
Abstract
We conducted a prospective serial laboratory cohort study to assess the correlation of factor VIII (FVIII) levels in response to thrombolysis in patients with large vessel occlusion (LVO) and acute ischemic stroke (AIS). Patients with AIS with anterior circulation LVO were eligible for enrollment if treated within 4.5 hours from last seen normal with intravenous tissue plasminogen activator (tPA). Patients (n = 29) had a mean age of 71 years and median National Institute of Health Stroke Scale of 14. Baseline pre-tPA FVIII was not significantly correlated with clot burden score (−0.147, P = .447) or vessel recanalization (−0.133, P = .499). Median FVIII decreased significantly from baseline to 6 hours post-tPA (282% to 161%, P = .002), but delta in FVIII level did not correlate with vessel recanalization (0.013, P = .948). There was no difference between median FVIII level at baseline and 90 days post-AIS. FVIII level decreased significantly after tPA, but baseline FVIII level and early change in FVIII level were not significant predictors of clot burden, vessel recanalization after thrombolysis, or symptomatic hemorrhage.
Background
Large vessel occlusions (LVOs) account for 40% of ischemic strokes and only 13% to 50% reperfuse with intravenous tissue plasminogen activator (IV tPA). 1 Recently, 5 randomized controlled trials demonstrated the benefit of mechanical thrombectomy for LVO, 1 making early recognition and expedited delivery of these stroke patients to endovascular capable hospitals imperative. In-hospital triage for thrombectomy eligibility is currently limited to neurological assessment scales in centers without access to emergent vascular imaging. A blood biomarker either coupled with these assessments or by itself could simplify the triage decision if rapid acquisition of results were feasible. Identifying such a biomarker could lead to targeted adjunctive interventions to increase recanalization and ultimately diminish the death and disability among patients with LVO who are at high risk of deterioration. A surrogate marker of response to IV tPA and post-tPA hemorrhage is needed to improve patient selection in routine clinical practice and to refine the inclusion criteria for future recanalization clinical trials. Specifically, this surrogate marker could serve to increase acute ischemic stroke (AIS) treatment rates, facilitate even rapid prehospital triage, decrease rates of symptomatic intracranial hemorrhage (sICH), reduce exposure to radiation encountered in neuroimaging, and reduce the expenses incurred by patients, insurers, and clinical trials by eliminating redundant neuroimaging.
Hemostatic factors are frequently evaluated as a possible etiology for venous and arterial thromboembolism. The coagulation cascade is dynamic, and when a thrombus is formed, transient changes in local and systemic concentrations of clotting factors likely occur. Factor VIII (FVIII) complexed with von Willebrand factor is essential for the formation of thrombin. 2 Factor VIII is an independent risk factor for deep venous thrombosis with the risk increasing with higher levels, 3 and previous population-based epidemiologic studies have linked baseline FVIII activity to the development of coronary artery disease and ischemic stroke. 2,4 Interestingly, the association between FVIII and ischemic stroke is independent of other traditional vascular risk factors. 5 Furthermore, effect of FVIII on arterial thrombosis remains even after adjustment for risk factors such as age, hypertension, cholesterol, and ischemic heart disease, thus arguing for independent association of elevated FVIII with arterial thrombosis. 2 Little is known about the variability of FVIII levels in the setting of AIS and thrombolysis due to the retrospective nature of existing hospital-based studies. The objective of this pilot study was to determine the feasibility of prospectively measuring FVIII levels prior to treatment with IV tPA and following treatment. We hypothesized that baseline FVIII levels would be positively correlated with clot burden and inversely correlated with successful vessel recanalization.
Methods
Study Design, Setting, and Participants
This study was approved by the university institutional review board. Informed consent in written and oral format was obtained from the participant or his or her legal decision maker. We conducted a prospective pilot study to determine the feasibility of obtaining serial laboratory measurements of FVIII levels in patients with AIS with an LVO. Patients with AIS were screened in the emergency department (ED) at a comprehensive stroke center for eligibility (Table 1). We enrolled patients with LVO on computed tomography angiogram (CTA) or magnetic resonance angiogram (MRA) who were treated with IV tPA within 4.5 hours of symptom onset. Patients on anticoagulant therapy and patients with a known factor deficiency were excluded. The FVIII levels were obtained on arrival in the ED, at 6 hours, followed by 12-hour intervals up to 72 hours. Patients returned to clinic 90 days post stroke for their final FVIII level and disability outcome assessments. Figure 1 shows the study timeline.
