
Abstract
One strategy to manage patients on warfarin starting an interacting drug is to increase the frequency of monitoring. Another strategy is to adjust warfarin dose around the time patient is started on an interacting medication, which is known as “preemptive warfarin dose adjustment.” The main objective of this study is to compare preemptive to nonpreemptive strategy and their impact on the quality of anticoagulation management. This is a retrospective cohort study performed at the pharmacist-managed anticoagulation clinic in a tertiary hospital in the State of Qatar. Over a 4-year period, 340 patients were evaluated, and 58 warfarin–drug interaction encounters were identified. Mean age of the patients was (57.7 ± 13.7), and 50% of them were females. Preemptive dose adjustment was used in 17 (29.3%) cases. Incidence of out-of-target international normalized ratio (INR) was statistically lower in the preemptive arm compared to the control group (41.2% [7/17] vs 69.2% [27/39], P = .048). Incidence of extreme out-of-target INR was numerically lower in the preemptive arm compared to the control but did not reach statistical significance (11.8% [2/17] vs 29.3% [12/41], P = .139). Change in frequency of INR monitoring was not different between the 2 groups. However, overall frequency of INR monitoring after onset/discontinuation of interacting medication increased compared to baseline (7 [9] vs 21 [16] days, P < .001). Preemptive strategy was shown in our study to decrease incidence of the out-of-target INR visits, although patients remained in need for close monitoring.
Introduction
Warfarin is the mainstay oral anticoagulant medication and one of the most widely prescribed medications all over the world. 1 Because of its narrow therapeutic index and numerous drug and food interactions, close and consistent monitoring of anticoagulation is mandated to ensure optimal outcomes and minimize the risks associated with inappropriate management. International normalized ratio (INR) is a reliable surrogate marker that has been used for decades as an indicator for warfarin therapeutic effect and its interaction with food and drugs. 2 Drugs interacting with warfarin can have different mechanisms including direct pharmacokinetic effect (induction or inhibition) on the Cytochrome P450 (CYP450) isoenzymes that are involved in the warfarin metabolism; altered absorption or protein binding (eg, cholestyramine); synergistic pharmacodynamic effect leading to increased risk of bleeding (eg, antiplatelets); eradication of vitamin K producing intestinal flora (eg, antibiotics and antifungals). In addition to drug interactions, most dietary products rich in vitamin K and those altering CYP enzyme activity can affect warfarin action. 3 Whether the warfarin interaction is drug–drug or drug–food, it may lead to serious adverse effects—where inhibition of warfarin effect can lead to treatment failure and recurrence of thromboembolic events, while potentiation of warfarin effect can lead to increased risk of bleeding that may range from minor to life-threatening bleeding and death. 4 –6 Although direct oral anticoagulants (DOACs) such as dabigatran, rivaroxaban, apixaban, edoxaban, and betrixaban offer advantages over warfarin, their use is still limited due to the increase in gastrointestinal side effects, contraindication in patients with major renal dysfunction, and lack of superiority when compared to patients with well-managed warfarin therapy. 7 –10 Lastly, the cost of DOACs compared to warfarin may be prohibitive for many patients. 11 This has led warfarin to remain as the most widely prescribed oral anticoagulant in many countries despite challenges with its management. 12 –17 Variety of models are used in warfarin management including patient self-management, specialized anticoagulation clinics, and pharmacist-managed anticoagulation clinics. 18 Pharmacist-managed anticoagulation clinic represents a model that provides patients with more consistent management, closer monitoring, more education, and awareness especially in regard to interacting drugs and food which can ultimately alter warfarin efficacy and safety. 18 –21
One strategy to manage patients on warfarin starting an interacting drug is to increase the frequency of monitoring. Another strategy is to adjust warfarin dose around the time patient is started on an interacting medication, which is known as “preemptive warfarin dose adjustment.” Most studies evaluating these strategies focused on warfarin interactions with anti-infective agents. In this study, we explore the effect of warfarin interactions with wide variety of medications on the quality of anticoagulation management in a pharmacist-managed anticoagulation clinic in Al Wakra hospital, Hamad Medical Corporation (HMC). The main objective is to compare preemptive to nonpreemptive strategy and their impact on the quality of anticoagulation management.
Aim of Study
To evaluate the different strategies used by the clinical pharmacists working in the anticoagulation clinic and to compare the incidence of supratherapeutic INR in preemptive dose adjustment group versus the control group.
Ethics Approval
The institute of research board at HMC approved the study protocol.
