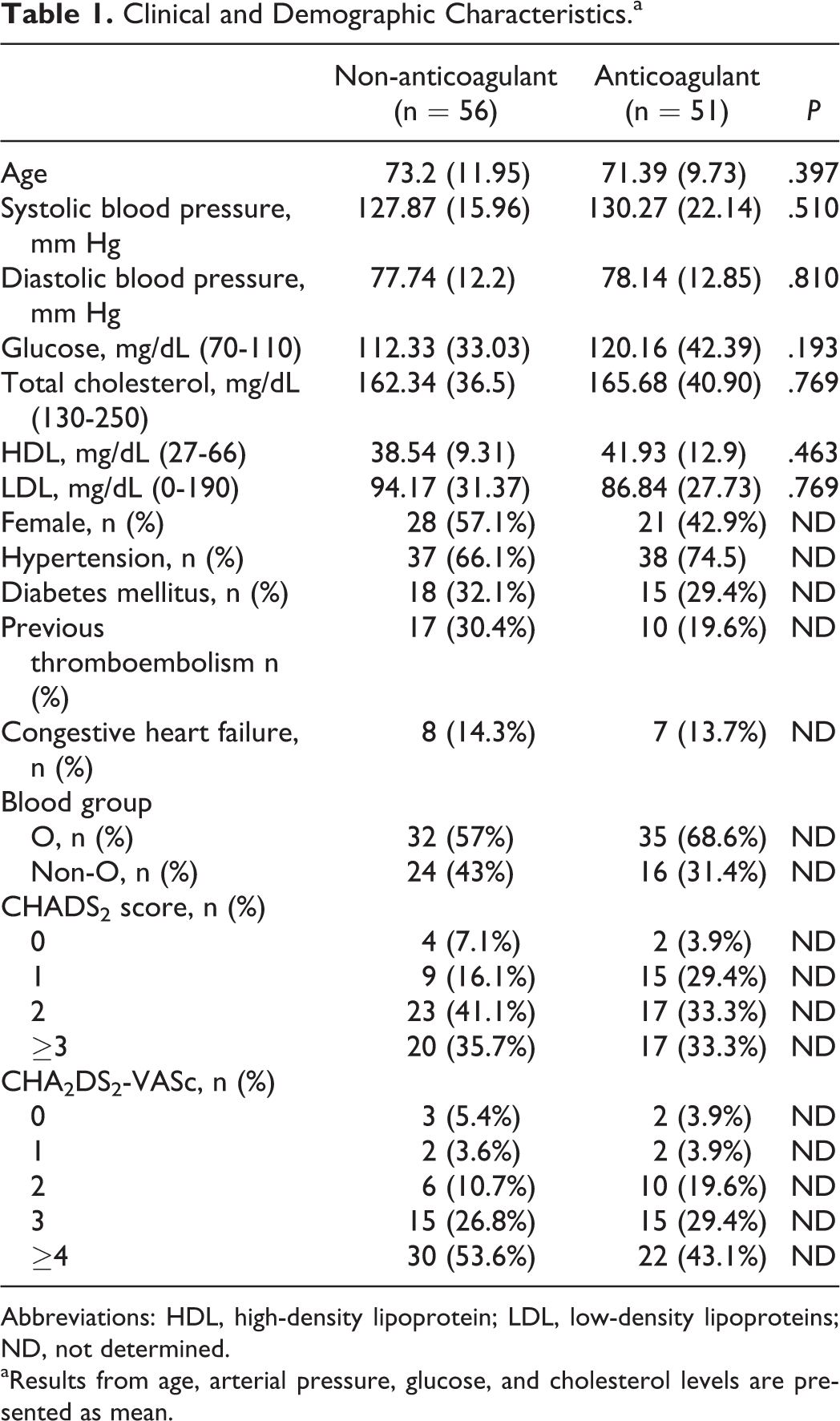
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoproteins; ND, not determined.
aResults from age, arterial pressure, glucose, and cholesterol levels are presented as mean.
