
Abstract
Cancer-associated thrombosis (CAT) studies have increased in recent years and the quality of guidelines to guide the clinical practice of CAT prevention and treatment becomes crucial. The therapy status of new oral anticoagulants (NOACs) has been established in some thrombotic diseases, but the evidence for CAT remains unconvincing. The aim of this research is to evaluate the quality of CAT guidelines and discuss the role of NOAC in CAT. A search of articles was performed using PubMed/Medline, Chinese National Knowledge Infrastructure, and other authoritative websites. Search terms included guideline or guidance, consensuses, cancer, and thrombosis. Appraisal of Guidelines for Research & Evaluation II (AGREE II) tool was used to evaluate the qualities of the guidelines. A total of 19 guidelines were screened out and evaluated, of which 8 were recommended, 5 were recommended after revision, and 6 were not recommended. For prevention and treatment of CAT, low-molecular-weight heparin is the most recommended, followed by vitamin K antagonist, unfractionated heparin, fondaparinux, and aspirin. New oral anticoagulant is optional in some cases of CAT treatment. Based on AGREE II assessment tool, the quality of CAT guidelines is inconsistent. Attention should be drawn to the quality of CAT guidelines during clinical practice. The role of NOAC in the treatment of CAT is gradually established but requires more supporting evidence from future clinical trials.
Introduction
Cardiovascular disease and cancer are the leading causes of death worldwide. Venous thromboembolism (VTE) is the third cause of mortality in cardiovascular disease in Western countries, accounting for 5% to 10% of the deaths of hospitalized patients after ischemic heart disease and stroke. 1 The relationship between cancer and VTE has been established. As early as 1823, Jean-Baptiste Bouillaud, a French physician, firstly described the association between cancer and thrombosis. 2 It is estimated that about 15% of patients with cancer have symptomatic VTE, while 15% to 20% of patients with VTE are patients with cancer, and approximately 10% of patients with unexplained VTE are diagnosed as tumors within 1 to 2 years. 3 The incidence of VTE in the general population is 1/1000 to 2/1000 person-years, 4 while the incidence of VTE in patients with cancer has been increasing every year, as high as 13.9/1000 person-years. 5 Among first-episode patients with VTE, patients with cancer account for 20% to 30%, 6 and only up to 20% of patients with cancer are diagnosed with VTE before death, while up to 50% of patients with cancer are found with VTE at autopsy. This result suggests that the morbidity of VTE may be underestimated. 7 Cancer is an independent risk factor for VTE, which occurs between 1% and 11% depending on the type of tumor. 8 Meanwhile, VTE is also an independent risk factor for bleeding and death in patients with cancer. 7 In fact, VTE is one of the leading causes of death in both outpatient and inpatient patients with cancer. 9 After the first episode, the recurrence rate of VTE in patients with anticoagulant therapy is 3.2 times higher than that of noncancer patients (20.7% per year, vs 6.8%), and the incidence of major bleeding is 2.2 times (12.4% per year vs 4.9%). 10 In addition, the medical cost of patients with cancer with VTE is approximately 2 times higher than that of non-VTE patients with cancer. 11,12
Given the increasing awareness of cancer-associated thrombosis (CAT)-related studies in recent years, it is imperative to evaluate the quality of relevant guidelines to help improve clinical practice for CAT prevention and treatment. However, many issues are yet to be studied and explored despite some existing knowledge of CAT, such as a hypothesis of mechanism and risk factors. One of these issues is the role of new oral anticoagulants (NOACs) in CAT. New oral anticoagulants are also called direct oral anticoagulants in some guidelines. New oral anticoagulant includes direct thrombin inhibitor (dabigatran) and factor Xa inhibitors (rivaroxaban, apixaban, and edoxaban) and has been established positions in the guidelines for prevention and treatment of atrial fibrillation, 13 pulmonary embolism (PE), 14 VTE after major orthopedic surgery, 15 and so on. In recent years, there have been multiple published guidelines for the prevention and treatment of CAT, so the status of NOAC for CAT needs to be understood and evaluated. In this article, we focus on the quality assessment of the guidelines for CAT with Appraisal of Guidelines for Research & Evaluation II (AGREE II) and the current status of NOAC in CAT.
