
Abstract
Heparin (H) anticoagulation in populations characterized by elevated platelet factor 4 (PF4) frequently elicits PF4/H antibodies, presenting a risk of heparin-induced thrombocytopenia. Recent studies have shown that anti-PF4/H enzyme-linked immunosorbent assays (ELISAs) detect antibodies in individuals never exposed to heparin. Platelet factor 4/H cross-reactive antibodies may result from PF4-mediated defense responses to injury or infection. This study questioned whether patients with diabetes are more likely to develop the endogenous cross-reactive antibodies. A comparison of healthy volunteers versus hospitalized patients with or without diabetes showed no significant differences in the prevalence of PF4/H ELISA-positive results. However, the group of patients who had both diabetes and an infectious condition had higher median antibody titer compared to other patients with or without diabetes regardless of reason for hospitalization. Higher PF4/H titers were also associated with patients with diabetes who were not on any medical therapy. In the future, determining whether PF4/H cross-reactive antibodies sensitize patients to respond adversely to heparin anticoagulation or predispose patients to other complications may be relevant to diabetes care.
Introduction
Commercial enzyme-linked immunosorbent assays (ELISAs) to detect antibodies to Platelet Factor 4/Heparin (PF4/H) complexes have been developed to aid in the diagnosis of heparin-induced thrombocytopenia (HIT). 1,2 Heparin-induced thrombocytopenia is a drop in platelet count that can occur 5 to 10 days following heparin anticoagulation and presents a high risk of potentially catastrophic thromboses. 3 Although, only 0.2% to 5% of heparin-treated patients develop clinical HIT, PF4/H antibodies can be detected in up to 50% of patients after exposure to heparin. 4 The frequency of seroconversion and of clinical HIT varies widely among patient populations. The risk of HIT is highest in conditions of elevated PF4, such as orthopedic surgery, cardiopulmonary bypass, and severe trauma. 4,5 A positive PF4/H ELISA result, that is, an optical density (OD) above a specified cut-off, helps to confirm the suspected diagnosis of HIT in heparin-exposed patients with a specific platelet count profile. 6
Currently, independent of HIT diagnosis, PF4/H ELISA OD values are also being utilized in research concerning the incidence and potential relevance of these PF4/H cross-reactive antibodies. Such studies have discovered naturally occurring cross-reactive antibodies, though typically low in titer, in healthy individuals and patients not exposed to heparin. 7,8 However in some instances, high-titer platelet-activating anti-PF4/H antibodies are found in heparin-naïve individuals who experience a spontaneous clinical syndrome consistent with HIT. 9 -12
Cases of spontaneous PF4/H seropositivity are typically preceded by an infectious, inflammatory, or surgical event. 13,14 Antibodies isolated from HIT patients cross-react with PF4 associated with activated endothelial cells, 15,16 microbial pathogens, 17 or with constituents of inflamed or damaged tissue. 18 -21 There is concern that a primary immune response to PF4 bound to endogenous structures could sensitize an individual to respond to subsequent PF4/H exposure. 13,22,23 Diabetes is associated with platelet hyperactivity, elevated PF4, and vascular compromise 24,25 which together may present an immunogenic, PF4 target conformation. To explore the possible relationship between diabetes and the presence of PF4/H sensitizing antibodies, we used the HIT ELISA to compare cross-reactive antibody OD values of hospitalized patients with and without diabetes and healthy volunteer controls.
Materials and Methods
Subjects between 18 and 80 years of age, nonpregnant and not currently on heparin who were admitted to Loyola University Medical Center Hospital in Maywood, Illinois were recruited from January 1, 2010, through February 28, 2012. Fifty patients with diabetes and 51 patients without diabetes consented to participate in the study. The study had the approval of the Loyola Institutional Review Board for the Protection of Human Subjects.
Blood specimens from patients were centrifuged and sera and plasma were stored at −70°C until testing by ELISA. Specimens from 50 healthy volunteers were available from a previous study. 26 Blood from each subject was studied in the LIFECODES PF4 Enhanced ELISA (Immucor GTI Diagnostics Inc, Waukesha, Wisconsin) which is used for detection of antibodies related to HIT. Optical density readings were used as a measure of PF4/Heparin antibody cross-reactivity. The inflammatory cytokines, IL-6, IL-8, TNF α, and CD40L were measured by ELISAs from eBioscience, Inc (San Diego, California). All ELISAs were conducted according to manufacturer’s instructions.