Median ages of the patients were not significantly different between the groups (P = .397); both groups were similar regarding clinical and demographic characteristics. Blood group was similar in both groups. CHADS2 and CHA2DS2-VASc scores were similar in both groups and were not associated with OAC. Approximately 25.5% of patients had a history of stroke, transient ischemic attack, or systemic embolism, and 12.5% were diagnosed with acute stroke.
von Willebrand Factor Parameters
vWF plasma concentrations were significantly higher in patients without OAC (154.00 [75-201] UI/dL) when compared to patients with OAC treatment (133.50 [90-192] UI/dL, P = <.001; Table 2). The vWF activity exhibited similar behavior, being significantly higher in nonanticoagulated patients (60.00% [20%-210%] and 50.00% [20%-160%], P = .02).
Plasma Levels of von Willebrand Factor (vWF), vWF Activity, ADAMTS13, and vWF Multimers in Patients With AF With and Without Oral Anticoagulation.a
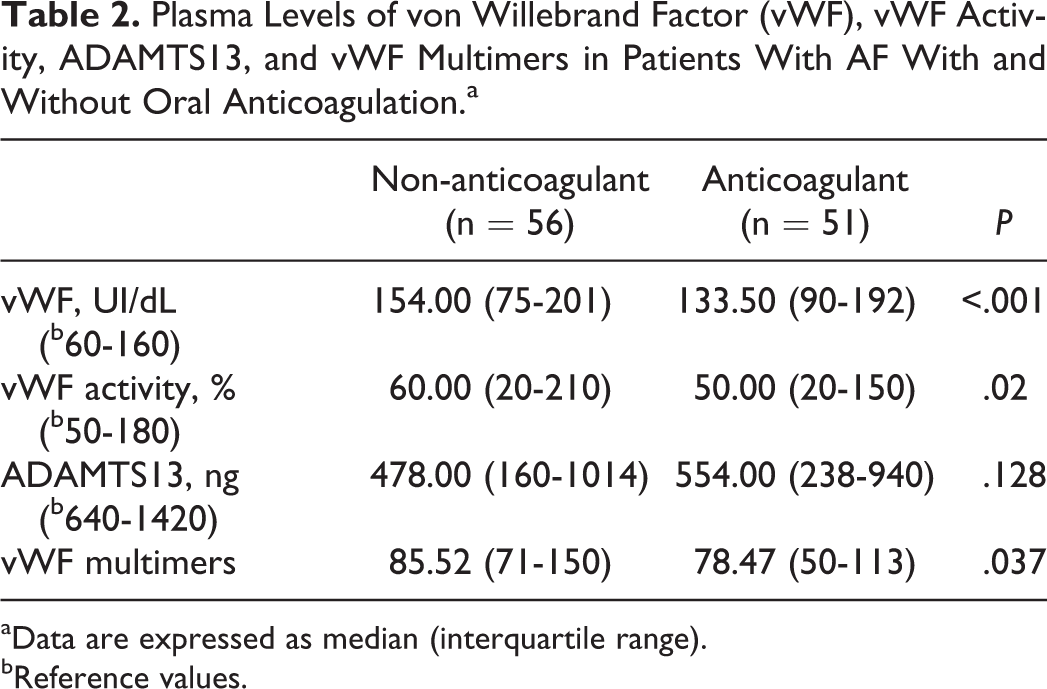
aData are expressed as median (interquartile range).
bReference values.
If we analyze the type of anticoagulant (Figure 1), vWF levels were significantly decreased in patients on acenocumarin (130.00 [90-187] UI/dL) compared with patients on rivaroxaban (139.00 [90-192] UI/dL) and patients without OAC (154.00 [75-201] UI/dL). There was a significant difference among the 3 groups (analysis of variance P = .001). The vWF concentrations and vWF activity between the acenocumarin and rivaroxaban groups did not differ significantly (130.00 [90-187] UI/dL and 139.00 [90-192] UI/dL, P = 0.310, and 50.00% [30%-160%] and 50.00% [20%-150%], P = .325, respectively). No difference was observed in vWF concentrations and vWF activity between patients on rivaroxaban and patients without OAC (139.00 [90-192] UI/dL and 154.00 [75-201] UI/dL, P = .171, and 50.00% [20%-150%] and 60.00% [20%-210%], P = .124). The vWF levels correlated positively with vWF activity (r = .781, P ≤ .001).
