
Abstract
The purpose of this study was to determine whether there are any differences in the levels of inflammatory, thrombotic, and collagen turnover biomarkers between individuals with atrial fibrillation (AF) and healthy volunteers. Circulating plasma levels of plasminogen activator inhibitor 1 (PAI-1), CD40-ligand (CD40-L), nucleosomes (which are indicators of cell death), C-reactive protein (CRP), procollagen III N-terminal propeptide (PIIINP), procollagen III C-terminal propeptide (PIIICP), procollagen I N-terminal propeptide, tissue plasminogen activator, and von Willebrand factor were analyzed as potential biomarkers of AF. Baseline plasma was collected from patients with AF prior to ablation surgery at Loyola University Medical Center. Individuals with AF had statistically significantly increased levels of PAI-1, CD40-L, and nucleosomes, when compared to the normal population (P < .0001). Additionally, there was a statistically significant increase in the CRP (P = .01), PIIINP (P = .04), and PIIICP (P = .0008) when compared to normal individuals. From this study, it is concluded that the prothrombotic, inflammatory, and collagen turnover biomarkers PAI-1, CD40-L, nucleosomes, CRP, PIIICP, and PIIINP are elevated in AF.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and is estimated to affect more than 3.03 million individuals in the United States. 1 It is thought that the prevalence of AF could increase to 12.1 million people by 2030. 2 The rising prevalence of AF is not solely attributed to the increasing elderly population but also to the increasing number of individuals with high body mass index, diabetes mellitus, hypertension, and other known risk factors for AF. 3,4 Atrial fibrillation is associated with significant morbidity and mortality due to the increases in adverse events, such as stroke, systematic embolism, and heart failure. The exact underlying pathophysiology of AF remains largely unknown. However, inflammation is hypothesized to play a major role in the development of AF due to increased oxidative stress, apoptosis, and fibrosis of the atria. Inflammation is also associated with the thromboembolic events observed in patients with AF due to its role in endothelial dysfunction, platelet, and coagulation cascade activation. 5 Inflammation of the left atrium is thought to subsequently lead to atrial structural remodeling and fibrosis. This results in increased heterogeneity of left atrial conduction and further propagation of AF. Due to the role of inflammation in the pathogenesis of AF, profiling inflammatory biomarkers may allow for risk stratification and aid in predicating outcomes in patients with this disease.
Atrial remodeling has an important role in the perpetuation of AF. A method of identifying the progression of atrial fibrosis could aid in assessing of the degree to which AF impacts cardiac architecture. The current reference for detecting myocardial and atrial fibrosis is through delayed enhancement magnetic resonance imaging (DE-MRI), which is both expensive and cannot be applied to patients with metallic or electronic implanted devices. 6,7 Measuring the levels of biomarkers of collagen turnover may allow for risk stratification, aid in identification of optimal treatments, and offer a cost-effective alternative to DE-MRI for individuals with AF.
The accumulation of fibrotic tissue in the heart is an essential adaptive mechanism to new pathophysiological conditions. 8 Increased collagen expression is a predominant component in the progression of extracellular matrix deposition in the heart, leading to structural remodeling in the atrium of individuals with AF. Measuring collagen turnover through procollagen propeptide plasma marker levels may be useful for assessing the degree of atrial fibrosis in AF. Type III collagen is derived from larger procollagen III molecules. The N-terminal (amino) and C-terminal (carboxyl) ends of procollagen III are removed by proteolytic cleavage during collagen synthesis and are released into the circulation as procollagen III N-terminal propeptide (PIIINP) and procollagen III C-terminal propeptide (PIIICP). The same process occurs for type I collagen, leading to the subsequent release of procollagen I N-terminal propeptide (PINP) and procollagen I C-terminal propeptide (PICP). Previous studies have shown that procollagen peptides, such as PICP and PIIICP, are associated with ventricular fibrosis in individuals with hypertension and postacute myocardial infarction, respectively. 9,10 Previous studies have demonstrated higher levels of collagen synthesis and degradation in individuals with persistent AF compared to normal individuals, using biomarkers such as C-terminal propeptide of collagen type-1 and C-terminal telopeptide of collagen type-1. 11 The role of collagen metabolism in atrial remodeling in AF prompted our investigation into the potential use of PINP, PIIINP, and PIIICP levels as noninvasive tools to assess atrial fibrosis.