Inclusion and Exclusion Criteria.
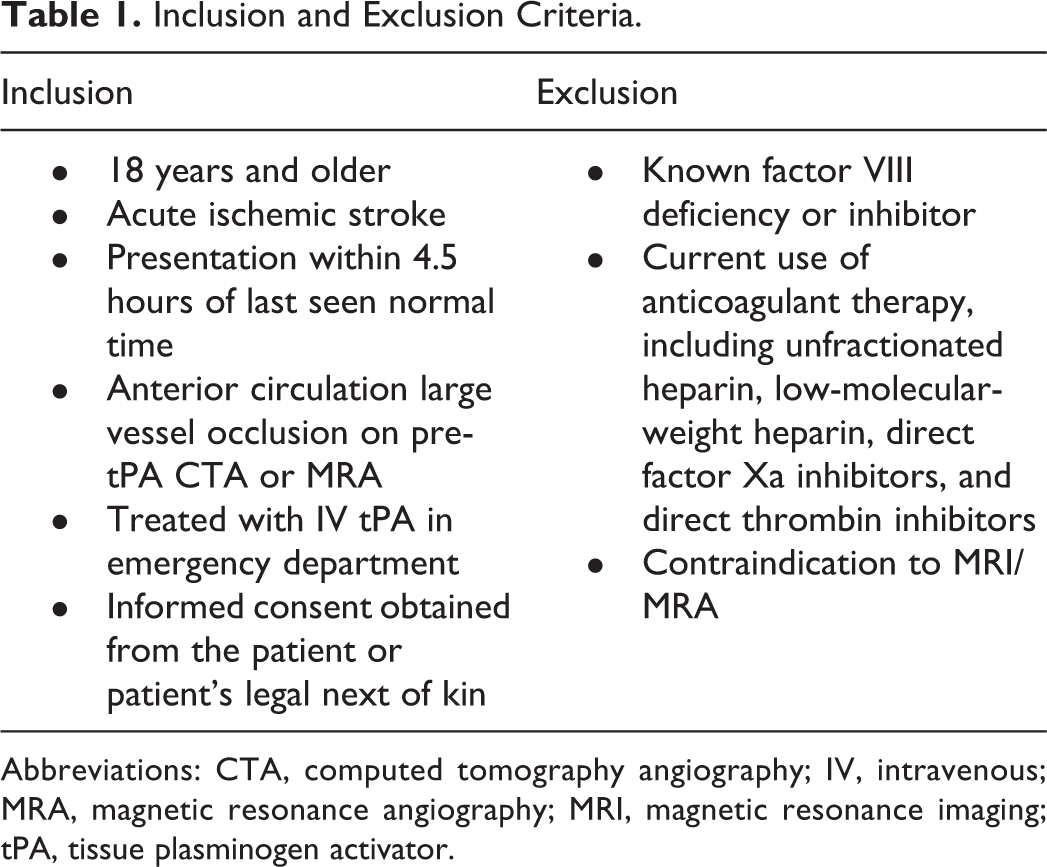
Abbreviations: CTA, computed tomography angiography; IV, intravenous; MRA, magnetic resonance angiography; MRI, magnetic resonance imaging; tPA, tissue plasminogen activator.