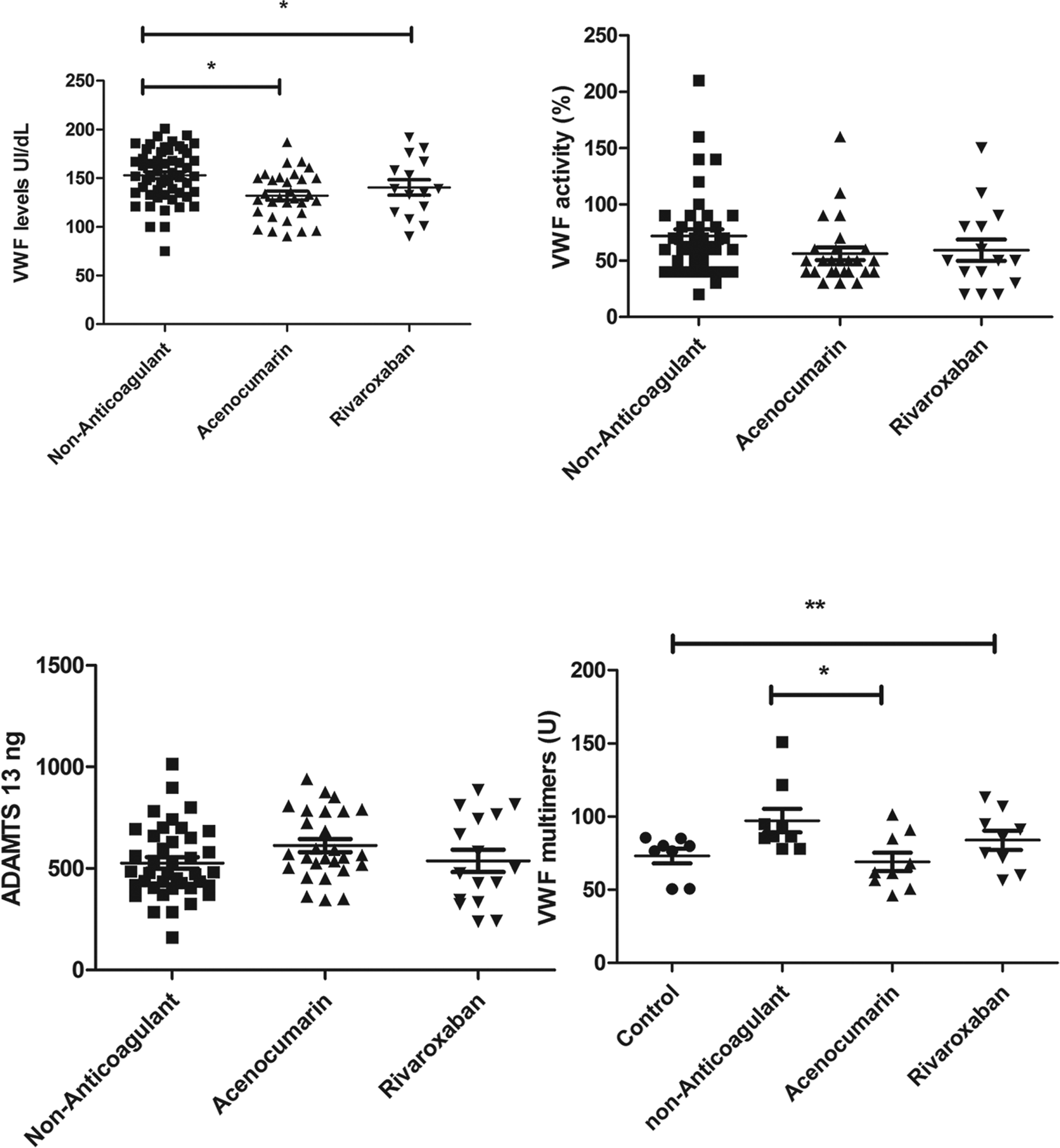
von Willebrand factor (vWF) and vWF-related parameters in atrial fibrillation with and without oral anticoagulation (OAC). Black circle: healthy controls; black squares: patients without OAC; black triangle: acenocumarin treatment; invert triangles: rivaroxaban treatment. Horizontal bars show median values. Significant differences are marked: *P ≤ .05 compared with the non-OAC group, **P ≤ .05 compared with the control group.
We investigated ABO blood group according to the studied groups, showing similar behavior in both, and we found a significant difference in vWF levels, which were decreased in O blood group patients (Table 3).