Extracellular nucleosomes are complexes of histones and DNA that are released during cell death. Circulating nucleosomes may function as damage-associated molecular patterns (DAMPs) via receptor binding and triggering of signaling pathways. Previous studies have demonstrated high levels of circulating nucleosomes in diseases of inflammatory, ischemic, autoimmune, and neoplastic etiology. 12 The C-reactive protein (CRP) is an acute-phase reactant released by the liver during an inflammatory insult in response to proinflammatory cytokines. The CRP has an established association with AF and may serve as predictor of future AF development. 13
The CD40-ligand (CD40-L) is a transmembrane glycoprotein that is expressed in many cells including platelets, B cells, monocytes and macrophages, endothelial cells, smooth muscle cells, mast cells, and so on. 14 Studies have shown that CD40-L and the interaction with its receptor CD40 have a role in numerous inflammatory and thrombogenic pathways. 14 –16 Expression of CD40 and CD40-L on cells is induced by proinflammatory cytokines, and upon ligation, the activated receptor is internalized and stimulates downstream signaling pathways, such as nuclear factor-κB, thus upregulating inflammation. 16
The von Willebrand factor (vWF) is a multimeric glycoprotein that mediates platelet adhesion and aggregation at sites of endothelial injury and is a carrier protein for factor VIII. The AF is known to be associated with a prothrombotic state, and previous studies have shown the relationship between individuals with AF/enlarged left atrium and higher levels of plasma vWF. 17 Tissue plasminogen activator (tPA) is a naturally occurring enzyme that initiates fibrinolysis by activating the conversion of plasminogen to plasmin on the fibrin clot surface. Increased tPA antigen level is an indicator of increased fibrinolytic activity. 18
Plasminogen activator inhibitor 1 (PAI-1) belongs to the serine protease inhibitor (serpin) superfamily of proteins and functions to inhibit plasminogen activation by forming covalent complexes with tPA and urokinase-type plasminogen activator (u-PA). 19 Previous studies have shown increased tPA antigen and PAI-1 levels to be predictors for cardiovascular disease (CVD) events such as myocardial infarction, coronary insufficiency, heart failure, and stroke. 20 Stroke is a major adverse event associated with AF; profiling of prothrombotic markers such as vWF, tPA, and PAI-1 may serve as a method for assessing the risk of thromboembolic events in patients with AF. Currently, the CHADS-VASc score is the clinical assessment tool used to profile the risk of thromboembolism in individuals with AF. 21 These biomarkers may complement the CHADS-VASc score in this patient population.
Materials and Methods
Plasma samples from patients with AF were used for this study. The age of the patients ranged from 18 to 81 years with a mean age of 59.1 years. Whole blood was obtained under an institutional review board-approved protocol. Baseline whole blood samples were drawn from 50 patients with AF prior to ablation surgery for AF at Loyola university medical center. The blood samples were collected into tubes containing 3.2% (0.109 mol/L) sodium citrate and immediately centrifuged at 3000 × g for 15 minutes. The platelet-poor plasma supernatant was collected, aliquoted, and stored at −70°C until analysis. Samples were analyzed in a blinded fashion without access to the patient’s clinical information.
Eligibility Criteria
To be eligible for this study, patients had to be aged 18 years or older with a diagnosis of nonvalvular AF and be receiving treatment at Loyola University Medical Center as an inpatient or outpatient. Patients were excluded from the study if they were critically ill with an acute stroke, acute myocardial infarction, severe heart failure, sepsis, or were being mechanically ventilated. Due to effects that pregnancy can have on biomarker levels, females who were pregnant or nursing mothers were excluded from the study.
