
Abstract
Hemophilia causes bleeding that may affect patients’ psychological aspects and quality of life. This study aims to evaluate the impact of psychological aspects and pain on health-related quality of life (HRQoL) in adult patients with hemophilia. This cross-sectional study was conducted on 103 patients with hemophilia. Data were collected using hemophilia-specific quality of life, Depression Anxiety Stress Scales, and pain visual analogue scales. Data were analyzed using correlation coefficients, analysis of covariance, and regression analysis. The results showed that 71.7% of patients with hemophilia experienced pain on the study day. The mean score of HRQoL of patients with hemophilia was 51.09 (standard deviation = 19.37). Moreover, 57.4%, 64.6%, and 44.6% of the patients had mild to severe depression, anxiety, and stress, respectively. In addition, a significant association was observed between HRQoL and depression, anxiety, and severity of pain. In the regression model, 48% of changes in HRQOL were explained by the study variables, with the severity of pain and depression being significant predictors. Therefore, attention should be paid to these aspects to improve patients’ quality of life and psychosocial health.
Introduction
Hemophilia is a bleeding disorder resulting from deficiencies of factors VIII (A hemophilia) and IX (B hemophilia). 1 Factor deficiencies cause bleeding in joints, muscles, brain, and other internal organs, with recurrent muscular skeletal bleeds leading to severe destruction of cartilage and bones, resulting in arthropathy, disability, and impairment in quality of life. 2 –5
Health-related quality of life (HRQoL) of patients with hemophilia is not only affected by the disease but it also can be influenced by personality characteristics, such as coping, and demographic characteristics, such as living status. 6 Studies have indicated that patients with hemophilia experienced reduced HRQoL compared to healthy individuals. 7 –9 Joint pain and physical limitations are the most common factors that impair the physical domain of HRQoL. 10 Moreover, the lowest and highest scores of HRQoL of patients with hemophilia are related to physical (physical function, physical roles, and pain) and mental (social function, psychological health, and mental health) domains, respectively. 11
The high cost of treatment and negative body image as a result of arthropathy are the most common concerns in patients with hemophilia. 12 Some patients have chronic stress and, consequently, depression. 13 Patients with hemophilia experience different levels of mood and depression related to pain and disability 14 ; a higher proportion of elderly hemophiliacs with depression was reported compared to the aged-matched general population in Italy including a correlation between depression and HRQoL. 15 Researchers have also disclosed that approximately half of young adults have anxiety/depression related to pain and bleeding. 16 Another study, revealing that 43% of patients have anxiety 17 and only one-third of patients with hemophilia reported not being depressed. 14
Some factors, such as depression related to low self-esteem when compared to “normal” siblings and peers might affect HRQoL in patients with hemophilia. 18 Negative associations have been observed between HRQoL and depression with a significant relationship demonstrated between depression and physical, psychological, and social domains of HRQoL. 19
In addition to psychological factors, pain may be associated with HRQoL. 20 Due to recurrent bleeds in joints and muscles, patients with hemophilia experience a life full of pain. They experience acute, persistent, and ever present pain, which is “intense, unbelievable, terrible, annoying, and intolerable” 21 ; this pain can alter all aspects of their lives. 22
Although researchers have shown impairments in HRQoL of patients with hemophilia, these studies were performed in other countries not comparable to our country due to access to treatment in other countries being greater than in Iran. Until few years ago in Iran, fresh frozen plasma and cryoprecipitate were often used because of limited access to factor concentrates. 23 Only 1 study was performed on HRQoL of adult patients with hemophilia in Tabriz, Iran. 24 One study was conducted on depression and anxiety among children with hemophilia. 25 Review of the literature also revealed that a limited number of studies have been done on the association between HRQoL and psychological aspects of patients with hemophilia.
Therefore, the present study aims to determine HRQoL, psychological aspects (stress, depression, and anxiety), and pain as well as the association between HRQoL and the psychological aspects and pain in adult patients with hemophilia in a single treatment center in Iran.