Methods
Design and Setting
The study design was a retrospective cohort study aiming to compare preemptive versus nonpreemptive strategies in managing drug interactions with warfarin. A retrospective chart review of all eligible patients enrolled at Al-Wakrah pharmacist-managed anticoagulation clinic was performed. All INR testing in clinic is performed with point-of-care (POC) instruments. Per clinic policy, all INR values greater than 5 obtained from POC instruments were verified with central laboratory assessment. A biweekly calibration is performed for the clinic’s POC instrument using plasma calibration sets. In addition to the clinic paper-based flow sheet, all visits are documented on electronic medical records (Cerner).
Data Collection and Study Patients
The research subjects included eligible patients managed between the period of May 2013 to May 2017. A data abstraction form was developed in order to collect patients’ data from HMC computer and paper-based database. The following information was extracted from each eligible record: (1) patient demographics and baseline characteristics including age, gender, indication for anticoagulation, duration of anticoagulation, drug interacting with warfarin, degree of interaction, and INR goal; (2) INR data at baseline (4 weeks prior) and after the onset/offset of drug interaction.
Patients were eligible for inclusion if they have been followed at the pharmacist-based anticoagulation clinic at Al-Wakrah and there was an initiation/discontinuation of a drug interacting with warfarin. Patients were excluded if they were less than 18 years of age or if they received anticoagulants other than warfarin. Anticoagulation clinical and hospital records were used for screening eligible patients.
Assessment of Outcomes
The primary outcome was to compare the impact of preemptive versus nonpreemptive strategies on the incidence of out-of-target INR (out-of-target INR was defined as INR above or below target range by ±0.2) as well as the incidence of extreme out-of-range INR values, as defined by an INR ≤1.5 or ≥4.5 (definition previously used by Schulman et al). 22
Secondary outcomes included comparison of the overall frequency of INR monitoring, incidence of out-of-target INR and extreme out-of-range INR prior and during the interaction period. Change in frequency of INR monitoring in the preemptive versus nonpreemptive strategies was also compared. We also included a subgroup analysis of the primary outcomes based on the level of drug interaction. Levels of drug interactions were identified using LexiComp definitions. LexiComp interactions module was used to analyze the interactions.
Statistical Analysis and Sample Size
Both descriptive and inferential statistical analyses were applied for the collected data using IBM Statistical Package for Social Sciences (IBM SPSS version 25 software). Categorical variables were expressed as frequencies and percentages while continuous variables were expressed either as mean ± standard deviation or median (interquartile range [IQR], for data that were not normally distributed). t test or Mann-Whitney U test (if data were not normally distributed) was used to compare continuous data. For paired continuous data, paired-t test or Wilcoxon signed rank test (if data were not normally distributed) was used. For categorical variables, either χ2 or McNemar (for paired variables) tests were used. Statistically significant results were determined at a P value of <.05. All patients who met inclusion/exclusion criteria were included in the analysis.
Results
Over the period of 4 years (2013-2017), 340 patients were evaluated and 58 warfarin–drug interaction encounters were identified. Mean age of the patients was (57.7 ± 13.7) and 50% of them were females. Atrial fibrillation/flutter stroke prevention and treatment of venous thromboembolism were the 2 main warfarin indications (43.1% and 39.7%, respectively). Majority of the patients had an INR goal of 2 to 3 (84.5%). Interacting medications and the number of patients affected by each agent are mentioned in Table 1. Initiation of an interacting drug was the main cause of interaction (84.5%) while the remaining interactions (15.5%) were due to discontinuation of an interacting drug. Most of the drug interactions were either grade C (58.6%) or grade D (39.7%). Preemptive dose adjustment was used in 17 cases (29.3%). There were no statistical differences between preemptive and control groups in any of the demographic or baseline characteristics (Table 2). A list of all interacting drugs in our cohort and their frequency are listed in Table 1.
Interacting Medications and Number of Patients Affected.

a Other medications = amiodarone, azithromycin, charcoal, celecoxib, diclofenac, digoxin, lansoprazole, ranitidine, torsemide.
Baseline Characteristics of Patients.

Abbreviations: INR, international normalized ratio; IQR, interquartile range; VTE, venous thromboembolism; SD, standard deviation.
a Baseline characteristics are presented based on number of encounters. Categorical variables were compared using χ2 or Fischer exact test, as appropriate. Age, dose, and INR were compared using independent t test and follow-up intervals were compared using Mann-Whitney U test.
As expected, the whole cohort’s overall frequency of INR monitoring after onset/discontinuation of interacting medication increased compared to baseline (7 [9] vs 21 [16] days, P < .001). Due to the effect of the interaction on INR stability, overall incidence of out-of-target INR was statistically higher after interaction compared to baseline (32 [59.3%] vs 13 [24%], P = .001]. Similarly, incidence of extreme out-of-range INR was also found to be higher after interaction compared to baseline but did not reach statistical significance (13 [23.6%] vs 6 [10.9%], P = .143; Table 3).