Methods
A comprehensive literature search (LS) was carried out in PubMed/Medline, Chinese National Knowledge Infrastructure, and other authoritative organization official website using the keywords “cancer-associated thrombosis, guideline, guidance, or consensuses”. The specific search strategies, selection criteria, and a flow diagram are shown in Additional File 1 as a supplement. Two review authors independently screened the results. The most recent version of the guideline was included.
Appraisal of Guidelines for Research & Evaluation II, 16 a new international tool for quality assessment of guidelines, was utilized to appraise the quality of the selected guidelines. Six domains with 23 items (shown in Figure 1) were scored, including: scope and purpose (domain 1), stakeholder involvement (domain 2), rigor of development (domain 3), clarity of presentation (domain 4), applicability (domain 5), and editorial independence (domain 6). Based on the scores of the 6 domains, overall assessment was obtained to assess the quality of the guidelines.
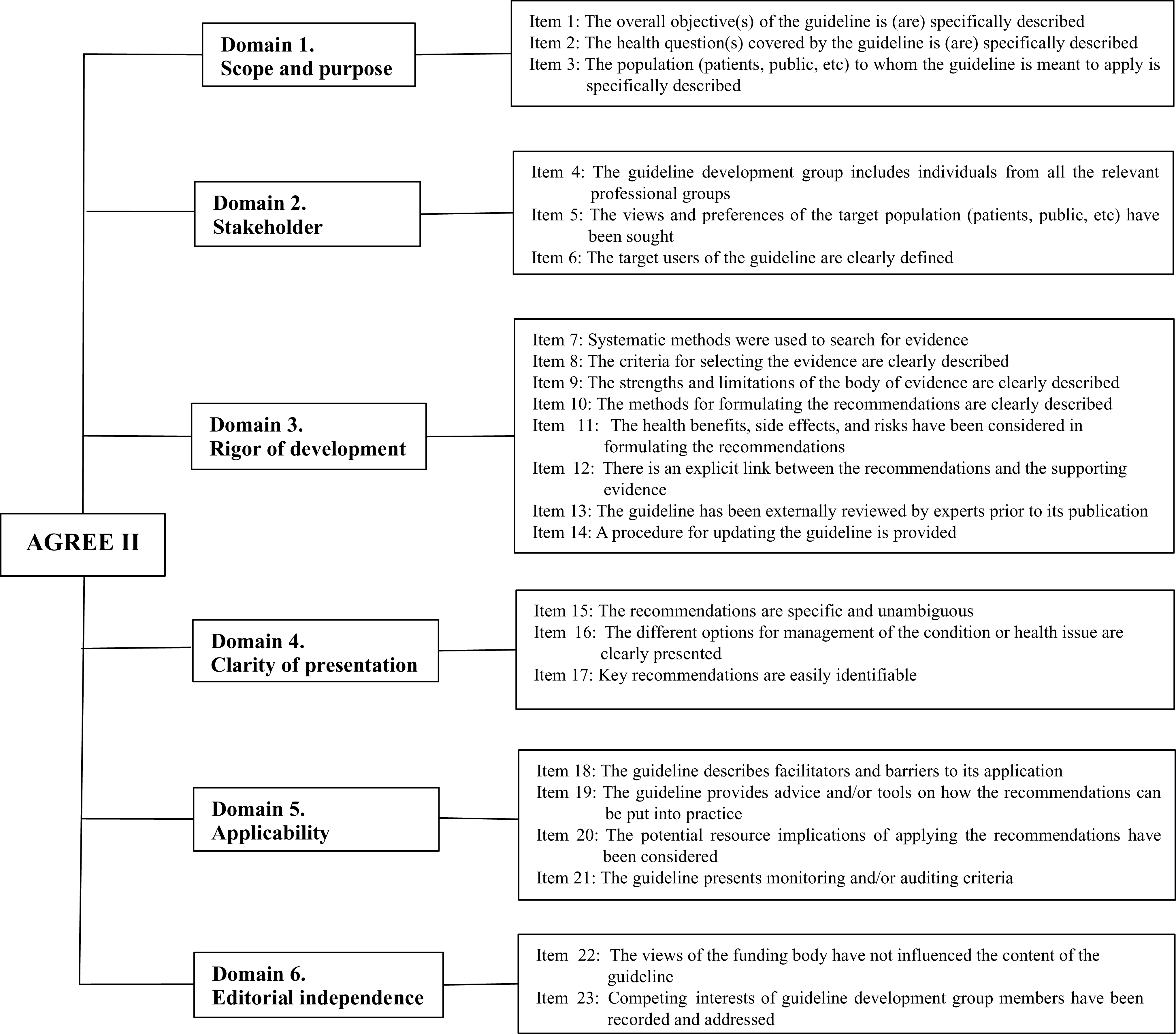
Six domains and 23 items which are scored by AGREE II. AGREE II indicates Appraisal of Guidelines for Research & Evaluation II.