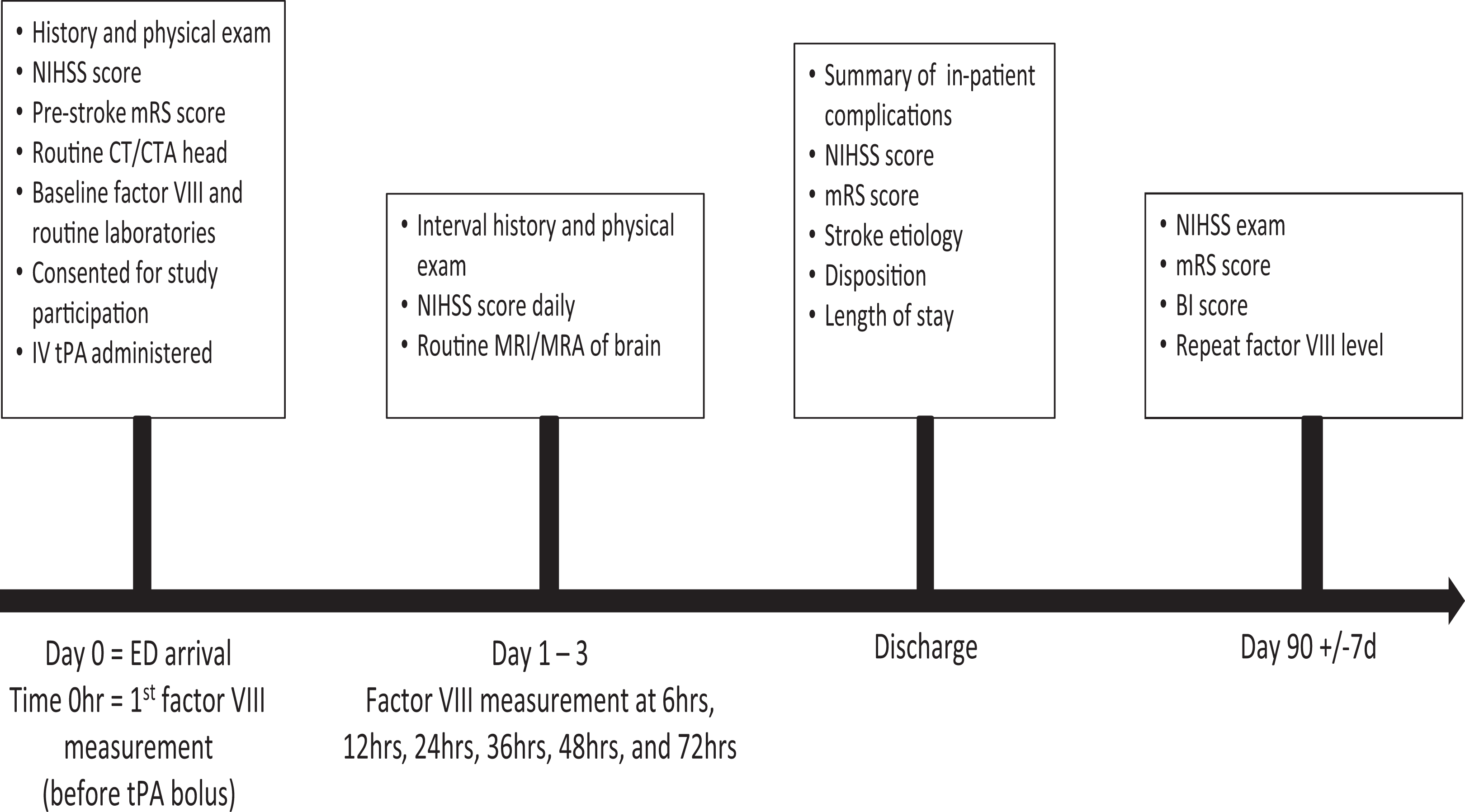
Study outline.
The blood obtained was centrifuged within 2 hours per laboratory protocol. Plasma was siphoned and frozen if the assay could not be immediately performed. The FVIII levels were considered elevated if exceeding our laboratory normal reference range of 150%.
Measurements and Definitions
Clot burden was assessed by applying the clot burden score. 6 The clot burden score is applied only to the symptomatic hemisphere (Supplemental Figure). Pre-tPA vessel patency was assessed with CTA or MRA and with MRA post-tPA and categorized as occluded, partially recanalized, and completely recanalized. Decision for endovascular treatment for LVO was per the treating physician’s discretion. Patients with neuroworsening (defined as increase in National Institute of Health Stroke Scale [NIHSS] by ≥4 points) and brain hemorrhage were categorized as having sICH. Patients with no evidence of stroke on MRI brain were classified as averted stroke. Good discharge disposition was defined as discharge to home or inpatient rehabilitation, and a good discharge outcome was defined as modified Rankin Scale (mRS) score of 0 to 2.
Outcomes Measures
The main outcome was feasibility of obtaining serial FVIII levels in the setting of LVO stroke. We measured recruitment rates, consent rates, and study completion rate.