Effect of Drug Interactions on the INR Monitoring Frequency and Quality of Anticoagulation Management.a
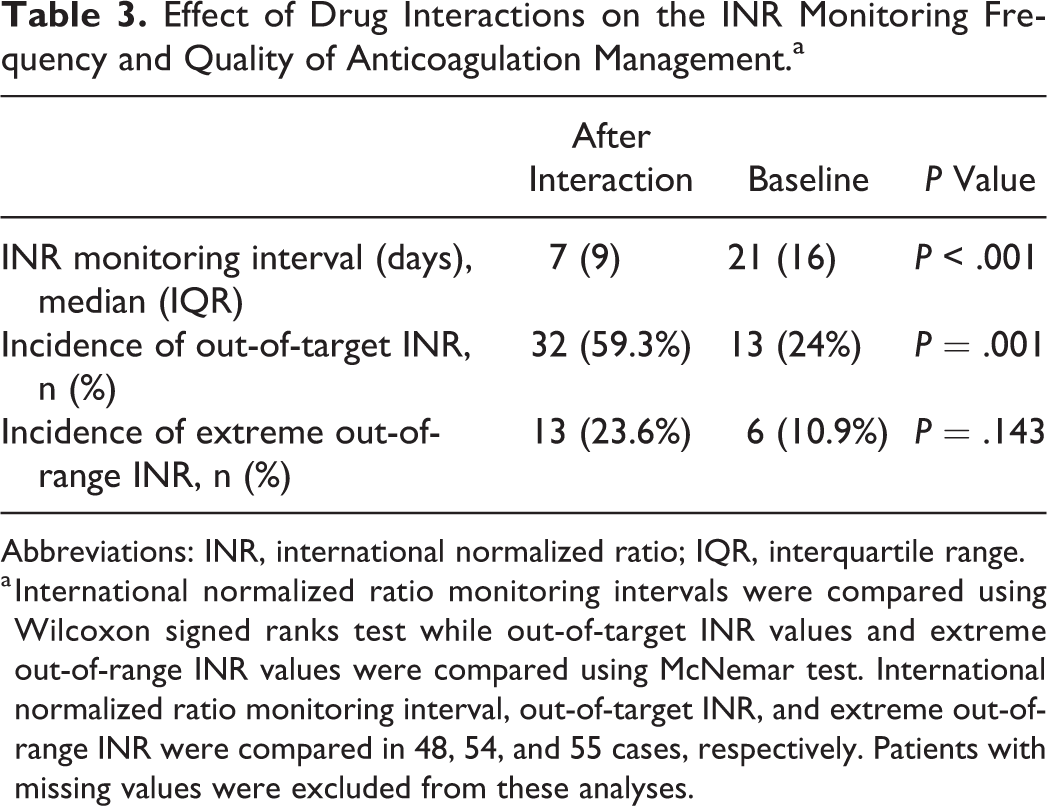
Abbreviations: INR, international normalized ratio; IQR, interquartile range.
a International normalized ratio monitoring intervals were compared using Wilcoxon signed ranks test while out-of-target INR values and extreme out-of-range INR values were compared using McNemar test. International normalized ratio monitoring interval, out-of-target INR, and extreme out-of-range INR were compared in 48, 54, and 55 cases, respectively. Patients with missing values were excluded from these analyses.
When we compared the change in the frequency of INR monitoring in the preemptive arm to the control arm, there was no statistical difference between both groups (−7.5 [27] vs −8.5 [70], P = .92; Table 4). However, incidence of out-of-target INR was statistically lower in the preemptive arm compared to the control group (41.2% [7/17] vs 69.2% [27/39], P = .048; Figure 1) indicating improved INR control with the preemptive strategy. Incidence of extreme out-of-range INR was numerically lower in the preemptive arm compared to the control but did not reach statistical significance (11.8% [2/17] vs 29.3% [12/41], P = .139).
Effect of Preemptive Dose Adjustment of Warfarin on the INR Monitoring Frequency.

Abbreviations: INR, international normalized ratio; IQR, interquartile range.
a Monitoring intervals were compared using Mann-Whitney U test.

Effect of preemptive dose adjustment strategy on the percentage of out-of-target INR values. Out-of-target INR was defined as INR above or below target range by more than 0.2. *χ2 test was used to compare the 2 strategies. INR indicates international normalized ratio.