Statistical Analysis
Data were graphed and analyzed using Sigma Plot software (version 9.0, SYSTAT Software, Inc). Categorical characteristics of patients with and without diabetes were compared by Z-test and continuous variables were compared by t test. The distribution of PF4/H cross-reactive antibody OD values in the hospitalized patients with and without diabetes and the healthy volunteers and in subsets of the hospitalized patient groups were compared using the Kruskal-Wallis One Way Analysis of Variance on Ranks followed by Dunn’s Multiple Comparisons Test. Levels of cytokines were analyzed by the Mann-Whitney Rank Sum Test and the relationship among cytokine levels in each study group was evaluated using Spearman Correlation analysis.
Results
Clinical and Laboratory Data
Table 1 summarizes the clinical and laboratory data collected from interviews and the electronic medical record for hospitalized patients and demonstrates substantial differences between the nondiabetic and diabetic groups. Collectively, diabetics had significantly higher body mass index and were more likely to have hypertension or a history of cardiovascular disease. Not surprisingly, patients with diabetes took one or more medications compared to the nondiabetic group.
Clinical and Laboratory Information.
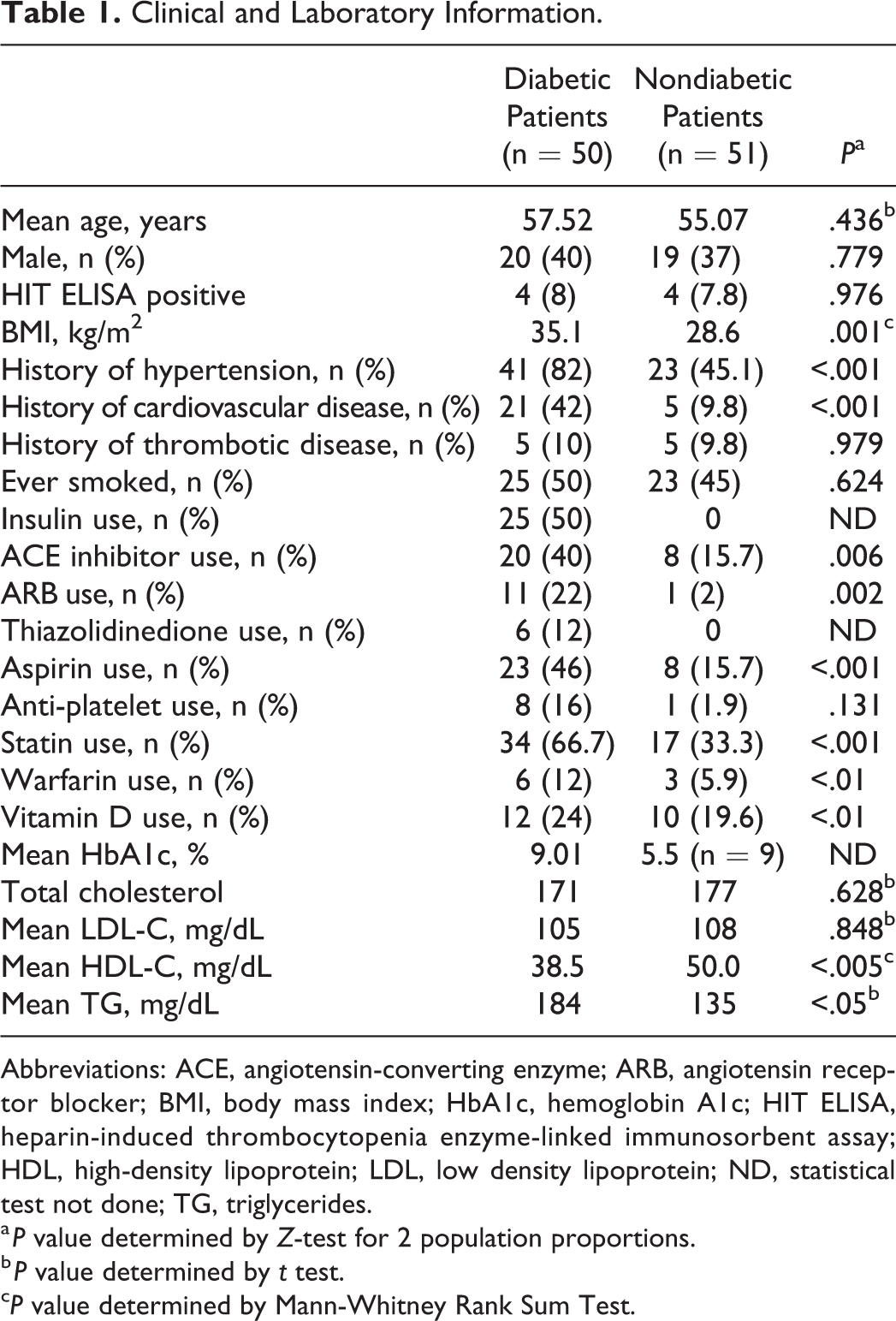
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BMI, body mass index; HbA1c, hemoglobin A1c; HIT ELISA, heparin-induced thrombocytopenia enzyme-linked immunosorbent assay; HDL, high-density lipoprotein; LDL, low density lipoprotein; ND, statistical test not done; TG, triglycerides.