Levels of vWF in Individuals With Blood Group O and Blood Group Non-O.a
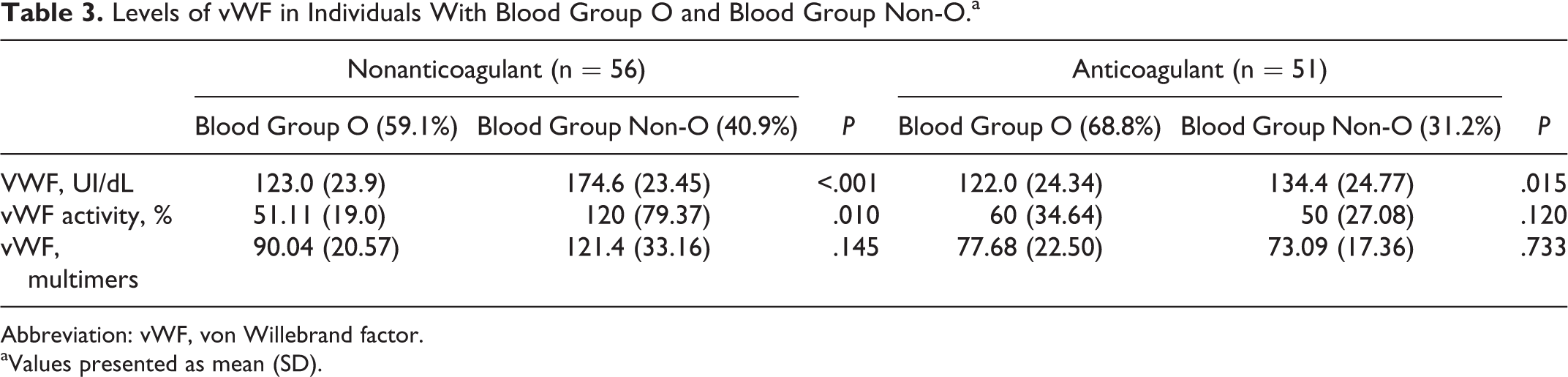
Abbreviation: vWF, von Willebrand factor.
aValues presented as mean (SD).
von Willebrand Factor Multimeric Structure
Multimers of vWF (expressed in arbitrary units of densitometric analysis) were compared in patients without anticoagulants (85.52 [71.90-150.86] U), patients on acenocumarin (64.80 [50.75-101.36] U), and patients on treatment with rivaroxaban (88.42 [56.34-113.09] U). Multimers were significantly elevated in the nonanticoagulant group (P = .009; Figure 2).
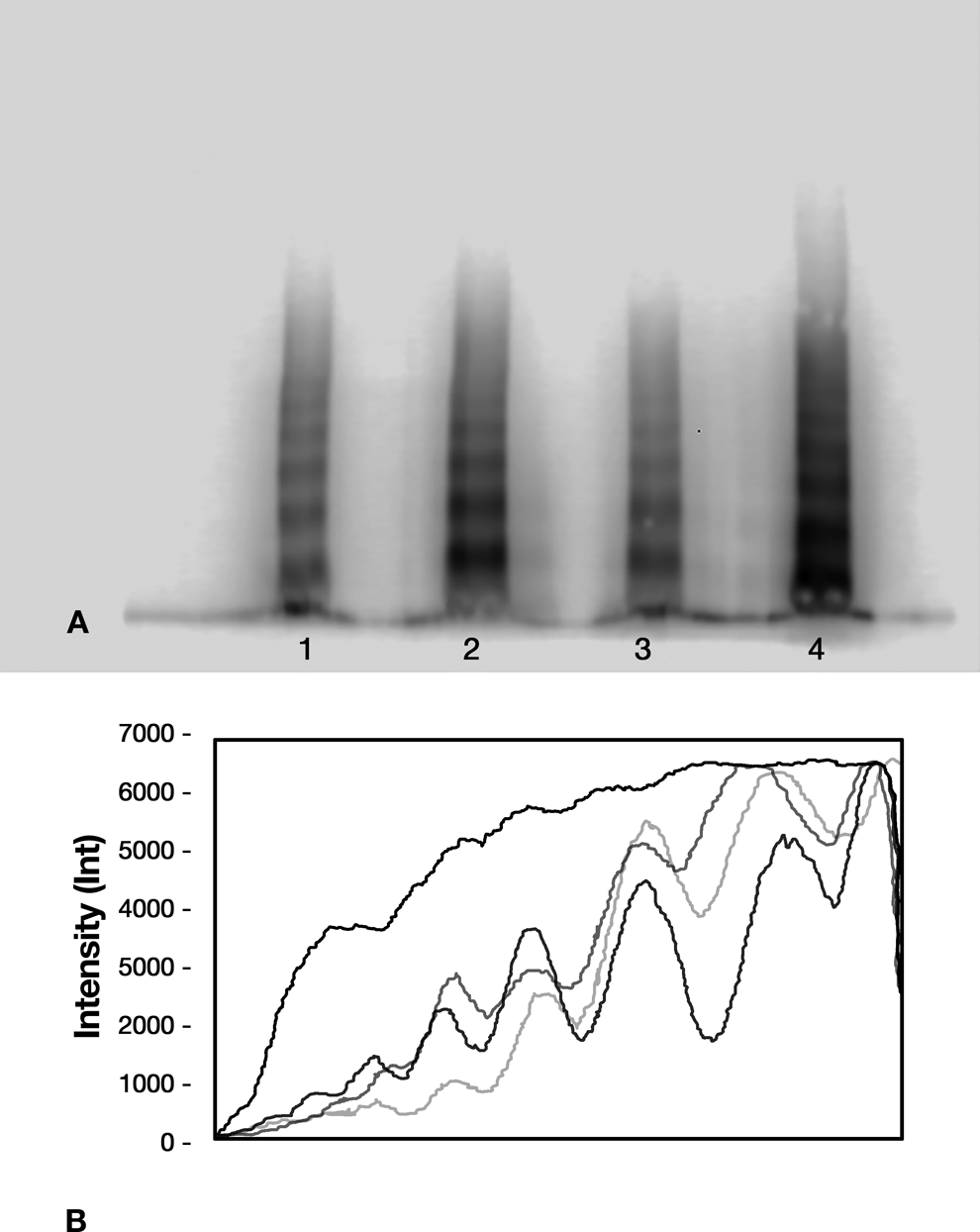
Multimeric pattern of von Willebrand factor (vWF). A, Multimerization pattern of vWF in atrial fibrillation (AF) with and without anticoagulant treatment. Sample 1, healthy control; sample 2, AF without oral anticoagulation (OAC) treatment; sample 3, AF with anticoagulant treatment; sample 4, AF with ischemic stroke. B, Densitometric analysis of vWF multimers. Upper black line: AF with stroke; lower black line: healthy control; light gray line: AF with OAC; gray line: AF without OAC.
In most patients without OAC, vWF HMWMs were increased in the multimeric pattern when compared to normal pooled plasma. The HMWMs were less detected in the multimeric pattern of patients with anticoagulant