Controls
Normal human plasma samples from nonsmoking, drug-free volunteers were obtained from a commercial laboratory (George King Biomedical, Overland Park, Kansas) and the University of Utah. George King Biomedical controls were collected from patients ranging in age from 19 to 54 years, with a mean age of 32 years, while control samples from the University of Utah were collected from patients ranging in age from 50 to 78 years, with a mean age of 64 years.
Methods
Commercially available enzyme-linked immunosorbent assay (ELISA) kits were used per kit instructions to measure the levels of PINP, PIIINP, and PIIICP and were obtained from MyBioSource (San Diego, California). These kits employ a quantitative sandwich enzyme immunoassay technique to quantify the levels of PINP, PIIINP, and PIIICP. The ELISA kit to profile nucleosomes was obtained from Roche Diagnostics (Mannheim, Germany). This kit employs a quantitative sandwich enzyme immunoassay technique to quantify the levels of cell death. The ELISA kits for the assessment of CRP, tPA, vWF, and PAI-1 were obtained from Hyphen BioMed (Neuville-sur-Oise, France). These kits employ a quantitative sandwich enzyme immunoassay technique to quantify the levels of CRP, tPA, vWF, and PAI-1. The ELISA kits to measure the levels of CD40-L were obtained from R&D Systems (Minneapolis, Minnesota). This kit employs a quantitative sandwich enzyme immunoassay technique to quantify the levels of CD40-L. All ELISA kits contained standards and controls provided for calibration purposes.
Statistical Analysis
This was performed using Microsoft Excel and Graphpad Prism Software version 7. The biomarker analysis compared the plasma values of patient with AF with the aggregated control values, except for the CD40-L and PAI-1 assays, which were compared to the George King Medical samples. The results were expressed as mean (standard deviation) and percentage change from normal mean. The groups were compared using the nonparametric and nonpaired Mann-Whitney U test. A P value <.05 was considered statistically significant.
Results
Comparison of Collagen Metabolism Biomarkers in Controls Versus Patients With AF
As seen in Figure 1A and B, the circulating plasma levels of PIIINP and PIIICP were significantly elevated in the AF group compared to the control group (P < .04 and P < .008, respectively). As seen in Figure 1C, the PINP levels were not statistically different in the AF group compared to the control group and demonstrated a large variability in both populations (P = .24; Table 1).
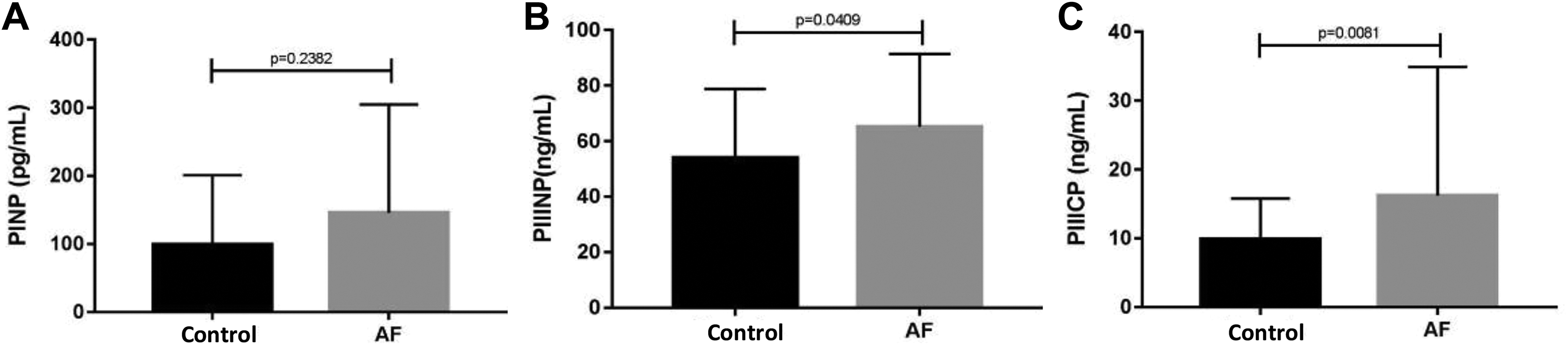
Comparison of the various collagen turnover biomarkers in patients with AF and in healthy controls. (A) demonstrates the comparison of PINP; (B) shows the comparison of PIIINP; and (C) shows the comparison of PIIICP. AF indicates atrial fibrillation; PAI-1, plasminogen activator inhibitor 1; PINP, procollagen I N-terminal propeptide; PIIICP, procollagen III C-terminal propeptide; PIIINP, procollagen III N-terminal propeptide.