a P value determined by Z-test for 2 population proportions.
b P value determined by t test.
cP value determined by Mann-Whitney Rank Sum Test.
Heparin-Induced Thrombocytopenia Antibody ELISA Titer (OD)
Three of 50 (6%) healthy individuals in the control group had a positive PF4/H antibody ELISA result based on the manufacturer’s cut-off OD value of 0.400. This is similar to 6.6% frequency of HIT positives reported in a population of 4000 normal blood donors. 7 Both the diabetic and nondiabetic hospitalized patient groups had 4 ELISA positive individuals. This rate (8%) of HIT ELISA positives among patients with diabetes is similar to that reported previously (8.8%). 27 However, the prevalence of positive responses among the diabetic group was not significantly different from that in the nondiabetic group (7.8%; Table I) nor from the healthy, control population.
In addition to determining the number of individuals with results above the minimum HIT diagnostic OD cutoff, we compared the distribution of PF4/H antibody ODs in each population as an indication of the possible presence of PF4/H cross-reactive antibodies not related to heparin exposure. We found no significant differences in median antibody titer among the 3 study populations (Figure 1).
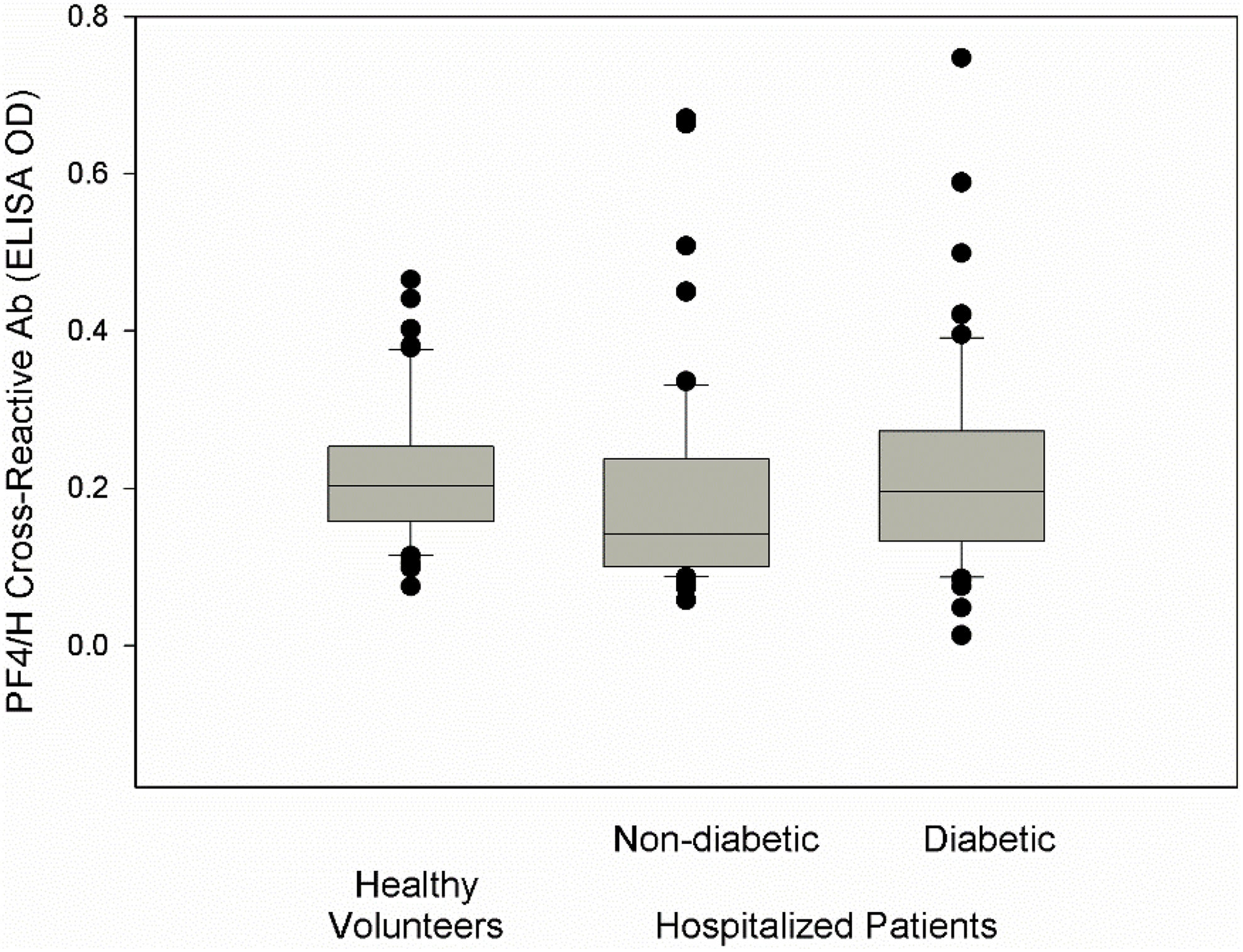
Box plot of PF4/H cross-reactive antibody levels comparing healthy volunteers to hospitalized patients with or without diabetes. Boxes indicate the median and upper and lower quartile values; the error bars delimit the 10th and 90th percentile and symbols designate outlying points. There were no significant differences by Dunn's Multiple Comparisons Test.
In a previous outpatient study, 26 HIT antibody OD was significantly lower in patients with diabetes compared to nondiabetic endocrine patients and healthy volunteers. In that study the patients with diabetes were more frequently using one or more conventional medications which we hypothesized might have had an overall beneficial effect. In the present study also, patients with diabetes were more likely taking medications compared to nondiabetics (Table 1), but no particular medication was associated with a significantly lower PF4/H antibody level. In general, the use of medications with anti-inflammatory or antiplatelet activity might be expected to prevent or suppress expression of a PF4-mediated immune stimulus. We compared the impact of diabetes on PF4/H antibody titer among patients in relation to therapy with the medications listed in Table 1. Seven patients, either mild cases or newly diagnosed diabetics, were not on medication at the time of this study. This group had higher PF4/H-cross-reactive antibody ODs compared to the majority of patients without diabetes or with medically treated diabetes (Figure 2). Understandably, given the small number of individuals in the group, the difference in median PF4/H antibody OD did not reach statistical significance (analysis of variance; P = .07).