treatment. Interestingly, in patients with stroke (12.5%), a particular increase in vWF levels (168.0 [135-201] UI/dL and 132.38 [75-192] UI/dL, P = .002), vWF activity (145.00% [80-210%] and 55.38% [20%-150%], P = .003), and vWF HMWMs (128.19 [127.85-128.55] U and 83.63 [50.75-150.66] U, P = .032) was observed when compared to patients with AF without stroke.
ADAMTS13
We found lower ADAMTS13 levels in patients without OAC (478.00 [160-1014] ng) than in patients on acenocumarin (566.00 [346-940] ng) and rivaroxaban (489.00 [238-886] ng, P = .087).
ADAMTS13 correlated negatively with vWF levels (r = −.356, P = .001), vWF activity (r = .449, P ≤ .001), history of stroke (r = −.222, P = .044), acute stroke (r = −.256, P = .048), CHADS2 score (r = −.228, P = .038), and CHA2DS2-VASc score (r = −.269, P = .014) in patients with AF.
von Willebrand Factor Parameters Related to Clinical Parameters
Acute stroke correlated positively with vWF antigen (r = .389, P = .001), vWF activity (r = .392, P = .002), and vWF multimers (r = .412, P = .029). In addition, a positive correlation was found between CHA2DS2-VASc and vWF levels (r = .303, P = .002), between CHA2DS2-VASc and vWF activity (r = 0.373, P = .001), and between CHADS2 and vWF activity (r = .320, P = .003). The vWF multimers correlated positively with CHADS2 (r = .338, P = .079).
