
Abstract
Considering the role of hemorheology in coronary circulation, we studied blood viscosity in patients with juvenile myocardial infarction. We examined whole blood viscosity at high shear rate using the cone-on-plate viscosimeter Wells-Brookfield ½ LVT and at low shear rate employing a viscometer Contraves LS30 in 120 patients (aged <46 years) with myocardial infarction, at the initial stage and subsequently 3 and 12 months after. At the initial stage, patients had an increased whole blood viscosity in comparison to normal controls. This hemorheological profile was not influenced by the cardiovascular risk factors, nor by the extent of coronary lesions, even if some differences were evident between patients with ST-segment elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI). The blood viscosity pattern at the initial stage did not influence recurring ischemic events or the onset of heart failure during an 18 months’ follow-up. The neutrophil to lymphocyte ratio did not affect the blood viscosity pattern. We reevaluated 83 patients 3 months after and 70 patients 12 months after the acute coronary syndrome, and we found that the hemorheological parameters were still altered in comparison to normal controls at both times. We observed an impairment of the hemorheological pattern in young patients with myocardial infarction, partially influenced by the infarction type (STEMI and NSTEMI) and persisting in the long term.
Introduction
Blood viscosity influences the risk of cardiovascular events 1 and plays a role in the pathophysiology of thrombosis 2 and atherothrombosis. 3,4 Several studies have explored blood viscosity in acute myocardial infarction (AMI) and its influence on some clinical and prognostic aspects. Some hemorheological variables seemed to distinguish ST-segment elevation myocardial infarction (STEMI) from patients with non-STEMI (NSTEMI), 5 but this finding was not confirmed by another study. 6 In patients with STEMI, a significant correlation between the left ventricular ejection fraction (LVEF) and some hemorheological parameters was observed. 7 Some authors described prolonged hemorheological impairment in AMI survivors not selected for age, 8 and a similar behavior was observed in the follow-up of patients with acute coronary syndromes. 9 All these literature data take on a specific relevance considering the role of blood viscosity in the regulation of myocardial microcirculation 10 and coronary blood flow 11 and the interaction between blood viscosity and endothelium. 12 An impairment of blood rheology could be involved in the phenomenon of secondary coronary slow flow: the slow progression of the contrast medium through the coronary tree in the absence of demonstrated organic lesions. 13 –15 In a small group of patients with slow coronary flow, an alteration in erythrocyte aggregation was observed. 16
The neutrophil to lymphocyte ratio (NLR) is considered as a prognostic factor in AMI. 17 –21 It seems to reflect the systemic inflammatory condition induced by AMI, and in fact, it is positively correlated with high sensitivity-C reactive protein (hs-CRP)in patients with AMI 22,23 as well as in healthy patients. 24 Previously, in small groups of patients with juvenile myocardial infarction belonging to this survey, we examined, as indicator of inflammation, elastase, a plasma marker of polymorphonuclear (PMN) leukocyte activation, that was significantly increased in comparison to normal controls, not only at the initial stage but also at three 25 and twelve 26 months after AMI. As it is known, elastase seems to reflect the inflammation status that characterizes these patients. Until now, the possible relation between NLR and the blood rheology profile in AMI has not been investigated.
Acute myocardial infarction has a low incidence in young adults, between 2% and 10% of all cases with AMI. 27 –31 Acute myocardial infarction 32 –34 or acute coronary syndromes 35,36 in young patients show peculiar risk factors, clinical, angiographic, and prognostic characteristics. In juvenile myocardial infarction, the risk factor pattern is different from older people. Cigarette smoking is the most common factor, followed by family history of coronary artery disease (CAD). In younger people, hypercholesterolemia is the third cardiovascular risk factor, while arterial hypertension and diabetes mellitus are not frequent. Regarding the clinical picture, young patients reach hospital earlier than other patients, helping efficacy of revascularization and complication treatment. In young people, often there is not CAD or just 1 coronary vessel is affected by significant narrowing; 3-vessel disease is infrequent. Consequently, the reperfusion with percutaneous intervention is more frequent than coronary artery bypass graft, and this has a favorable influence on prognosis. In young people, AMI seems to have a lower incidence of complications such as early and late heart failure, angina, reinfarct, and atrioventricular block. Death during hospitalization and after 6 months are both significantly reduced.