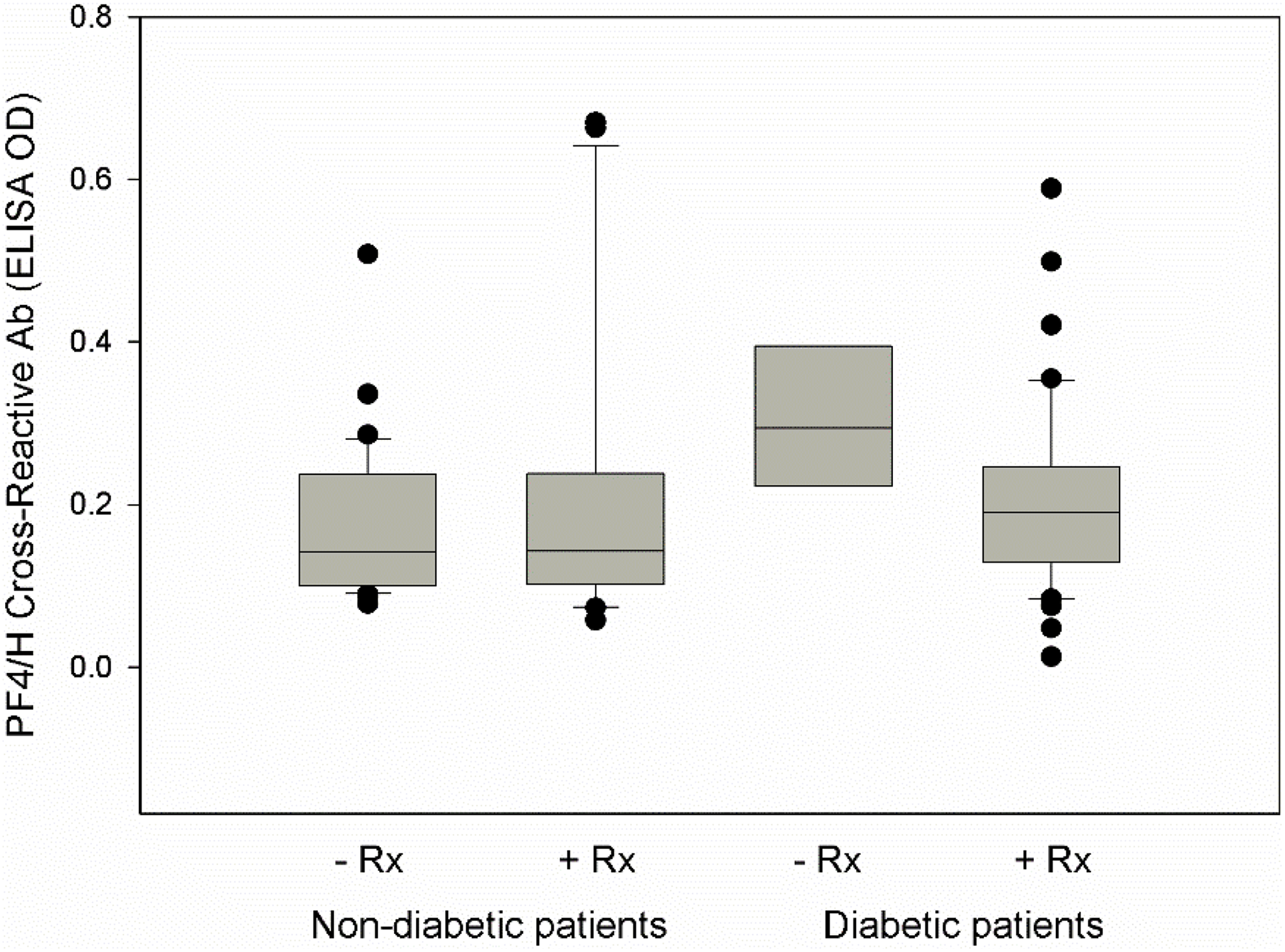
Box plot of PF4/H cross-reactive antibody levels among patients with or without diabetes and with or without medical therapy (Rx). The differences were not significant (P = .07) by one way analysis of variance.
Comparisons were also made based on the cause for hospitalization as determined by chart review. Patients with infectious diagnoses such as pneumonia, cellulitis, or urinary tract infections, for example, were compared to the patients with cardiovascular, pulmonary, renal, or other conditions (Figure 3). Among all hospitalized patients, there was no significant difference in PF4/H cross-reactive antibody OD due to the presence of infection alone. However, the group of patients who had both diabetes and an infectious condition, but not patients with diabetes with other conditions, had significantly higher antibody OD compared to patients without diabetes regardless of their reason for hospitalization.