Comparison of Various Biomarkers of Collagen Turnover, Inflammation, and Thrombogenesis.
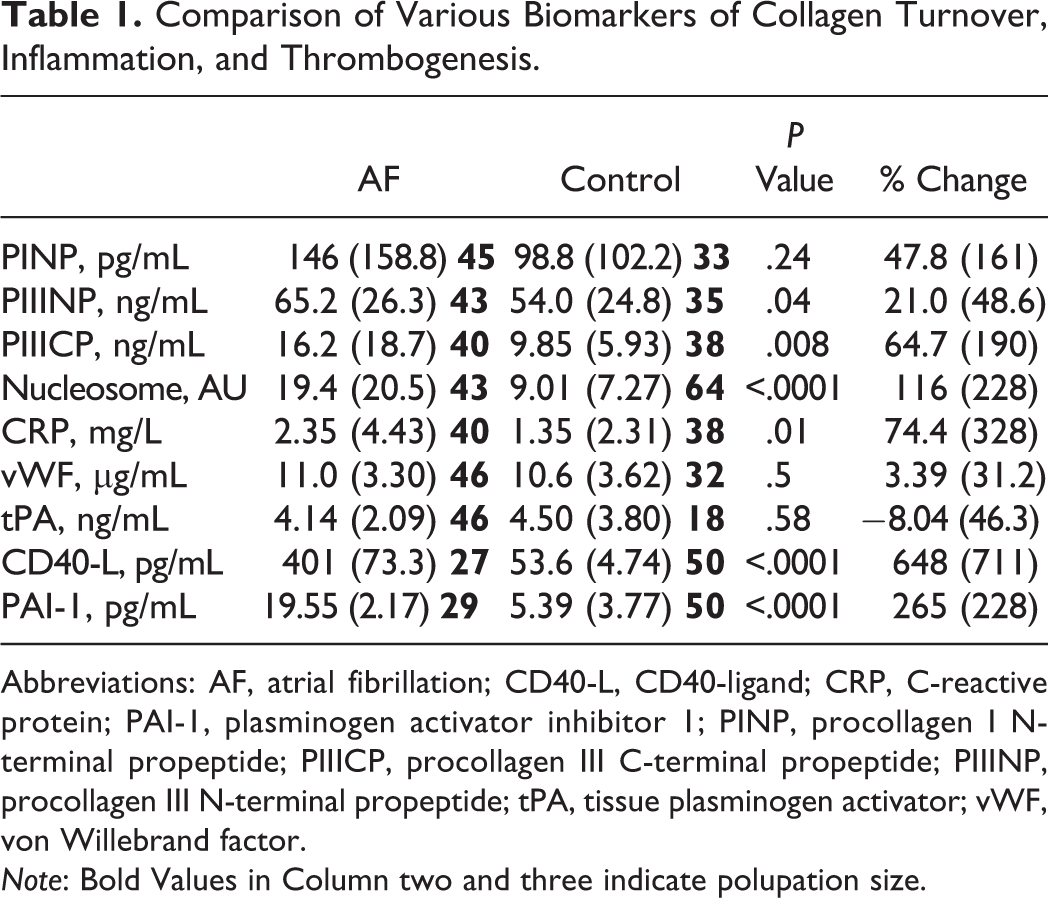
Abbreviations: AF, atrial fibrillation; CD40-L, CD40-ligand; CRP, C-reactive protein; PAI-1, plasminogen activator inhibitor 1; PINP, procollagen I N-terminal propeptide; PIIICP, procollagen III C-terminal propeptide; PIIINP, procollagen III N-terminal propeptide; tPA, tissue plasminogen activator; vWF, von Willebrand factor. Note: Bold Values in Column two and three indicate polupation size.