Since 2001, we have participated in the “Sicilian study on juvenile myocardial infarction,” evaluating the hemorheological profile in patients who had AMI at an age <46 years. The investigation was carried out at the initial stage and 3 and 12 months after the AMI onset. In our previous reports, 37,38 we described an increase in whole blood viscosity (WBV), plasma and serum viscosity, and a decrease in erythrocyte deformability.
In this conclusive study, we reexamined the data previously obtained in young patients with AMI in the light of the follow-up performed in most of them. Although the short-term prognosis of AMI is favorably influenced by young age, 34 the long-life expectancy of these patients makes the control of their long-term risk profile particularly relevant.
Materials and Methods
The enrollment of patients with recent AMI aged <46 years lasted from 2001 to 2007. In each patient, we examined the main cardiovascular risk factors, including current smoking habits, family history of CAD, hypercholesterolemia, arterial hypertension, and diabetes mellitus. Family history consisted in any first-grade relative with clinical manifestation of CAD at age <55 years. Hypercholesterolemia was defined as a total cholesterol level >220 mg/dL and/or the use of lipid-lowering drugs. Arterial hypertension was defined as a systolic blood pressure >140 mm Hg and/or a diastolic blood pressure >90 mm Hg and/or the use of antihypertensive drugs. Diabetes mellitus was defined as a fasting blood glucose level ≥126 mg/dL and/or the use of hypoglycemic agents. Coronary angiography was performed in all the patients, except when consent was refused or when the hospital in which the AMI was diagnosed was very far from the Cardiac Catheterization Laboratory of our University Hospital.
In each patient, LVEF was evaluated by echocardiography.
On fasting venous blood, we evaluated the following hemorheological determinants: WBV at the shear rate of 450 s−1, using the cone-on-plate viscometer Wells-Brookfield ½ LVT (Middleboro, Massachusetts); WBV at the shear rate of 0.51 s−1 employing a viscometer Contraves LS30 (proRheo GmbH, Althengstett, Germany); Hematocrit (Ht) obtained using a micromethod technique; WBV at 450 s−1/Ht × 100; and WBV at 0.51 s-1/Ht × 100.
An automated blood cell count was carried out on the same sample used for the hemorheological evaluation and employed to calculate the NLR.
The same variables were measured in 83 patients with AMI 3 months after AMI and in 70 patients 12 months after AMI.
A clinical follow-up of the patients with AMI was conducted to investigate about the onset of new ischemic events or heart failure. We analyzed data obtained from 98 patients followed up to 18 months after the initial AMI, including some patients in whom the rheological evaluation at 3 and/or 12 months had not been performed.
The rheological study was also performed in a group of 50 control patients free of medical diseases as assessed by clinical history, physical examination, electrocardiography, and routine hematological and urine analysis. The ethical committee approved the study, and each patient gave informed consent.
Statistical Analysis
Data were expressed as means (standard deviation [SD]) The Student t test for unpaired data was used to compare normal controls to patients with AMI. The differences in demographic characteristics other than age were evaluated using the Fisher exact test. The subgroups of patients with AMI with a different number of risk factors or stenosed coronary vessels were compared using the 1-way analysis of variance model, completed by the Bonferroni posttest. At the initial stage, patients with AMI were also divided into 2 subgroups according to different criteria (see Results section), and every time the Student t test for unpaired data was employed to compare the subgroups between each other. The correlation between LVEF and hemorheological parameters was examined using the linear regression. The difference between the hemorheological parameters at the initial stage and those at 3 and 12 months, respectively, was examined using the Student t test for unpaired data.
Results
We enrolled 120 patients (109 men and 11 women) with recent AMI. The demographic characteristics of control patients and patients with AMI are shown in Table 1. Patients with AMI were older than control patients (P < .001), although the age range was similar. No difference was present in gender or body weight distribution. The time interval between AMI onset and the initial examination was 13 (7) days.
Demographic Characteristics in Control Patients and Patients With AMI.