Statistical Methods
The number of patients enrolled was not based on power analysis as this was a pilot study intended to provide proof of concept and estimate the effect size in anticipation of powering a larger trial. Categorical variables were reported as frequencies and percentages. Continuous variables were reported as median (minimum-maximum) or mean (standard deviation), as appropriate. Unadjusted regression models, as well as multivariable models adjusted for previously reported confounders (eg, gender, age, race, diabetes, body mass index, serum triglyceride level), were performed. The following hypotheses were tested using linear regression:
Results
Participants
From October 2012 to April 2016, 1316 patients with AIS were screened (Figure 2). Thirty-eight patients met inclusion criteria and 31 were offered participation based on availability of coinvestigators for the consent process. Over 93% of eligible patients (n = 29) consented to enrollment. Among the recruited patients, only 1 patient lost to follow-up. The 3 study protocol violations identified were used to adjust the study protocol to prevent future study protocol violations. Although the protocol violations were problematic, there was no harm done to the study participants during these protocol violations.
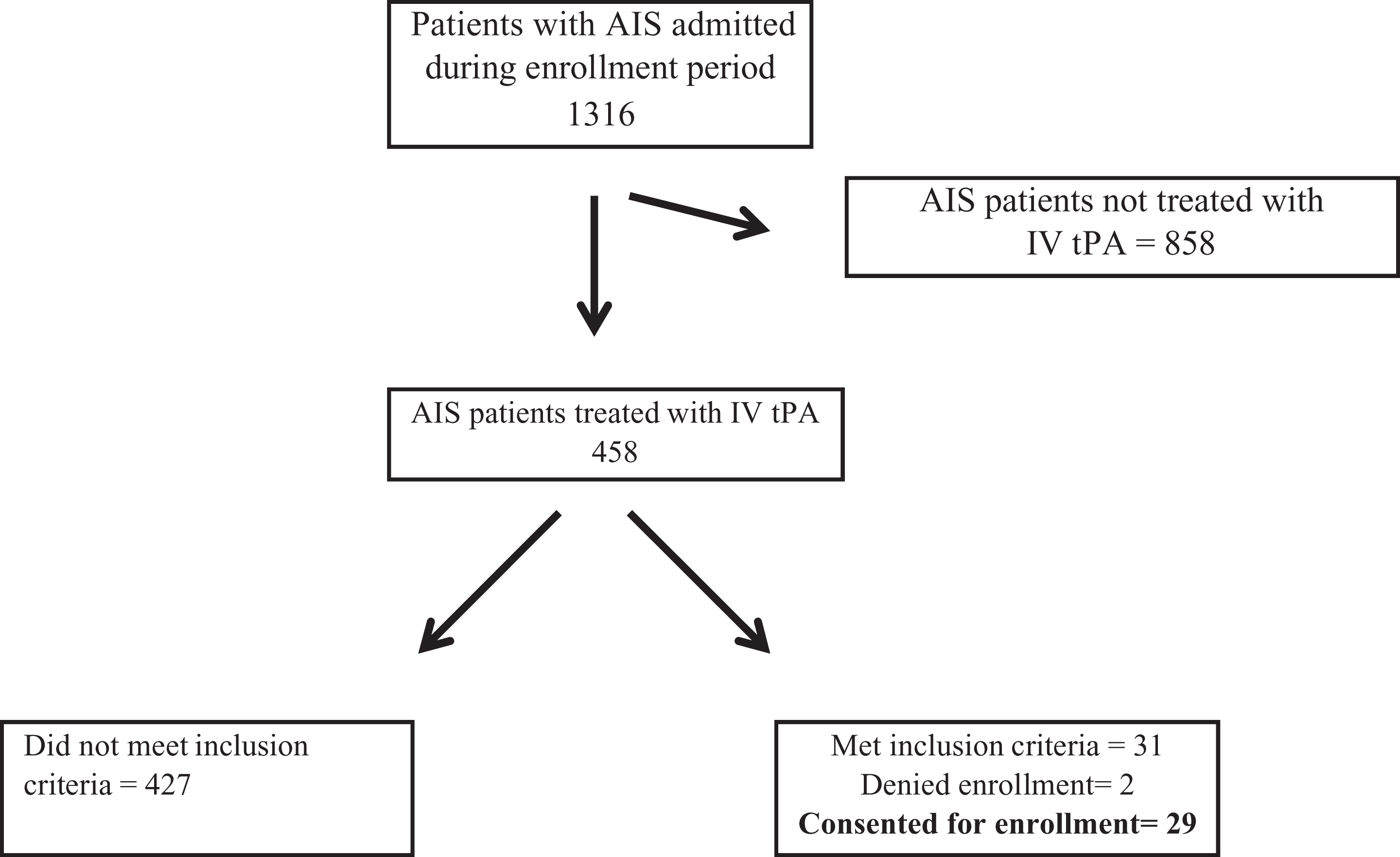
Enrollment cascade.