Comparison of Inflammatory Biomarkers in Controls Versus Patients With AF
As shown in Figure 2A, the circulating plasma levels of nucleosomes were significantly elevated in the AF group (19.4 [20.5] AU) compared to the control group (9.01 [7.27] AU; P < .0001). As shown in Figure 2B, the circulating plasma levels of CD40-L were significantly elevated in the AF group (401 [73.3] pg/mL) compared to the control group (53.6 [4.74] pg/mL; P < .0001). As seen in Figure 2C, the CRP levels in patients with AF (2.35 [4.43] mg/L) were also significantly elevated compared to the control group (1.35 [2.31] mg/L; P = .01).
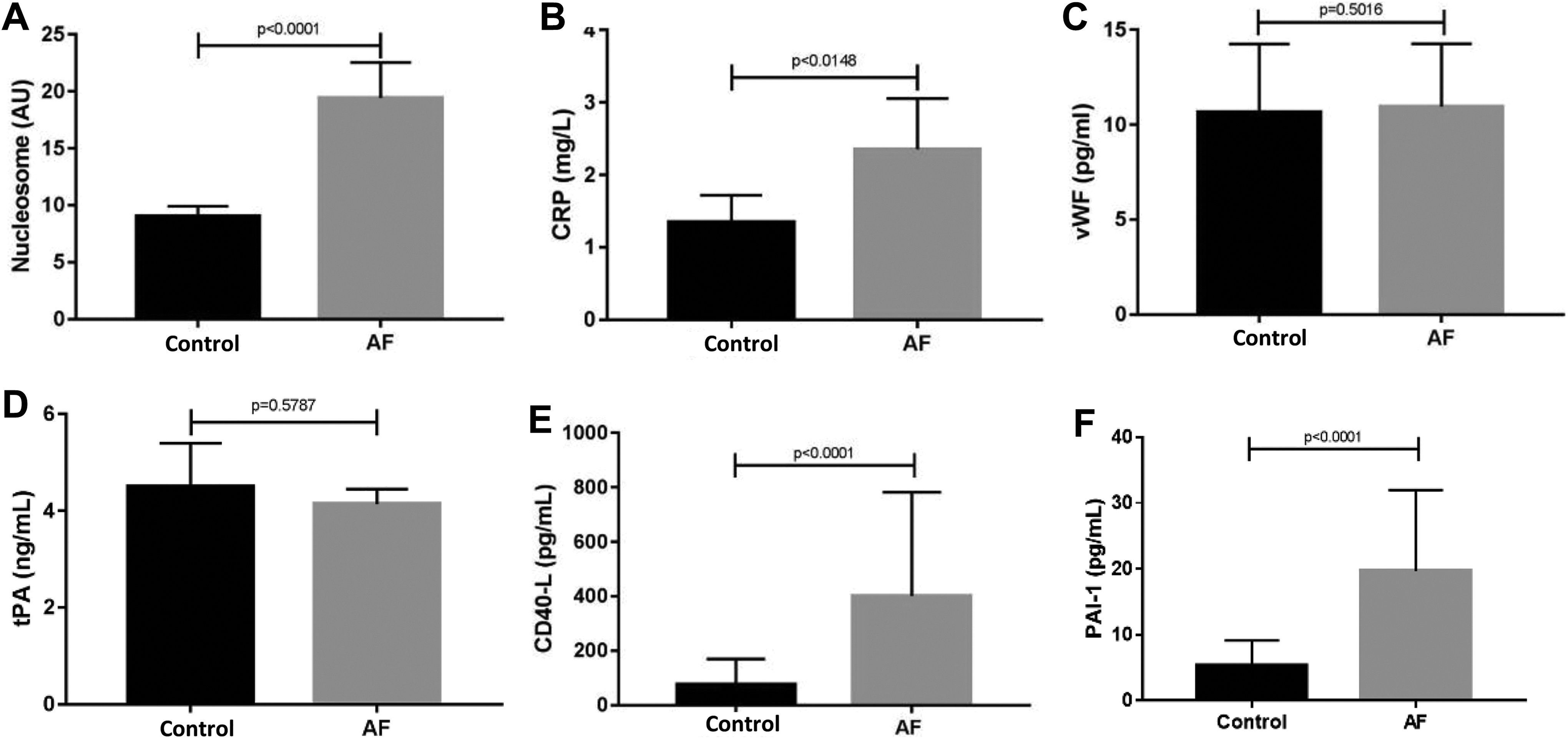
Comparison of various of inflammatory and thrombotic biomarkers in patients with AF and in healthy controls. (A) demonstrates the comparison of nucleosomes; (B) shows the comparison of CRP; (C) shows the comparison of vWF; (D) shows the comparison of tPA; (E) shows the comparison of CD40-L; and (F) shows the comparison of PAI-1. AF indicates atrial fibrillation; CD40-L, CD40-ligand; CRP, C-reactive protein; tPA, tissue plasminogen activator.
Comparison of Thrombotic Biomarkers in Controls Versus Patients With AF
As seen in Figure 2F, the plasma levels of PAI-1 were significantly elevated in the AF group (19.55 [2.17] pg/mL) when compared to the control group (5.39 [3.77] pg/mL; P < .0001). The circulating plasma levels of tPA and vWF were not statistically different between the groups (P = .58 and P = .50, respectively).
Percentage Change in all Circulating Biomarkers From the Normal Mean