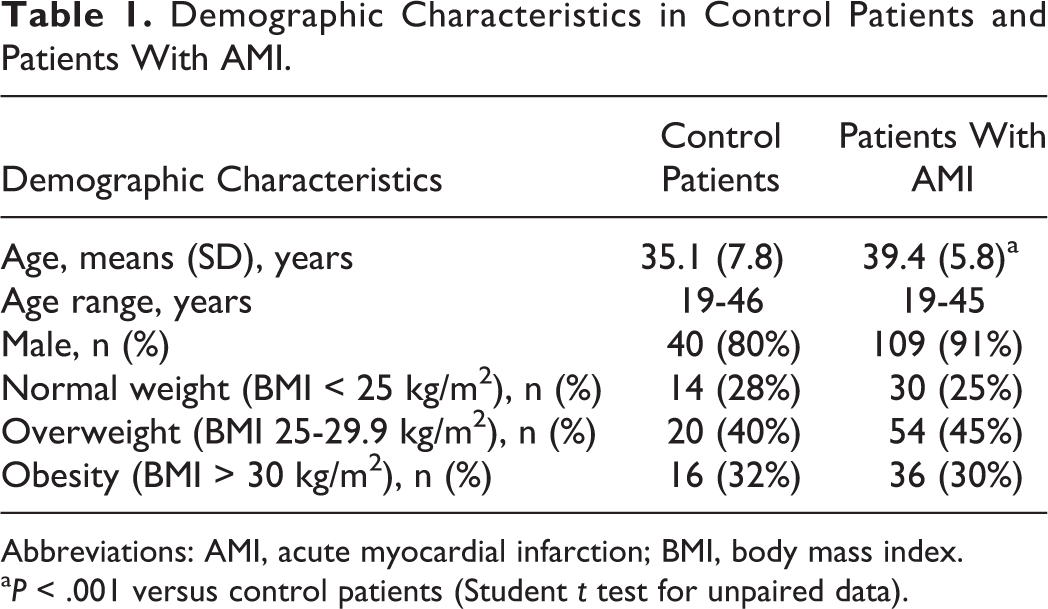
Abbreviations: AMI, acute myocardial infarction; BMI, body mass index.
aP < .001 versus control patients (Student t test for unpaired data).
Left ventricular ejection fraction was 54.52 (7.31%) in the whole group; in patients with STEMI (n = 86), LVEF was 53.88 (7.72%), and in patients with NSTEMI (n = 34), the LVEF was 56.14% (6.00%; not significantly different vs STEMI).
Patients with AMI were subdivided into 3 groups, having 0 or 1, 2, and 3 or more risk factors, respectively. Thirty-nine patients had 0 or 1 risk factor, 39 had 2 risk factors, and 42 had 3 or more of them. Coronary angiography was performed in 103 patients, subdivided into 3 groups according to the extent of coronary lesions: 23 patients did not show any significant coronary stenosis, 46 had a single-vessel disease (defined as a stenosis >70% in 1 coronary artery), and 34 had a multivessel disease, defined as a stenosis >70% in at least 2 coronary vessels.
During the follow-up, 5 patients developed heart failure, 15 a new ischemic event (12 angina and 3 AMI), and 4 a new ischemic event associated with heart failure.
At the initial stage, patients with AMI showed significantly higher levels of rheological determinants in comparison to control patients (P < .001), with the exception of Ht (Table 2).
Means (SD) of the Hemorheological Determinants in 50 Control Patients and in 120 Patients With AMI at the Initial Stage.