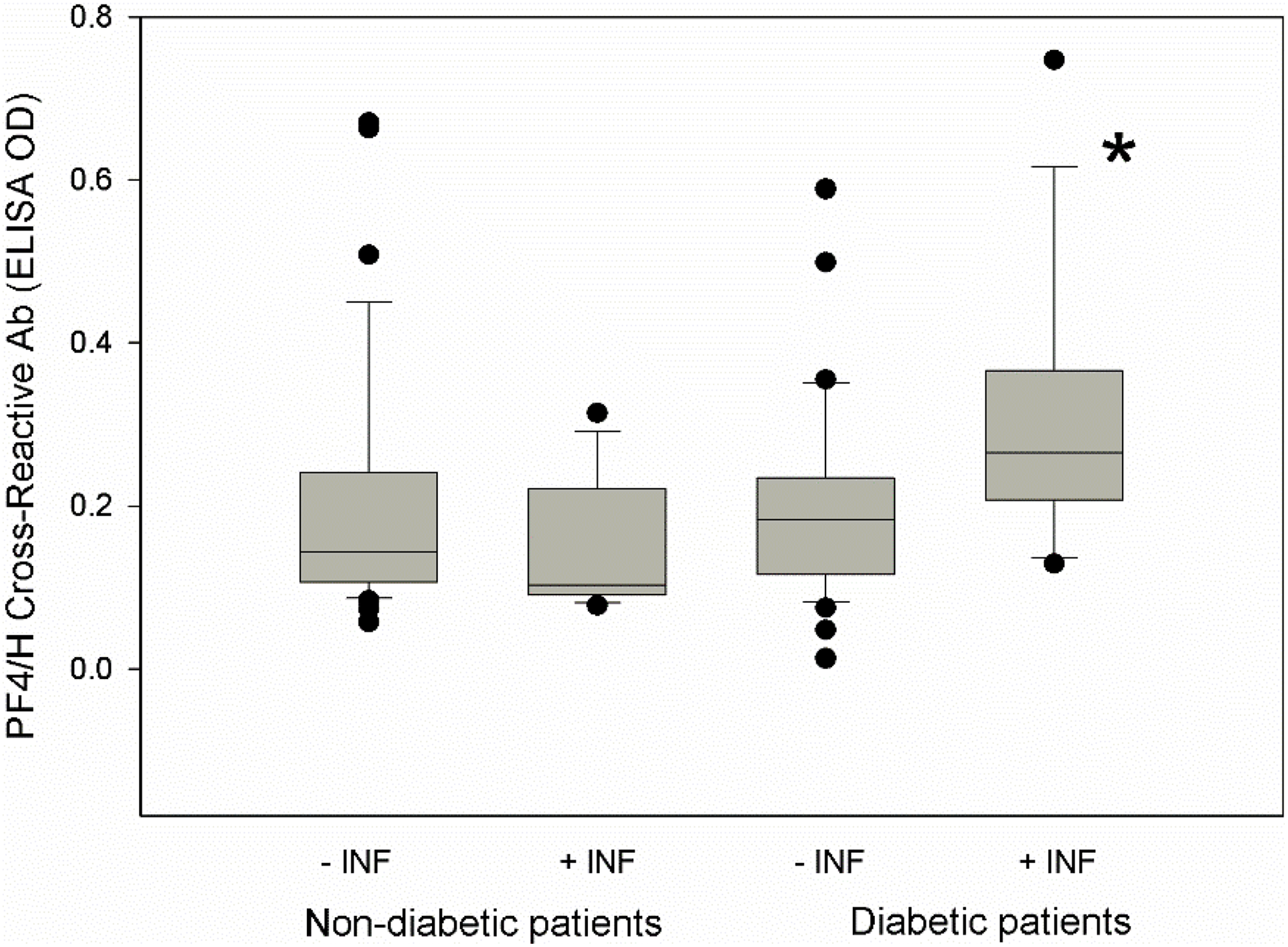
Box plot of PF4/H cross-reactive antibody levels among patients with or without diabetes and with or without an infectious condition (INF). * indicates P < .05 compared to patients without diabetes by Dunn's Multiple Comparisons Test.
Inflammatory Cytokines
Four inflammatory cytokines were measured by ELISA in specimens from the volunteer group and all hospitalized patients; there was no correlation between PF4/H antibody OD and level of any of the cytokines among the 3 populations. The only significant difference detected in mean cytokine levels was that IL-6 and IL-8 were lower in the healthy control group compared to hospitalized patients.
This finding is not surprising. The volunteer donors were younger, healthy, and of normal body weight and these cytokines are elevated in response to tissue damage, inflammation, infection, malignancy, and other disease states. 26,28,29 These inflammatory cytokines were somewhat lower in groups of patients taking medications, however only the reduction in IL-8 in diabetic patients taking angiotensin receptor blockers was statistically significant (P = .014).
There were no significant differences in mean levels of IL-6, IL-8, TNF α, or CD40L between the diabetic and nondiabetic groups regardless of cause for hospitalization. We also looked for correlations among cytokine levels in each group, shown in Table 2. In healthy individuals all 4 cytokines showed a highly significant, strong positive correlation (r = 0.6-0.8) indicating a coordination of increase or decrease in level of all cytokines measured. In contrast the patient groups had less integrated response patterns. In these groups, the positive correlation of IL-6 to IL-8 or TNF-α was weaker (r = 0.4-0.5). The only other significant relationship was a very strong positive correlation between TNF-α and CD40L in patients without diabetes.