Forty-eight percent (n = 14) of those enrolled were women and 62% (n = 18) were black. The mean age was 71 years (standard deviation: 14). The pre-tPA median NIHSS was 14 (2-29), the median pre-tPA clot burden score was 7 (0-9), and the post-tPA clot burden score was 10 (2-10). Twenty-one percent (n = 6) received adjuvant endovascular therapy. Fifty percent (n = 14) had complete recanalization, 25% (n = 7) had incomplete recanalization, and 25% (n = 7) did not recanalize. Eighty-nine percent (n = 25) had a diffusion-weighted imaging hyperintensity and 10.7% (n = 3) were classified as averted stroke. The remainder of the baseline characteristics of the cohort is in Table 2.
Baseline Characteristics.
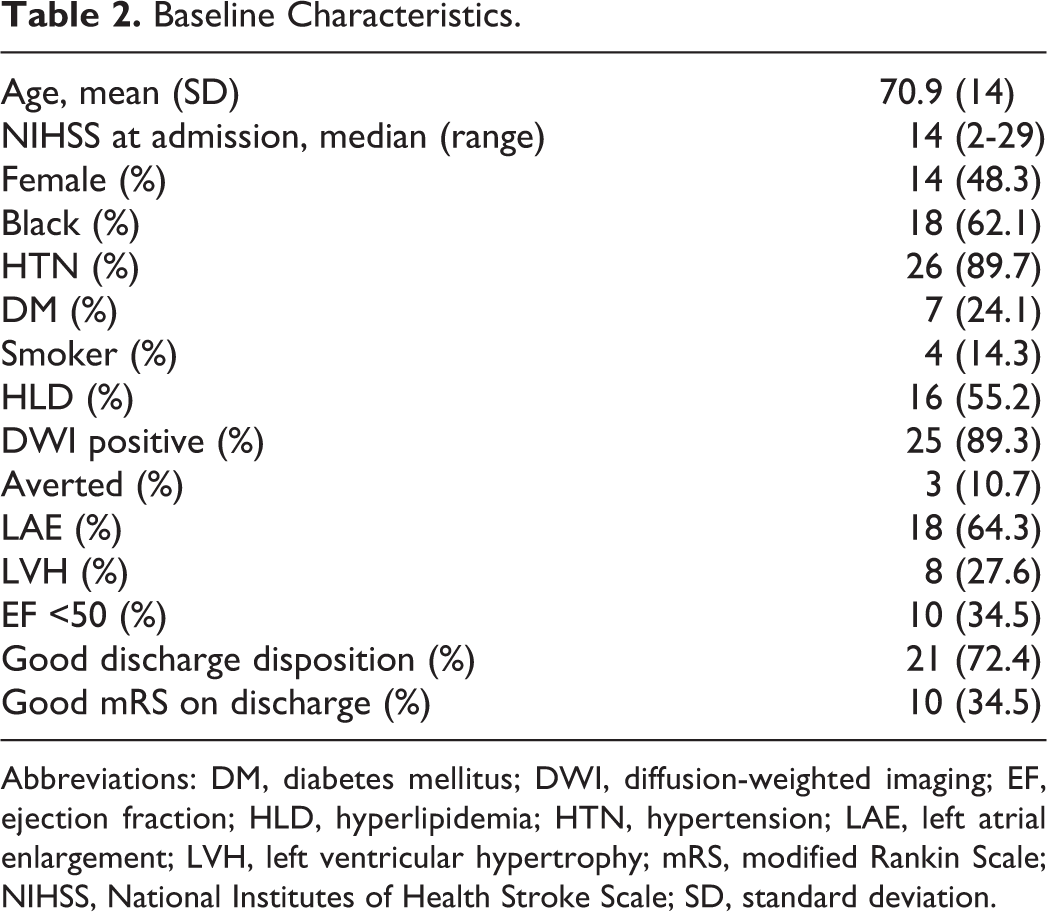
Abbreviations: DM, diabetes mellitus; DWI, diffusion-weighted imaging; EF, ejection fraction; HLD, hyperlipidemia; HTN, hypertension; LAE, left atrial enlargement; LVH, left ventricular hypertrophy; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; SD, standard deviation.