The percentage change from normal mean values can be found in Figure 3. The CD40-L showed the largest percentage change from the normal mean (648 [711]). The PAI-1 showed the second largest percentage change from normal mean (265 [228]) followed by the nucleosome levels (115 [228]) and CRP (74.4 [328]). The lowest percentage change from the normal mean were the vWF levels (3.39 [31.2]).
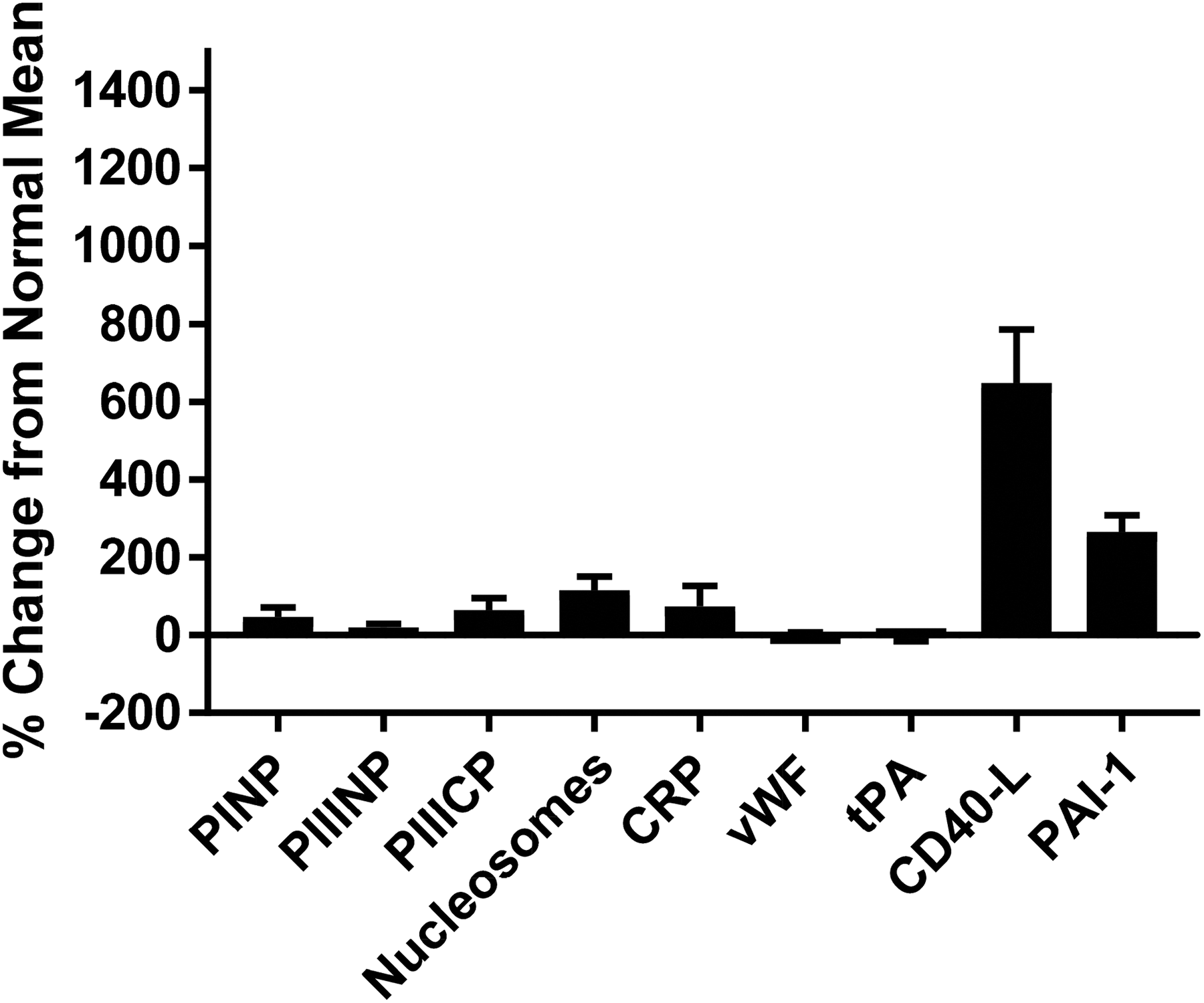
Comparison of various biomarkers percent change from normal mean ± standard error of the mean. Data is already in Table 1, no need for the figure.
Discussion
Atrial fibrillation is the most common sustained cardiac arrhythmia. As its incidence continues to increase, the population affected by AF is expected to grow, and further study of its clinical assessment and treatment is warranted. A better understanding of the pathophysiology behind AF would aid in the advancement of the management of this disease. Based on findings showing increased levels of inflammatory biomarkers in individuals with AF, inflammation is believed to play a significant role in the atrial remodeling and thromboembolic events observed in these patients. 5 Biomarkers may be useful to define the progression of inflammation, atrial remodeling, and thromboembolic events in patients with AF and could potentially serve as valuable clinical tools in the treatment of patients with AF.