Correlation of Cytokine Responses in Healthy Volunteers Compared to Hospitalized Patients with or without Diabetes.a
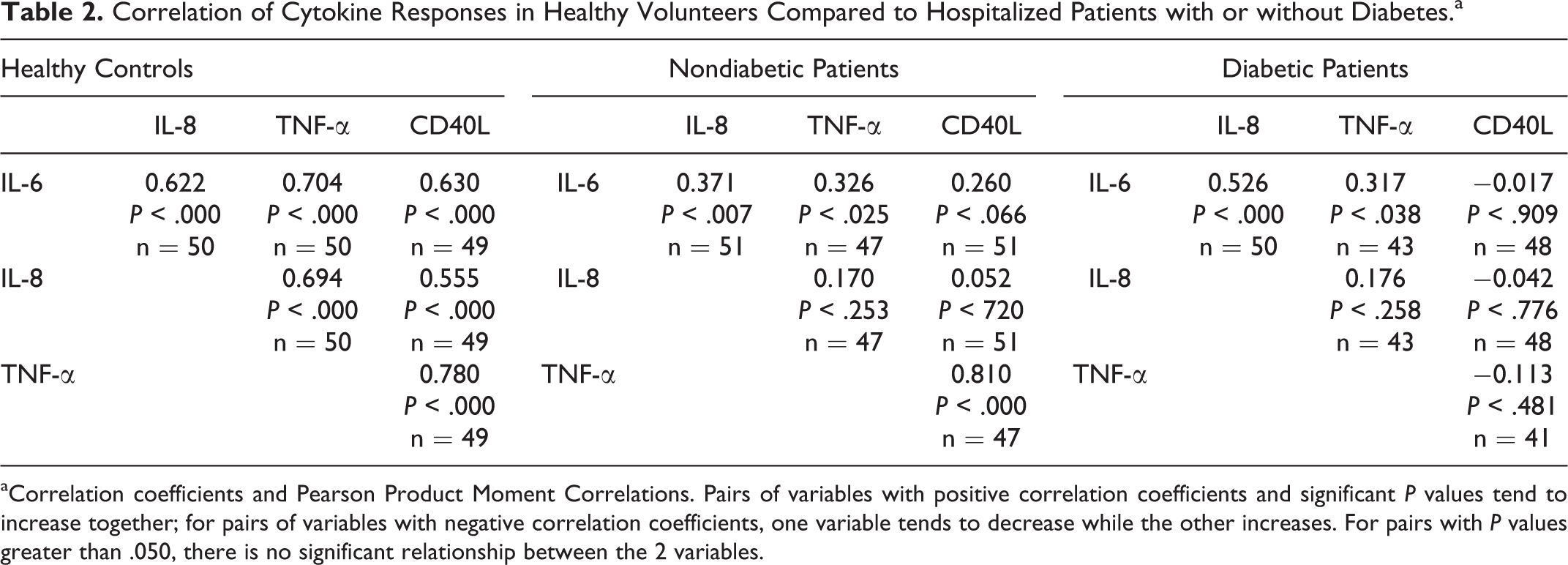
aCorrelation coefficients and Pearson Product Moment Correlations. Pairs of variables with positive correlation coefficients and significant P values tend to increase together; for pairs of variables with negative correlation coefficients, one variable tends to decrease while the other increases. For pairs with P values greater than .050, there is no significant relationship between the 2 variables.