Methods
Design
This was a cross-sectional, correlational study.
Setting and Sample
The study was conducted in a hemophilia center in Shahid Dastghaib hospital affiliated to Shiraz University of Medical Sciences (SUMS), Shiraz, Iran, from September 2015 to February 2016.
The inclusion criteria for the study were being Iranian, being aged 18 years or above, speaking Persian, and with a confirmed diagnosis of hemophilia A or B for greater than 1 year. Patients who were admitted to the hospital within the last month and those with cognitive impairment or additional congenital disorders were excluded from the study. Patients with other genetic diseases, such as thalassemia, were excluded from the study to ensure that HRQoL aspects were purely related to living with hemophilia.
Sample Size
To determine the sample size, a pilot study was performed on 10 patients with hemophilia. The findings showed that correlation coefficients between HRQoL and stress, depression, anxiety, and pain were r = 0.28, r = 0.33, r = 0.35, and r = 0.39, respectively. Therefore, based on the lowest coefficient (r = 0.28), α = 0.05, and β = 0.20, a 98-patient sample size was determined. The sample size was raised to 120 participants to allow for dropouts.
Ethical Considerations
This study was approved by the ethics committee of SUMS, Shiraz, Iran (93-01-86-8517). Written informed consent was obtained from all participants after the study objectives and procedures were explained and all questions were answered. They were also assured that participation in the study was voluntary and that they could leave the study at any time without reason and that participation/nonparticipation would not affect their care and treatment. Anonymity was taken into account, and each participant was given a study number.
Data Collection
The participants were selected using convenience sampling. One hundred and twenty questionnaires were distributed to patients, in which 110 questionnaires were returned (91.6%) and 7 questionnaires were incomplete; thus, 103 questionnaires were used for data analysis.
The study data were collected using a demographic and clinical characteristics form, as well as standardized and validated instruments, namely the hemophilia-specific quality of life (Haem-A-QoL) and Depression Anxiety Stress Scales (DASS). The demographic and clinical characteristics form assessed the patients’ age, education level, marital status, type of hemophilia, disease severity, HIV and hepatitis status, bleeding history, site of bleeding, pain experience, severity of pain (on a visual analogue scale [VAS] ranging from 0 to 10), and occupation.
Instruments
The Haem-A-QoL, which was developed by von Mackensen et al, was used to evaluate the patients’ HRQoL. 26 This questionnaire consisted of 46 items with 10 dimensions (“physical health,” “feeling,” “view of yourself,” “sports and leisure,” “work and school,” “dealing with hemophilia,” “treatment,” “future,” “family planning,” and “relationship and sexuality”). These items have to be responded on a 5-point Likert scale ranging from 1 (never) to 5 (always). The total score and the subscales scores were then transformed to a score between 0 and 100, with higher scores representing higher impairment in HRQoL. The validity of the questionnaire was approved in a study performed on 233 patients with hemophilia in Italy. 27 Its excellent reliability and discriminant validity have also been confirmed in patients with hemophilia from other countries. 28 –30 The Haem-A-QoL has been translated into more than 60 languages. 31
In order to linguistically and psychometrically validate the Haem-A-QoL for Persian, a person who had master degree of English language translation and was familiar with health professions forward translated the original questionnaire from English to Persian. This translated version was then reviewed by the researcher (the first author), and all problematic items were discussed and clarified. Then, the Persian questionnaire was back-translated into English by an Iranian individual who had lived in Europe for 10 years. Afterward, it was assessed by the developer of the questionnaire (Dr von Mackensen), and modifications were implemented until all items were approved by Dr von Mackensen. After that in a cognitive interview session, 10 adult Iranian patients with hemophilia assessed and approved the items regarding simplicity, clarity, and easiness to understand. They were also asked to formulate each item in their own words. This helped the researchers to determine whether the participants understood the items and whether their interpretations of each item were in the right direction. The content validity of the questionnaire was approved by 10 faculty members of universities of medical sciences.