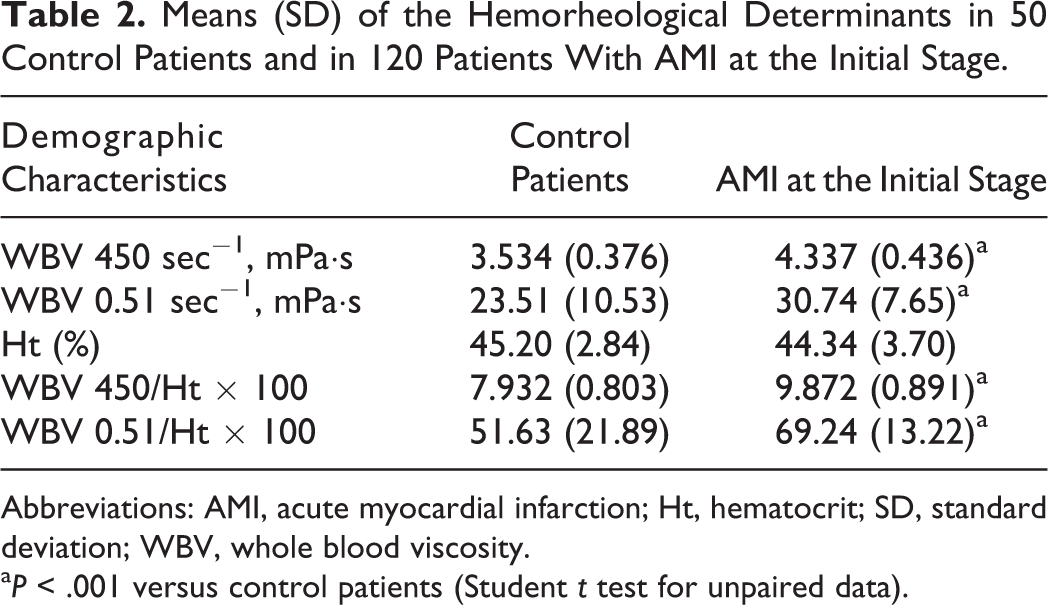
Abbreviations: AMI, acute myocardial infarction; Ht, hematocrit; SD, standard deviation; WBV, whole blood viscosity.
aP < .001 versus control patients (Student t test for unpaired data).
Subdividing patients with AMI according to the number of cardiovascular risk factors and to the number of involved coronary vessels, no significant difference was noted in any of the rheological variables.
At the initial stage, we subdivided patients with AMI according to 3 criteria: STEMI or NSTEMI; with or without ischemic events and/or heart failure at follow-up; and high or low NLR.
We found a difference in WBV at 450 sec−1 (P < .01) and in WBV at 450 sec−1/Ht ratio (P < .05) between patients with STEMI and NSTEMI; both parameters were in fact higher in STEMI in comparison to patients with NSTEMI (Table 3).
Means (SD) of the Hemorheological Determinants at the Initial Stage in Patients With AMI With or Without ST-Segment Elevation.
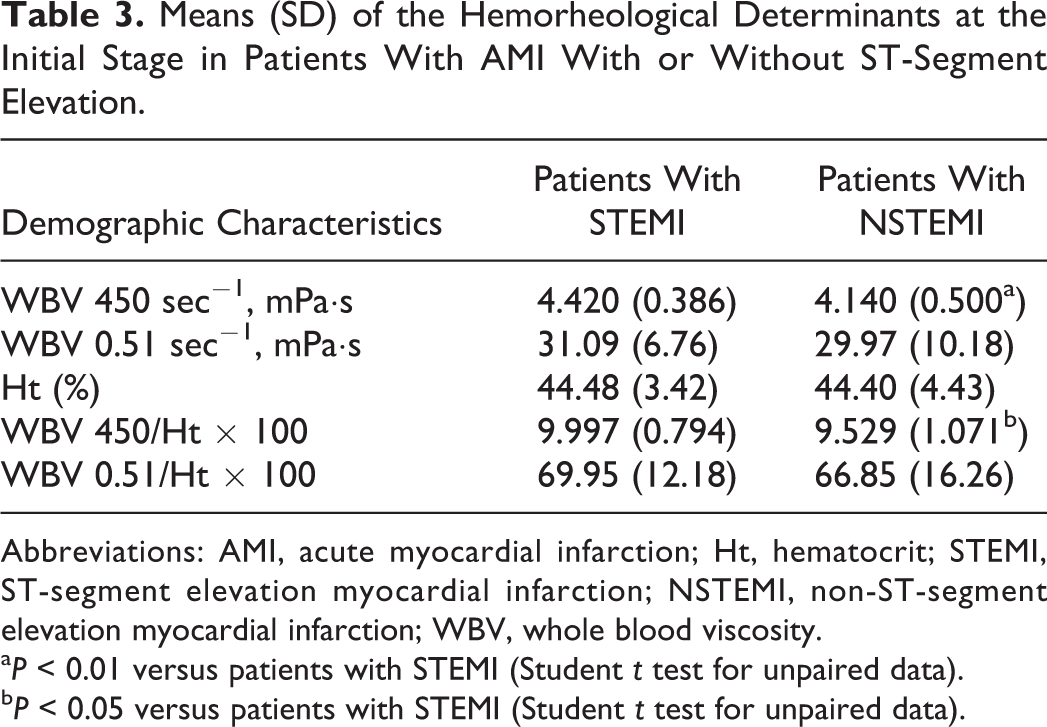
Abbreviations: AMI, acute myocardial infarction; Ht, hematocrit; STEMI, ST-segment elevation myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction; WBV, whole blood viscosity.
aP < 0.01 versus patients with STEMI (Student t test for unpaired data).
bP < 0.05 versus patients with STEMI (Student t test for unpaired data).