Guideline evaluation was conducted by having 2 independent teams of 3 use AGREE II to score relevant guidelines followed by official training modules. The consistency among the 3 appraisers was tested using intraclass correlation coefficient (ICC): ICC ≥0.75 indicates good agreement, and ICC <0.4 indicates poor consistency. 17 Based on the guidelines, recommendations for anticoagulants and status of NOAC for VTE prevention and treatment in the different groups of patient with CAT were summarized.
Results
Quality Evaluation of the Guidelines
A total of 19 related guidelines were retrieved, ranked by years of publication as listed in Table 1. Most languages were in English (17/19), except 1 in Chinese and 1 in Spanish.
List of the 19 Guidelines for CAT.

Abbreviations: Asp, asprin; CAT, cancer-associated thrombosis; Fx, fondaparinux; ISTH, International Society on Thrombosis and Haemostasis; LMWH, low molecular weight heparin; LS, literature search; NOAC, new oral anticoagulant; SEOM, Spanish Society of Medical Oncology; SR, systemic review; SSC; Scientific and Standardization Committee; UFH, unfractionated heparin; VKA, vitamin K antagonist.
Six domains of the 19 guidelines were evaluated using the AGREE II tool, with scores were listed in Table 2. High-quality guidelines were categorized to have a threshold score of over 70%. 16 The scores of overall assessment for the 19 guidelines were among 3 to 6 point (the maximum score was 7 points). Among them, 8 guidelines (5 or 6 points) were recommended, 5 guidelines (4 points) were recommended after revised, while 6 guidelines (3 points) were not recommended.
Domain Scores and Recommendations for the 19 Guidelines Using AGREE II Tool.

Abbreviations: AGREE II, Appraisal of Guidelines for Research & Evaluation II; ICC, intraclass correlation coefficient; N, no; Y, yes; Y-M, yes, with modification.
The scores of 6 domains for the 19 guidelines are shown in Figure 2, with each domain’s score distribution and variance. Domain 2 (stakeholder involvement) and domain 5 (applicability) were of lower quality with the scores of 45% (19%; mean [standard deviation, SD]) and 52% (16%), respectively. The coefficient of variation (CV) of each domain in descending order was domain 6 (45.70%) > domain 2 (42.37%) > domain 5 (30.91%) > domain 3 (30.72%) > domain 1 (19.16%) > domain 4 (6.50%).

Score distribution of the 6 domains among the 19 guidelines.
Intraclass correlation coefficient was used to measure the consistency when performing a quality appraisal of the guidelines among the 3 appraisers, and our results are shown in Table 2. All the ICC are >0.75, indicating that the agreement was consistent with each other.
Venous Thromboembolism Prevention and Treatment in Patients With Cancer and Status of NOAC in CAT
Below is a summary of anticoagulant suggestions for VTE prevention and treatment in different types of patients with cancer followed by the 19 guidelines (shown in Table 3).
Anticoagulant Recommendations for VTE Prevention and Treatment in Patients With Cancer.

Abbreviations: Asp, asprin; Fx, fondaparinux; LMWH, low-molecular-weight heparin; NOACs, new oral anticoagulants; PE, pulmonary embolism; UFH, unfractionated heparin; VKA, vitamin K antagonist; VTE, venous thromboembolism.