Outcomes
We were able to obtain FVIII measurements on 100% of participants on arrival in the ED, 100% at 6 hours, followed by 12-hour intervals up to 72 hours and 97% at 90 days. The median FVIII decreased significantly from baseline to 6 hours post-tPA (282% to 161%, P = .002; Table 3). The FVIII level declined in 83% (24/29) of patients. Of these 24 patients, 18 (75%) recovered FVIII level within the next 72 hours and 92% (22/24) had follow-up FVIII >200% during 72 hours of follow-up. There was no difference between median FVIII level at baseline and 90 days post-AIS.
Factor VIII Levels.
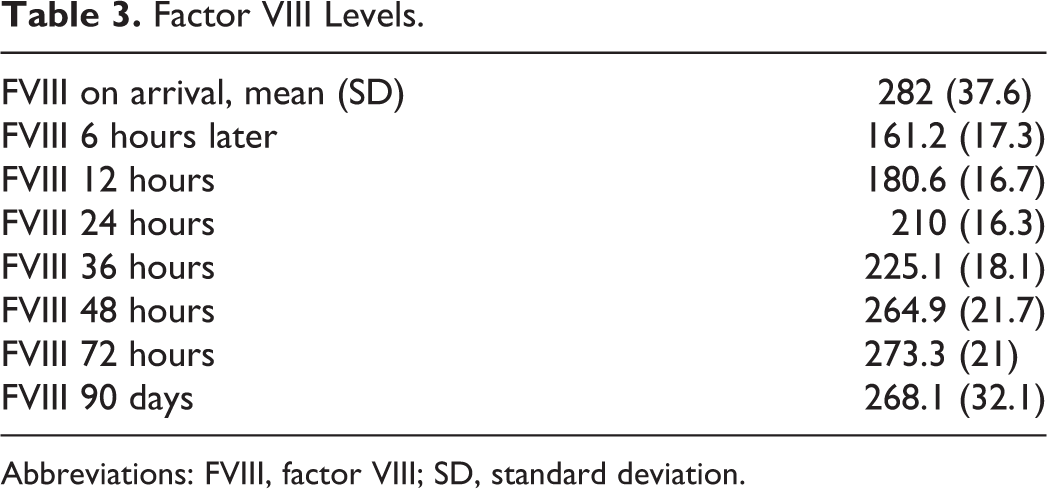
Abbreviations: FVIII, factor VIII; SD, standard deviation.
Baseline FVIII was not significantly correlated with clot burden (−0.147, P = .447) or vessel recanalization (−0.133, P = .499). Change in FVIII (FVIII at 6 hours minus baseline FVIII level) was not significantly correlated with vessel recanalization (0.013, P = .948).
No patients experienced an sICH. Baseline FVIII was not significantly correlated with averted stroke (−0.181, P = .358). Change in FVIII was not significantly correlated with averted stroke (0.036, P = .854).
Neither baseline FVIII level nor the change in FVIII level, as continuous values, was associated with vessel recanalization (odds ratio [OR]: 0.99, 95% confidence interval [CI]: 0.99-1.00, P = .488; OR: 1.00, 95% CI: 1.00-1.01, P = .946). Neither the baseline nor change in FVIII level was associated with averted stroke (OR: 0.99, 95% CI: 0.98-1.01, P = .364; OR: 1.00, 95% CI: 0.99-1.01, P = .848). Neither baseline nor change in FVIII was associated with good discharge mRS (0-2; OR: 0.99, 95% CI: 0.99-1.00, P = .136; OR: 1.00, 95% CI: 1.00-1.01, P = .762; Figure 3).