In the whole group, as well as in the 2 subgroups with STEMI or NSTEMI, no correlation between each hemorheological variable and LVEF was observed.
We compared the rheological determinants at the initial stage in patients with AMI who subsequently developed recurrent ischemic event or heart failure (n = 24) to those of patients who were free from such complications up to 18 months (n = 74). From this analysis (Table 4), no significant difference emerged between the 2 groups.
Means (SD) of the Hemorheological Determinants at the Initial Stage in Patients With AMI With or Without Cardiovascular Events During Follow-Up.
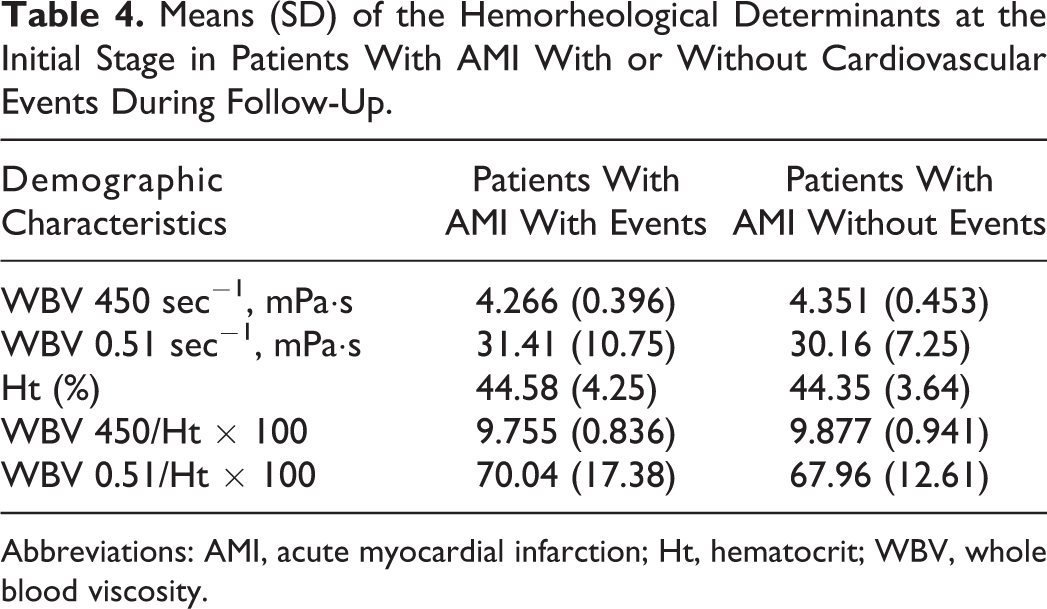
Abbreviations: AMI, acute myocardial infarction; Ht, hematocrit; WBV, whole blood viscosity.
We further subdivided the whole group of patients with AMI according to the median value of NLR, and there were no differences between the 2 subgroups (Table 5).
Means (SD) of the Hemorheological Determinants at the Initial Stage in Patients With AMI Having Low or High Neutrophil/Lymphocyte Ratio.