Discussion
The present study suggests that plasma concentrations of vWF, as well as vWF activity, are increased in patients with AF without OAC when compared to patients with AF with OAC. Although vWF plasma levels may seem lower than those found in other studies, this could be due to the high prevalence of O blood type in Mexican population, since vWF levels are usually lower in this blood type. Other groups have found similar results. In 1995, Gregory Lip demonstrated that plasma levels of vWF are increased in patients with chronic AF not taking antithrombotic treatment compared with controls with sinus rhythm. 21 Li-Saw-Hee et al and Jeffrey Liles et al confirmed the presence of higher levels of vWF in patients with AF compared to healthy controls. 22,23 Ammash et al demonstrated that elevated vWF:Ag may help identify patients with AF at risk of left atrial appendage thrombus. 24 Meanwhile, Roldán et al demonstrated that high plasma vWF levels are an independent risk factor for adverse events in anticoagulated patients with AF, 8 and Lind et al associated vWF factor with all-cause mortality and cardiovascular events in patients with AF. 25
Paradoxically, high levels of vWF antigen are associated with both thrombotic events and bleeding complications in patients treated with OACs. 8,26 The mechanism for the dual association is not clear, and different pathways could contribute to high levels of vWF. It is also possible that vWF could be an effector in thrombotic events, possibly by increased binding to platelets. 25 An indirect example of the importance of vWF in promoting thrombogenesis is the clinical hemorrhagic consequences of its deficiency in von Willebrand disease. 4 Likely, the mechanisms for increased vWF have not been fully elucidated in chronic diseases such as cardiovascular disease. Higher vWF plasma levels have been linked to hyperglycemia and hyperinsulinemia in diabetes, to increased hydrostatic pressure in hypertension, and to oxidized low-density lipoprotein cholesterol in hypercholesterolemia. 4,27,28 Our results showed lower vWF plasma levels in patients with OAC. Similar observations of the marked reduction in hemostatic markers with conventional anticoagulation have been reported in previous studies. 29,30 The introduction of conventional adjusted-dose warfarin (achieving an INR 2.0-3.0) seems to normalize abnormal levels of thrombogenic markers. 21,29 Plasma levels of vWF antigen are somewhat reduced by OAC treatment. 23,25 As it is well known, vWF possesses several functions in hemostasis; among them, some of the most important might be protecting factor VIII from proteolysis or cellular uptake besides binding to the surface of activated platelets and endothelial cells. 5 Thrombin cleaves vWF off of FVIII, releasing it to mediate platelet adhesion and aggregation. 31 This latter step might be impaired in patients receiving coumadin-derived oral anticoagulants.
Plasmatic levels of vWF are often regarded as a biomarker of endothelial dysfunction and atherosclerosis. 4,32 It is possible that high plasma levels of vWF antigen reflect a more severe form of endothelial dysfunction, in general, while increased active levels of vWF may reflect a decrease in its regulation due to reduced proteolysis (by ADAMTS13 or another protease) or diminished clearance by low-density lipoprotein receptor-related protein 1. 33 We found higher vWF activity in patients without OAC and a positive correlation with vWF levels. In patients with high levels of vWF activation and antigen, the incidence of cardiovascular events and mortality is especially high, indicating that these patients have an increased thrombotic risk. 25,32
An interesting finding is that patients without OAC seem to have substantially higher levels of vWF HMWMs. The larger multimeric forms of vWF are hemostatically more active, adhering better to endothelium and platelets. 4,34 This results in larger procoagulant vWF multimer concentrations and consequently a prothrombotic state that may lead to thrombus formation at sites of endothelial damage and especially at sites with a higher shear stress such as arterial circulation. 35 Further studies are needed to investigate whether the increased risk that is related to vWF antigen is in part mediated by the presence of vWF HMWMs.