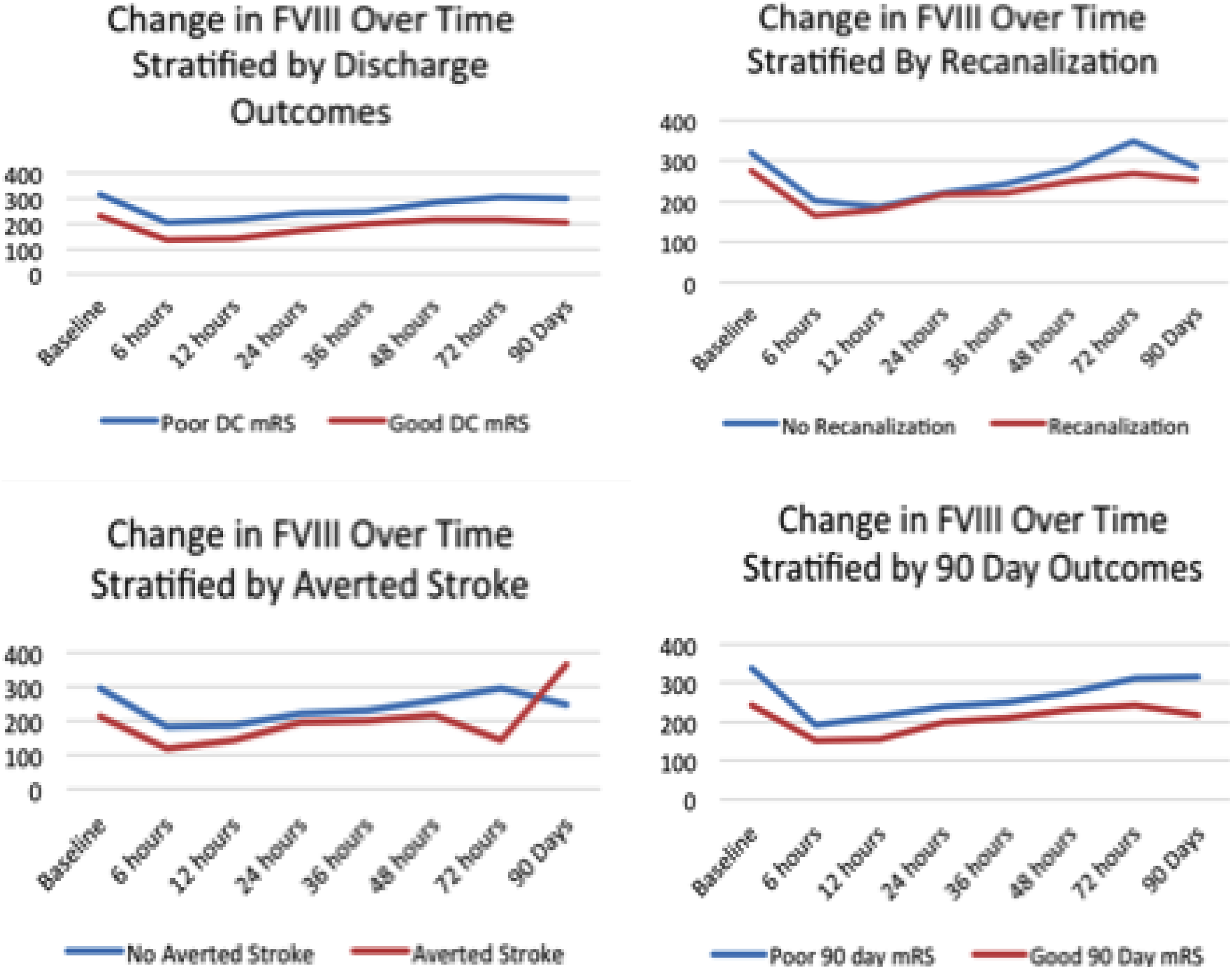
Changes in factor VIII level over time. Neither baseline or change in factor VIII level were associated with good discharge outcome, vessel recanalization, averted stroke, and 90-day outcome.
Discharge and Safety Outcome
Twenty-one (72.4%) patients had a good discharge disposition and 10 (34.5%) patients had a good discharge mRS.