Discussion
Platelet factor 4 is a multifunctional defense peptide released from activated platelets whether functioning in hemostasis, inflammation, or immune surveillance. 30,31 Antibodies elicited as a result of heparin therapy, which are responsible for the HIT syndrome, are known to be generated by the conformation of PF4 when bound to the heparin molecule. 1,16,32 Since this discovery, and with the means to measure these antibodies by ELISA, 2 it has been learned that PF4/H-cross-reactive antibodies are measurable in some individuals with no proximal heparin exposure, and can in some cases lead to clinically relevant cases of HIT. 9 -12 Cases of spontaneous PF4/H seropositivity are typically preceded by an infectious, inflammatory, or surgical event. 13,14,33 Thus, there is evidence suggesting that PF4 binding to bacterial cell walls or to RNA/DNA nucleotides or glycosaminoglycans released by trauma or surgery creates the PF4 neoepitope which provokes antibody generation. 17,18 It is possible that an immune response can be influenced by the cumulative expression of conformationally altered PF4 whether it is bound to activated or damaged cells, invading pathogens or exogenous therapeutic drugs such as heparin. 14,17,34 Patients with conditions associated with platelet hyperactivity and elevated PF4 often have measurable PF4/H antibody prior to heparin administration, 35 -37 are more likely to develop HIT 36,38,39 and to experience poorer outcomes. 40,41 Diabetes is associated with platelet hyperactivity, elevated PF4, and vascular compromise 24,25 which together may present an immunogenic, PF4 target conformation. Also, diabetes is associated with a higher likelihood of developing PF4/H antibodies in heparin-treated patients with vascular disease. 42
Results of this study indicate that the prevalence of PF4/H antibody ELISA-positive results does not differ among hospitalized patients with diabetes, hospitalized nondiabetic patients and healthy controls. However, the level of PF4/H cross-reactive antibodies may be higher in patients with diabetes when other risk factors are also present. Our results with hospitalized patients found a significantly higher OD for PF4/H cross-reactive antibodies associated with infection but only among patients who also have diabetes. Patients with either infection or diabetes had equivalent OD ranges; only patients with the dual risk factors had significantly higher ODs. These results suggest that there may be an additive interaction between independent conditions where each has some potential to elicit PF4-reactive antibodies. Heparin-induced antibody seroconversion, even in the absence of the clinical HIT syndrome, is significant because it has been associated with poorer outcomes, such as increased length of hospital stay, 43,44 higher incidence of 30-day death or myocardial infarction 45,46 and increased mortality in hemodialysis patients. 47,48
Common comorbidities of diabetes, such as macrovascular disease, obesity, hypertension, and hyperlipidemia, may contribute to vascular dysfunction/inflammation and relative abundance of PF4 that may increase the risk of antibody generation. 49 -54 Medical therapies to address these conditions, most of which have platelet modulating activity, 55 -57 may abrogate these potentially immunogenic conditions. Our results show slightly higher PF4/H antibody ODs in the patients with diabetes who were taking no medications. This suggests that therapies commonly used to control comorbidities associated with diabetes may also attenuate the risk of developing PF4/H cross-reactive antibodies. In fact, our previous study of well-controlled, outpatient diabetics indicated a significantly lower PF4/H antibody titer compared to other outpatient populations and healthy volunteers. 26
In contrast to our expectations, but in agreement with other studies, 13,58 we did not find a relationship between inflammatory cytokine levels and presence of PF4/H cross-reactive antibodies. Although platelet activation or infection may have an influence on PF4/H cross-reactive antibody formation, there is no evidence herein that it is mediated through or dependent on specific cytokines. Our results also introduce a note of caution. We show that synchronization of inflammatory cytokine levels is not equivalent among different study populations, and that the coordination of immune response may be disrupted by illness or medical condition. Thus, any conclusions drawn regarding relationships between PF4/H cross-reactive antibodies and individual cytokines may not be the same for different patient populations.
The present study of heparin-naïve hospitalized patients with and without diabetes used the PF4/H antibody ELISA not as a surrogate for diagnosing an immune response to heparin, but as an indication of the presence of endogenous PF4/H cross-reactive antibodies. Rather than comparing the frequency of responses greater than the HIT diagnostic cut-off OD of 0.4, we compared the distribution of OD readings between patient populations. We found that the diagnosis of diabetes alone is not associated with a significant elevation in PF4/H-reactive antibodies. However our study raises the concern that diabetes with its common complications, when untreated or when challenged with concurrent infectious conditions, may result in potentially sensitizing PF4/H cross-reactive antibody formation.
This preliminary study is limited by the small sample size of each population. In particular, the number of individuals in subgroups of patients with and without diabetes, where interesting differences in PF4/H antibody OD were observed, was limited. Also no physical or clinical information, beyond gender and body weight, was available to characterize and compare volunteer blood donors to patient groups or to include in subgroup analyses. Rigorous statistical analyses of the potentially important observations will require future, larger studies designed to compare specific patient and control subpopulations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.