In the current study, we found that the levels of peptides derived from the precursor to type III collagen were significantly elevated in the AF group compared to the control group. The increased circulating levels of both PIIINP and PIIICP may indicate that type III collagen is the predominant type of collagen present in the atrial fibrosis that occurs in AF. 22 There was no significant difference in circulating PINP levels between the AF group and the control group. The lack of difference in circulating PINP levels between the AF group and the control group was surprising, as Polyakova et al have demonstrated both PINP and PIIINP levels to be higher in the atrium of individuals with permanent AF compared to the normal population. 23 It is even more surprising that the circulating PINP levels showed no significant difference between the AF group and the control groups, considering that type I collagen is the dominant collagen in the cardiac tissue. 24 Interestingly, in Polyakova et al’s study, an increase in atrial type III collagen synthesis compared to type I collagen was noted. 23 Atrial fibrosis and the associated atrial remodeling that occurs in AF is believed to further propagate AF. If elevations in the biomarkers of collagen metabolism can be correlated with increased atrial fibrosis, then PIIINP and PIIICP are potential biomarkers that can be used to assess progression of AF. Considerations for a future study include conducting a longitudinal study using DE-MRI and/or electrophysiological mapping to monitor atrial activity while measuring levels of PIIINP and PIIICP at similar intervals.