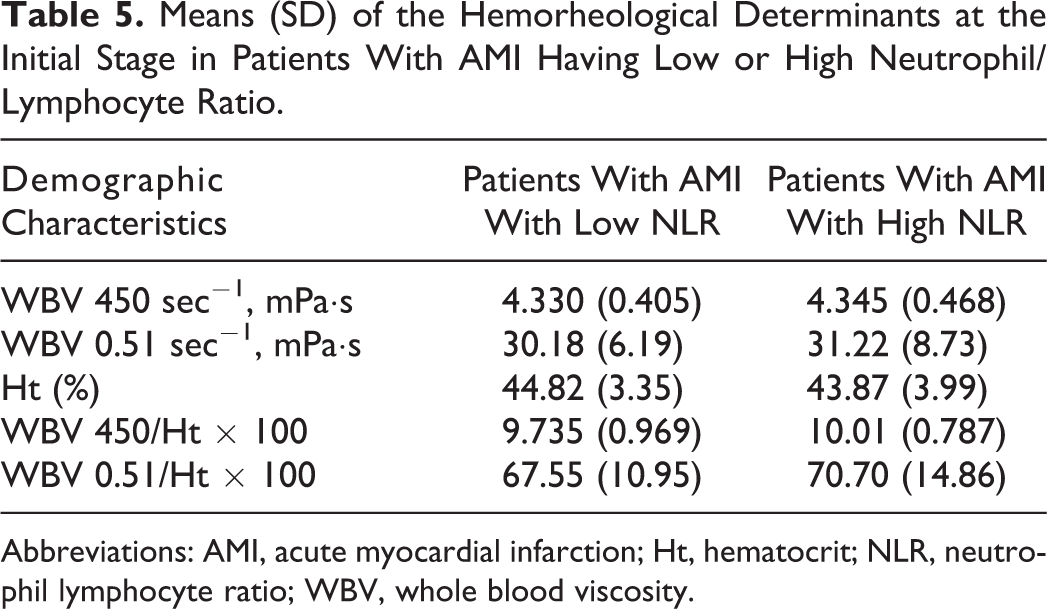
Abbreviations: AMI, acute myocardial infarction; Ht, hematocrit; NLR, neutrophil lymphocyte ratio; WBV, whole blood viscosity.
When we reexamined the patients with AMI 3 and 12 months after the acute event (Table 6), we observed that at both times the rheological determinants showed higher values in comparison to those found in normal controls (P < .001 for all the parameters at both times, with the exception of WBV at 0.51 sec-1 at 12 months, for which P < .01). No significant difference was present between rheological variables at 3 and 12 months.
Means (SD) of the Hemorheological Determinants in Control Patients and Patients With AMI After 3 and 12 Months.
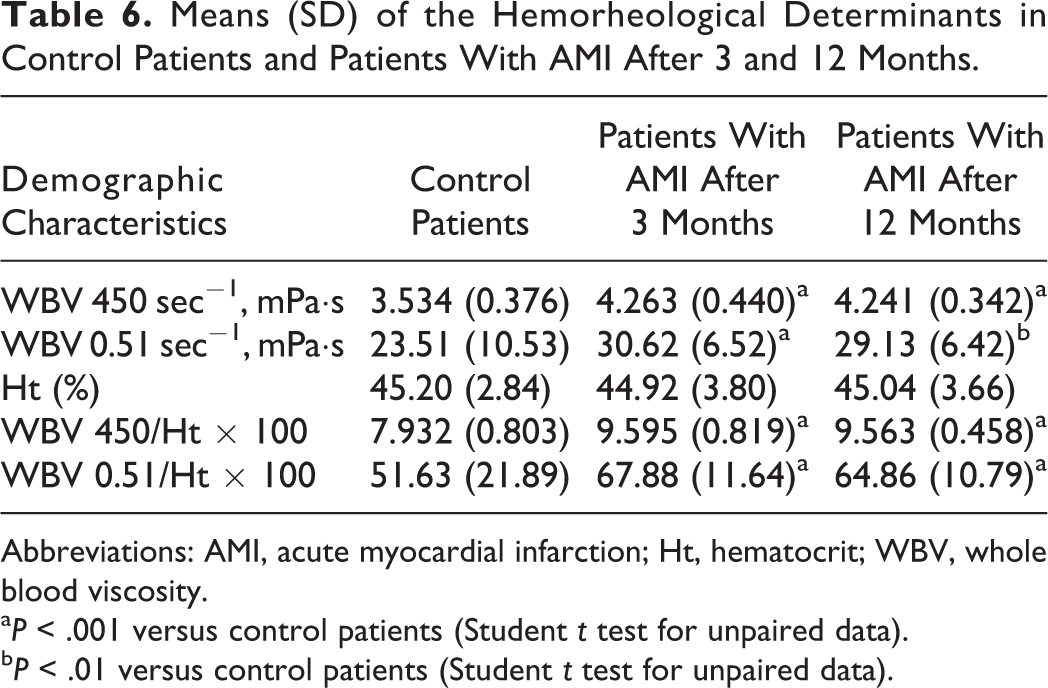
Abbreviations: AMI, acute myocardial infarction; Ht, hematocrit; WBV, whole blood viscosity.
aP < .001 versus control patients (Student t test for unpaired data).
bP < .01 versus control patients (Student t test for unpaired data).