Depression Anxiety Stress Scales was designed by Lovibond and Lovibond in 1995. Depression Anxiety Stress Scales consisted of 21 items responded through a 4-point Likert scale (0 = never, 1 = sometimes, 2 = often, and 3 = almost always). The scores of stress, depression, and anxiety were classified as normal, mild, moderate, severe, and extremely severe. 32 Scores for normal levels of stress, depression, and anxiety are 0-14, 0-9, and 0-7, respectively; abnormal scores are (respectively) as follows: mild: 15-18, 10-13, and 8-9; moderate: 19-25, 14-20, and 10-14; severe: 26-33, 21-27, and 15-19; and extremely severe: 34+, 28, and 20+. The construct validity of DASS was approved by Szabo in a sample of young adolescents. 33 Moreover, Sinclair et al assessed the psychometric properties of this scale in 503 adults in United States and reported Cronbach α coefficients of 0.84, 0.91, and 0.80 for stress, depression, and anxiety, respectively. 34 The reliability and validity of the scale were also confirmed in Iranian population and patients with asthma. Accordingly, Cronbach α was 0.93 for the total scale and 0.86, 0.81, and 0.80 for stress, depression, and anxiety, respectively. 35,36
Data Analysis
The data were analyzed using the SPSS statistical software, version 16. The Haem-A-QoL was psychometrically tested regarding reliability (internal consistency, test–retest reliability) and validity (convergent, known groups). Convergent validity was tested correlating the Haem-A-QoL with domains of the DASS and pain intensity. Spearmen and Pearson coefficient tests were used according to the distribution. Known groups’ validity was tested related to depression and anxiety comparing subgroups of patients with “no/mild” and patients with “moderate/severe/extremely sever” symptoms. Descriptive statistics included frequency, mean, and standard deviation (SD) of clinical and demographic data and psychological aspects. At first, normality of the data was confirmed by Kolmogorov-Smirnov test. Since there were associations between pain intensity and HRQoL (r = 