In a subgroup analysis in patients with grade C interactions, the incidence of out-of-target INR (more than 0.2 from target) was significantly lower in preemptive dose adjustment group compared to the control group (22.2% [2/9] vs 75% [18/24], P value = .009). Moreover, patients with grade D interactions had numerically lower incidence of out-of-target INR in preemptive dose adjustment compared to control group but it did not reach statistical significance as shown in Table 5. Another subgroup analysis of extreme out of range INR (1.5 ≤ or ≥ 4.5) in preemptive dose adjustment group compared to the control group stratified by the grade of drug interaction with warfarin showed a lower incidence in patients with preemptive dose adjustment compared to control group in drug but it did not reach statistical significance as shown in Table 5.
Subgroup Analyses of Preemptive Dose Adjustment Compared to Control Group Comparisons Based on Degree of Interaction.

Abbreviations: INR, international normalized ratio; IQR, interquartile range.
Discussion
In this research work, we observed an improved INR control with the preemptive strategy that was evidenced by the decreased incidence of the out-of-target INR visits. Extreme out-of-range INR was also numerically lower compared to the nonpreemptive strategy but did not reach statistical significance. Benefit of the use of preemptive warfarin dose adjustment has been studied by others, however, results were conflicting. 23 –27 Three of these studies were retrospective observational studies that focused on preemptive dose reduction of warfarin in patients initiating metronidazole, 23,25 sulfamethoxazole-trimethoprim, 23,24 and levofloxacin. 24 While 2 other studies were randomized controlled trials (RCTs) by Dowd and colleagues and they compared preemptive warfarin dose reduction to reactive warfarin dose adjustment in patients receiving prednisone 26 and in patients receiving doxycycline. 27 The 3 observational studies indicated that patients with preemptive strategy were more likely to maintain therapeutic INR and not to have supratherapeutic INR compared to the control group. These results were more pronounced in patients on metronidazole and sulfamethoxazole-trimethoprim than in patients on levofloxacin.23–25 On the other hand, both RCTs on warfarin–prednisone and warfarin–doxycycline interactions, found more control patients with INR of more than 1 point over the goal upper limit compared to the intervention group but these results did not reach statistical significance. 26,27 There was also a statistical significance increase in the incidence of subtherapeutic INRs in the preemptive group. Controversy in these studies’ results is likely justified by the differences in the study design, extent of dose reduction made in the preemptive arm, measured outcomes, and the studied drug interaction. For example, medications such as sulfamethoxazole-trimethoprim and metronidazole are well known to have higher level of interaction with warfarin and to induce more consistent elevation in INR. 28,29 This justifies the positive impact of preemptive strategy seen in the research work studying the warfarin interaction with these drugs. In our study, all different medications interacting with warfarin were included. About 20% of these observed interactions, however, were with metronidazole and sulfamethoxazole-trimethoprim (Table 1).
Based on our subgroup analysis that stratified interacting medications according to degree of interaction, a significantly lower out of range INR was seen in preemptive dose adjustment versus control in category C interaction. This was the only statistically significant result in this subgroup analysis. Other results showed some trend of less extreme out of range INR in the preemptive dose adjustment group although these results were not statistically significant (Table 5).
Our study also indicates that warfarin drug interactions increase the need for frequent INR visits due to instability in the INR. However, there was still an increased incidence in the out-of-range INR visits postinteraction compared to baseline. This result is in alignment with previous report by Raebel et al where warfarin monitoring in patients receiving antimicrobial therapy was evaluated. 30 The study found that 77% of the patients were seen within 14 days of the initiation of the interacting medication.
Our study must be taken in context of several limitations. First, the study was observational in nature and may have been exposed to selection bias that could impact its internal validity. Additionally, our study sample may have been inadequate since it was not powered. Instead, we relied on capturing all drug interactions that occurred at the clinic since it was launched. Further, percentage dose reduction or increase was not always consistent since it was a clinical decision based on the interacting medication and the patient condition and was left at the discretion of the pharmacist running the clinic.
Despite these limitations, our study is considered unique since it is one of few studies that looked at wide variety of medications interacting with warfarin and was not specific to 1 or 2 medications. There was also a limited attrition and information bias since we had good record of patients’ INR at baseline and after the interaction.
Conclusion
Drug interactions with warfarin are associated with impaired INR control that requires more frequent follow-up visits to adjust warfarin dose. Preemptive strategy is shown in our study to decrease incidence of the out-of-target INR visits, although patients remained in need for close monitoring. Future randomized prospective studies are warranted to confirm these findings.
Footnotes
Authors’ Note
This work has been presented at ACCP Fall meeting in 2017: Fahmi A, Mohamed A, Elewa H, and Saad M. Management of warfarin drug interactions in a pharmacist managed anticoagulation clinic: evaluation of frequency of INR monitoring and preemptive dose adjustment. ACCP fall conference, October 7-10, 2017, Phoenix, Arizona.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Medical Research Center, Hamad Medical Corporation. RP#17226/17.