Discussion
This study demonstrated the feasibility of assessing FVIII levels prospectively in patients with large vessel AIS. Our study found that all patients had elevated pre-tPA FVIII levels except one. This is consistent with findings from other studies, where patients with FVIII >150% had an increased risk of thrombosis by 4.8 times. 3 Ours was the first study to demonstrate high prevalence (∼70%) of severely elevated (>200%) FVIII level in patients presenting with hyperacute LVO; only 3% (1/29) of patients had normal FVIII level prior to treatment with thrombolytic. Because we only studied patients with documented LVO, we did not provide evidence that acute FVIII levels could distinguish between LVO and other ischemic stroke types. Future studies should be conducted to explore the prevalence of elevated FVIII levels in different ischemic stroke subtypes.
This study demonstrates dynamic FVIII levels in relation to thrombolysis. Eighty-three percent experienced a drop in FVIII level after thrombolysis. All but one of these patients had recovery of severely elevated FVIII level by 72 hours after thrombolytic treatment. If measurement of FVIII level is considered during the acute phase of stroke, it should probably be delayed for 72 hours in patients who received recanalization therapy based on our study results. Another prospective study has demonstrated a precipitous drop in FVIII level followed by steady rise in FVIII levels 24 hours postthrombolysis in an unselected population of patients 7 ; thus, the reasons behind different times in steady rise after thrombolysis needs to be explored further. Only 50% of the patients in this feasibility study achieved complete recanalization, which could have influenced the relationship among baseline and change in FVIII levels with clot burden prior to or after recanalization. Because we found no relationship between the reduction or magnitude of reduction in FVIII level and recanalization, FVIII measurement in the hyperacute phase of stroke probably has little value in predicting recanalization of LVO.
Persistently elevated FVIII levels 24 hours postthrombolysis was demonstrated to have poor functional outcomes at 90 days in patients inclusive of all AIS subtypes 7 ; however, we were unable to demonstrate the relation of functional recovery to severely elevated FVIII level at any time point in our study, likely due to small sample size. Being said that, we were also unable to demonstrate good functional outcome with reduction in FVIII levels or its difference postthrombolysis arguing for reasons other than FVIII level driving the good functional outcomes in these patients.
A significant drop in FVIII level was seen at 6 hours after administration of IV tPA. It is likely that this decrease in FVIII level was due to clot dissolution through a plasmin-mediated phenomenon; however, our study design could not measure volume directly and was not powered to detect such a difference. Alternatively, the FVIII measurement may have been affected by tPA-related changes in the PTT and not a true measurement of the FVIII level. Future studies can be designed to allow for vessel imaging around 6 hours postthrombolysis, particularly in patients who receive adjuvant thrombectomy.
Our study demonstrates high prevalence of elevated FVIII (94%) and severely elevated FVIII level (56%) 90 days after LVO ischemic stroke, suggesting elevation in FVIII was not an epiphenomenon of stroke; rather premorbid elevation of FVIII may be a risk factor for ischemic stroke and potentially for more severe ischemic strokes. The optimal antithrombotic for stroke prevention in patients with chronic elevation of FVIII is unknown and remains a potential target of investigation.
Conclusion
We were successfully able to demonstrate feasibility of this prospective cohort study. A larger study with a control group consisting of AIS due to non-LVO should be conducted in order to explore the pathophysiology behind elevated FVIII in large vessel strokes.
Supplemental Material
Supplementary_material_781045 - Factor VIII in Acute Cerebral Ischemia Pilot Study
Supplementary_material_781045 for Factor VIII in Acute Cerebral Ischemia Pilot Study by Digvijaya Navalkele, Amelia Boehme, Karen Albright, Cindy Leissinger, Laurie Schluter, Melissa Freeman, Stacy Drury, Ramy El Khoury, T. Mark Beasley, and Sheryl Martin-Schild in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The authors would like to acknowledge the Tulane Neurology Residents and Tulane Medical Center nurses for their important roles in identifying potential candidates for our study and for adherence to the timing of study-related laboratory procedures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: Dr Sheryl Martin-Schild was supported in part by 1 U54 GM104940 from the National Institute of General Medical Sciences of the National Institutes of Health, which funds the Louisiana Clinical and Translational Science Center. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.