Venous thromboembolism prevention in cancer outpatients
Most cancer outpatients do not require routine prevention (2B). 21,23,27,28 It may be suitable for preventing for the following types of particularly high-risk VTE conditions: multiple myeloma with thalidomide or lenalidomide regimens, 23,27,28 high Khorana scores, 23,37 some with a prior history of VTE. 23
The duration of the prophylaxis and the indications for discontinuation were unknown; low-molecular-weight heparin (LMWH) was recommended (2B). 25 New oral anticoagulant was not compared with LMWH in an outpatient setting.
Venous thromboembolism prevention in hospitalized (illness) patients with cancer
Venous thromboembolism prevention is recommended when there is no contraindication in hospitalized patients with limited activity (1B). 31 Patients without limited activity, if not contraindicated, may also benefit from prevention (2B). 31 Patients who receive systemic chemotherapy do not need routine prevention. 33 However, for locally advanced or metastatic pancreatic cancer and locally advanced or metastatic lung cancer, thalidomide and renatamide (prophylaxis with LMWH, vitamin K antagonist [VKA], or aspirin) are recommended (2C). 33 Routine prophylaxis is not recommended for patients admitted to hospital with short-term chemotherapy infusion or small procedure. 24,35 Low-molecular-weight heparin is recommended (1B), although it is unclear which one is superior among LMWH, fondaparinux, and unfractionated heparin (UFH) from current studies. 31 New oral anticoagulant was not compared with LMWH in this setting, either.
Venous thromboembolism prevention in hospitalized (surgical) patients with cancer
Prevention is recommended in most surgical patients with cancer, but not required for those with smaller operations. 34 The prophylaxis was 12 to 2 hours before operation or 6 to 12 hours after the operation, usually lasting for 7 to 10 days (1A). 28,33 The duration of prevention of extensive abdominal and pelvic surgery is 4 weeks (1B). 19,28,31 The use of LMWH, fondaparinux, and UFH depends on the patient’s characteristics. There are no NOAC trials for this type of patients.
Venous thromboembolism (PE) treatment in patients with cancer
Initial treatment (5 to 10 days)
Low-molecular-weight heparin is preferred (1A). 25,28,29 Unfractionated heparin or fondaparinux can also be used (2D). 33 If LMWH cannot be used, NOAC can be considered. 26,27,36
Long-term treatment (3 to 6 months)
Low-molecular-weight heparin is preferred over VKA (1A). 18,33 If LMWH is not applicable, NOAC is an acceptable alternative, which lasts for at least 3 months. 36 Although 6 months is recommended from 2 large trials, the evidence level is low. Compared with VKA, the survival rate of patients with cancer using LMWH remains the same. However, recurrence-risk decreases during the treatment of VTE, and the risk of massive hemorrhage does not increase. 25,29 In contrast with VKA, the risk of recurrence of VTE in patients with cancer used NOAC is lower, whereas that of massive hemorrhage does not increase. 33 There is no data to show that LMWH is directly compared with NOAC in the safety and effectiveness when the guidelines are issued. Some trials are underway and may yield results in the near future.
Extended-term therapy (> 3 to 6 months)
Venous thromboembolism (PE) treatment depends on whether the tumor is active, progressive, metastatic, under treatment, or cure. 33 The risk of recurrence and bleeding in VTE should be weighted. Tumor types, costs, survival expectations, treatment options, and patient willingness might be considered. The research in this filed is paucity. The recurrence risk assessment scale (Ottawa Score) 38,39 has to be verified.
Discussions
A total of 19 guidelines for the prevention and treatment of CAT were screened out and evaluated. Appraisal of Guidelines for Research & Evaluation II tool was used to evaluate the quality of the guidelines, and the higher score indicates better quality. The evaluation showed inconsistent quality results among the 19 guidelines, with scores of 3 to 6 points (the maximum score was 7 points). This result indicates that the quality of these guidelines needs to be further improved. Among the 6 domains, domain 2 (stakeholder involvement) and domain 5 (applicability) were of lower quality with the scores of 45% (19%) and 52% (16%), respectively. This suggests that the extent of developers, intended users, and their views was not described or considered sufficiently in the process of the guideline development. Meanwhile, facilitators and barriers, tools, and resources for application were also presented or provided insufficiently. Domain 4 (clarity of presentation) with the scores of 86% (6%) and the CV of 6.50% indicates that clarity of presentation of all guidelines is the most assuring, while domain 2 (stakeholder involvement) is the least guaranteed.