The levels of all 3 inflammatory biomarkers measured in our study, namely, CD40-L, nucleosomes, and CRP, were significantly higher in the AF group compared to the control group. The association between inflammation and AF was first established when it was recognized that inflammatory states such as myocarditis, pericarditis, and cardiac surgeries initiated AF. 25 Although several studies have established an association between elevated inflammatory biomarkers and the presence of AF, it is not entirely clear whether inflammation is a trigger for AF or a consequence of AF. Inflammation is also thought to have an association with AF outcomes. Elevated levels of circulating inflammatory biomarkers such as CD40-L, CRP, and IL-6 have been linked to an increased risk of thromboembolic events in individuals with AF. 14 –16,26,27 With inflammation playing a role in the pathogenesis, progression, and consequences of AF, the increased levels of all the inflammatory biomarkers that were observed in the AF group were expected. It is reasonable to assume that inflammation is a possible trigger, leading to increased cell death and turnover, causing an increase in the circulating nucleosome levels seen in patients with AF. Extracellular nucleosome release and the subsequent activation of the innate immune response via DAMPs may initiate cytotoxicity of the host cell and further propagate inflammation. The interaction between CD40 and CD40-L involves platelet activation, which in turn mediates inflammation and thrombosis. 14 With increased inflammation and thrombogenesis being associated with AF, we expected the CD40-L levels in the AF group to be elevated, compared to the levels in the control group. Of all analyzed biomarkers, CD40-L was noted to have the greatest percentage change from the normal mean. Its potential as both an inflammatory and a thrombogenic biomarker would be a valuable clinical tool in the assessment of risk stratification and progression of AF.
The PAI-1 levels were significantly elevated in the AF group compared to the control group. The plasminogen activators, tPA and uPA, function in the activation of plasminogen into plasmin and consequently the dissolution of fibrin in the circulation. 19 The PAI-1 acts as an inhibitor of both tPA and uPA, leading to decreased fibrinolytic activity. The PAI-1’s role in fibrinolysis enables it to be a potential plasma marker for thromboembolic events. With AF accounting for more than 15% of all strokes in the United States, the identification of a biomarker to aid in the risk stratification of thromboembolic events in this patient population would be clinically relevant. 28 Future studies may evaluate the PAI-1 levels in patients with AF with a low risk of thromboembolic events and high risk of thromboembolic events based on their CHADS-VASc scores. Unexpectedly, there was no significant difference in the vWF and tPA antigen levels between the AF group and the control group. In our study, there was no difference in tPA antigen levels between the groups. The tPA antigen assay measures both free and complexed tPA, and increased concentration of tPA antigen is an indication of reduced fibrinolytic activity. 20 The trend toward decreased tPA antigen levels in the AF group may indicate increased fibrinolytic activity compared to the control group. Previous studies have suggested that clots that have increased tPA-induced lysability are more prone to embolization. 29 Future studies on the levels of vWF and tPA in patients with AF may benefit by using a larger cohort.
Due to the limited size of our study, considerations for future studies include using a larger population of patients with AF to compare the circulating levels of these biomarkers to the normal population. In conclusion, this study was performed as a baseline analysis of circulating biomarkers in a group of patients with AF prior to ablation procedure. The prothrombotic, inflammatory, and collagen turnover biomarkers PAI-1, CD40-L, nucleosomes, CRP, PIIICP, and PIIINP are elevated in AF. It would be interesting to correlate the levels of these biomarkers with clinical outcomes and treatment in this population.
Footnotes
Acknowledgments
The authors acknowledge the support from the cardiovascular institute, the chairs of the departments of pathology, Dr Eva Wojick, pharmacology, Dr Keith Jones, and the director of the STAR program, Dr Gail Hecht. We are also thankful to Mr Jonas Kingo of Aniara Laboratories for providing some of the kits used in this study. Special thanks to the staff of the thrombosis and hemostasis research laboratory for their support in completing this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.