ADAMTS13 antithrombotic properties are related to the cleavage of von Willebrand Factor (vWF) into smaller and less active multimers. 15 Individuals who had both lowest ADAMTS13 activity and higher vWF levels had an increased risk of ischemic stroke, suggesting that ADAMTS13 and vWF are independent risk factors for thrombotic events. 35 Patients without OAC had lower levels of ADAMTS13, and such levels correlated with higher vWF levels, higher vWF activity, stroke risk stratification scales, and the incidence of stroke. The association between ADAMTS13 and ischemic stroke has been investigated previously in small case–control studies. 10,36 –38 The association between low ADAMTS13 activity and ischemic stroke risk is likely to be explained by less cleavage of vWF HMWMs, which are the most prothrombotic. 4,35 Freynhofer et al affirm that vWF and its cleaving protease ADAMTS13 might play an important role in the development and perpetuation of vascular disease in patients with AF. 39 Sonneveld et al conclude that low ADAMTS13 activity was significantly associated with the risk of ischemic stroke, independent of age, sex, and established cardiovascular risk factors over a median of 10.7 years of follow-up, and addition of ADAMTS13 activity improved the accuracy of risk predictions for ischemic stroke beyond the traditional risk factors. 35 In other words, more risk is associated with lower ADAMTS13 levels.
From these results, an altered vWF multimeric pattern would be expected with the presence of HMWMs because lower ADAMTS13 levels correlate with increased levels of ultralarge vWF multimers.
Thrombotic risk is assessed in patients with AF by means of stroke risk stratification scales (CHADS2 or CHA2DS2-VASc) to determine whether anticoagulants should be used to prevent stroke. 40 It is not surprising that in our study we found a positive correlation between the risk stratification scale and vWF levels, vWF activity, and multimeric structure of vWF. There are studies that found significant correlations between plasma vWF levels and CHADS2 score. 7 Levels of vWF antigen were proposed to be a risk marker, when included in clinical risk scores, for thromboembolic events in patients with AF. 41 The addition of vWF plasma levels to the clinical risk stratification data has shown an independent association between high levels of vWF and the risk of a vascular event. 8,22 CHADS2 score does not include many common stroke risk factors. Given the need to be more inclusive of common stroke risk factors, many studies have confirmed the ability of CHA2DS2-VASc to identify “low-risk” patients. 40 One validation of CHA2DS2-VASc and CHADS2 in a Danish nationwide cohort of 73 538 patients with AF demonstrated that CHA2DS2-VASc performed better than CHADS2 in predicting the risk of stroke and thromboembolism. 42 We found an important correlation between CHA2DS2-VASc and vWF levels, vWF activity, and multimers of vWF.
Many studies support that vWF is not only a marker but also an important effector in the pathogenesis of cardiovascular disease. 9 Our results show that increased vWF levels, vWF activity, and modifications in the multimeric structure showing HMWMs all correlate with the incidence of stroke and could indicate a causal role of vWF. 10,25 Several studies have reported an association between high vWF levels and the risk of ischemic stroke. 11,43,44 We found increased vWF levels, vWF activity, and vWF HMWMs in patients with acute stroke . High plasma levels of vWF are regarded as a biomarker of endothelial dysfunction. 4,32 Patients with stroke were not on OAC as the diagnosis of AF was established at admission. As it is well known, OAC inhibits thrombin formation and thrombin inactivates ADAMTS13, 45 and in consequence, formation of HMWMs; larger multimeric forms of vWF are more active in hemostasis, 4,34 promoting a prothrombotic state. 35 Nevertheless, this could be due to the acute response to stroke, so further studies are needed to confirm whether vWF parameters are related to an increased risk of stroke. Low ADAMTS13 activity is associated with the risk of ischemic stroke and improves the accuracy of risk predictions for ischemic stroke beyond traditional risk factors. 35
Limitations
The limitations of the study are: Our study includes a small number of patients; nevertheless, it was sufficiently powered to show pronounced effects on the biomarkers studied; however, due to the sample size, we cannot draw firm conclusions. Anticoagulant therapy was prescribed according to clinician criteria, and patients were not assigned in a randomized manner. Finally, further investigation is required to confirm our results.
In our study, samples were frozen and stored at −80ºC for a maximum of 8 months before analysis. Previous studies have shown that such storage time does not seem to affect stability of plasma proteins. 46
Conclusions
In conclusion, our data demonstrate that vWF plasma levels, activity, and molecular structure were modified in patients with AF who were treated with OAC and who were related to stroke; the correlation with thrombotic complications adds the potential importance of vWF as a biomarker or pharmacological target. Future, larger investigations are required to confirm our hypothesis. The description of a new risk factor might thus support the development of new preventive measures and treatment strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.