In summary, different anticoagulants are recommended in cancer outpatients, hospitalized (illness) patients with cancer, and hospitalized (surgical) patients with cancer. As shown in Table 1, LMWH is recommended in all the 19 guidelines, 15 of which were based on systematic reviews (SRs) and the other 4 on LSs. Vitamin K antagonist is recommended in 16 guidelines, 12 of which were based on SRs and the other 4 on LSs. The other 3 anticoagulants of UFH, fondaparinux, and aspirin are also recommended, but their recommendation levels are lower than LMWH and VKA. As to NOAC, only 5 guidelines recommend them, and the evidence sources are LSs. Therefore, LMWH and VKA are still the most recommended anticoagulants for prevention and treatment of CAT overall.
The development of guidelines is generally based on evidence-based medicine. Relative CAT trials with anticoagulants are summarized and listed in Table 4. CLOT trial (2003) and Long-term Innovations in TreatmEnt program (LITE) trial (2006) earn a place of LMWH over in the treatment of VTE in patients with cancer. The subgroup analysis of randomized controlled trial has proved that NOAC is superior to warfarin. Although the evidence on the direct comparison of NOAC with LMWH is lacking, the results of Hokusai-VTE (2017.12) and the first phase of SELECT-D trial suggest that NOAC is not less effective than LMWH. The incidence of major bleeding in the NOAC group was higher than that of LMWHs group, but there was no significant differences between the 2 groups. SELCET-D trial displays significantly higher clinically relevant nonmajor bleeding in NOAC group (6/203, 3% vs 25/203, 12%). The patient’s own bleeding risk factors should also be considered in the selection of NOAC. Future trials will provide more evidence to elucidate the role of NOAC in the treatment of CAT. In addition, because of the particularity of the patients enrolled in the studies, the significance of the POOL study remains to be discussed. Studies on extended-term treatment of VTE, especially longer than 6 months and the regimen of VTE recurrence are scanty. There is a shortage in study on NOAC in cancer-related thromboprophylaxis and catheter-associated thrombosis in patients with cancer. These areas above are some directions for future research.
Trials of Anticoagulants in CAT.

Abbreviations: CAT, cancer-associated thrombosis; DVT, deep vein thrombosis; LMWH, low-molecular-weight heparin; NOACs, new oral anticoagulants; PE, pulmonary embolism; RCTs, randomized controlled trials; VTE, venous thromboembolism.
aMain results of first phase of the study.
Conclusion
Based on the assessment by AGREE II, the qualities of the 19 CAT guidelines were varied, 8 of which (guideline 2, 3, 10, 11, 14, 15, 16, 19) were recommended, while others recommended after revised, or not recommended. Special attention should be paid to domain 2 and 5 (lower scores) and domain 6 (largest variations) when developing or revising CAT guidelines. For prevention and treatment of CAT, LMWH is the most recommended, followed by VKA, UFH, fondaparinux, and aspirin. The role of NOAC (dabigatran, rivaroxaban, apixaban, edoxaban) in the treatment of CAT is gradually established, but more supporting evidence is needed from the current and future clinical trials.
Supplemental Material
Supplemental Material, Additional_File_1 - Quality Appraisal of Guidelines on Cancer-Associated Thrombosis Using AGREE II Instrument and Analysis of Current Status of New Oral Anticoagulants
Supplemental Material, Additional_File_1 for Quality Appraisal of Guidelines on Cancer-Associated Thrombosis Using AGREE II Instrument and Analysis of Current Status of New Oral Anticoagulants by Jiuxing Zhang, Juan Xu, Wenlong Zhang, Meiting Jiang, Juan Liu, Lei Xu, Gaofeng Liu and Zhigang Zhao in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Authors’ Note
The study was performed according to the Helsinki convention and its ethical standards. This article does not contain any study with human participants performed by any of the authors. Jiuxing Zhang and Juan Xu contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the China Health Promotion Foundation [grant number: Huizi (2016) No. 99].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.