Discussion
Our data show that in young patients with AMI, a hyperviscosity syndrome is present as widely demonstrated in patients with AMI not selected for age. These data confirm our previous results 37,38 but differ from what was found by other authors in a group of patients with similar age who had experienced an AMI 3 to 24 months earlier and whose plasma and blood viscosity values were not different from controls. 39 This latter data may be explained considering that the young patients with AMI were examined within a wider time interval from the acute event.
We observed an increased blood viscosity at high shear rate in patients with STEMI compared to patients with NSTEMI. In another study, ST-segment elevation did not influence the rheological profile of patients with AMI, 6 while other authors observed an increase in blood viscosity at low shear rate in STEMI compared to NSTEMI and unstable angina. 5
In our patients with AMI, the rheological pattern was not dependent on the number of cardiovascular risk factors or on the extent of coronary lesions as reported previously. 37,38
We did not observe any significant correlation between LVEF and each rheological variable in the whole group of patients with AMI or in STEMI and NSTEMI subgroups; in older patients with STEMI, a correlation between LVEF and blood viscosity was observed, 7 but in another study, only plasma viscosity was related to LVEF. 8
Neither the subdivision based on cardiac complications during the 18 months’ follow-up nor that based on NLR showed a difference in blood viscosity pattern. Differently, plasma viscosity in the same group of patients with AMI was significantly higher in patients who subsequently developed new ischemic events and/or heart failure and in those with high NLR. 40
A main point of this study was the persistence of the rheological abnormalities 3 and 12 months after AMI, a behavior already described by us in smaller groups of patients. 37,38
The hyperviscosity syndrome early detected after AMI has been commonly considered as part of an acute-phase reaction, likely to regress in a few weeks. In patients not selected for age, such behavior was in fact described in some studies, 41 –45 while other authors observed a persistent rheological alteration. 8,9,46,47
In our study, patients with AMI, after hospital discharge, received a prescription of drugs according to current recommendations (antiplatelet agent in 96.7%, statin in 75.3%, and a β-blocker in 64.4%) and were provided with counseling about lifestyle. As assessed during the follow-up, most of the patients gave up smoking and started to exercise regularly; those affected by arterial hypertension and diabetes mellitus achieved a better control of their diseases. Despite a satisfactory compliance with treatment, the hemorheological alteration persisted, substantially unchanged until 12 months after AMI.
A similar long-term persistence of alterations after AMI was also evident when we examined aspects of PMN leukocytes, such as membrane fluidity and cytosolic Ca++ concentration at baseline and after in vitro activation, 48 plasma markers of PMN and platelet activation, 49 and some parameters of the oxidative status. 50
These abnormalities could be partially caused by a proinflammatory genetic pattern and could favor the onset of AMI at a relatively young age. A high prevalence of some pro-inflammatory gene polymorphisms was actually observed in the Sicilian study on juvenile AMI. 51
Young patients with AMI could be a subset of patients with CAD whose proinflammatory genetic pattern, interacting with acquired factors such as smoking, precipitates acute myocardial ischemia.
The hemorheological abnormality that persists 12 months after the AMI onset needs a particular attention, especially considering the long-life expectancy of young patients with AMI. The follow-up of young patients with AMI performed by us is still short and does not allow us to hypothesize a prognostic role for hemorheological abnormalities, although in our patients plasma viscosity was higher in those who subsequently experienced adverse cardiac events. 40
A limitation of this further analysis of our survey of young patients with AMI is the lack of information about the hemorheological pattern later than 12 months after the acute event so that the relationship with the long-term clinical outcome remains questionable. However, considering the prognostic role of the rheological profile in cardiovascular morbidity and mortality, 52 the assessment of blood viscosity in patients with AMI at young age might deserve particular attention.
Conclusions
In conclusion, we observed an impairment of the blood rheological profile in patients who had AMI at a young age, partially influenced by the type of AMI (STEMI or NSTEMI). The persistence of the alteration after 3 and 12 months suggests a genetic mechanism and could have a prognostic relevance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.