0.47, P < .0001), stress (r = 0.21, P = .04), depression (r = 0.26, P = .01), and anxiety (r = 0.30, P = .004), analysis of covariance (ANCOVA) model was used to assess the association between HRQoL and the psychological aspects, in which pain intensity was considered as the covariant. Multiple regression analysis was used to predict HRQoL in patients with hemophilia.
Results
Demographic and Clinical Characteristics
Data from 103 eligible patients with hemophilia with the mean age of 29.40 years (SD = 9.02) were analyzed. Forty-seven percent of the patients had secondary and high school education levels and 52% were single, and most patients were self-employed (Table 1).
Demographic and Clinical Characteristics of Patients With Hemophilia.
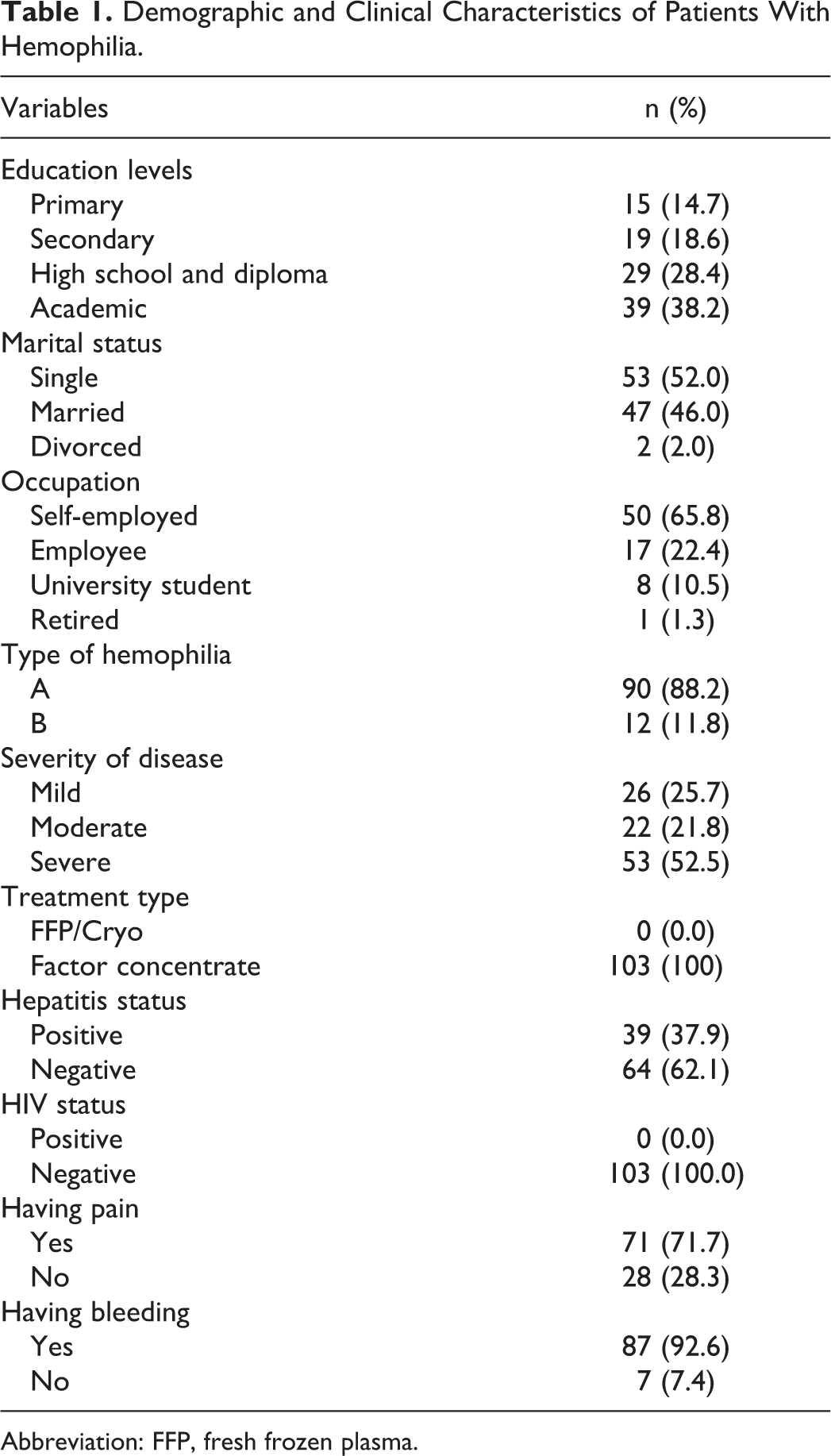
Abbreviation: FFP, fresh frozen plasma.
About 52.5% of the participants had severe hemophilia and 37.9% had hepatitis. However, no one had HIV. The incidence of bleeding was 92.6% in the last 6 months (Table 1). From the 103 participants, 87 reported to have had bleeds over the last 6 months (84.5%); overall, patients bleeds were reported mainly in joints (n = 100) and mucosal membrane (n = 42), and 14 bleeds were reported in muscle/soft tissue. Hemarthrosis, epistaxis, and bleeds in mouth, urinary, and gastrointestinal systems and in muscles were the most common bleeding. All patients used factor concentrates to treat their bleeding. Indeed, 71.7% of the patients with hemophilia experienced pain on the study day. The mean score of pain intensity was 4.43 (SD = 1.61), and maximum values in this cohort ranged from 0.0 to 6.0 (possible range 0-10).
Psychometric Characteristics of Haem-A-QoL and DASS in the Persian Hemophilia Cohort
The Haem-A-QoL questionnaire had good internal consistency; Cronbach's α coefficients of the whole questionnaire and all its subscales were α > 0.7, except for the dimension “view of yourself” which was α = 0.47, and were comparable to the original validation study in an Italian cohort. Test–retest reliability of the questionnaire in a smaller cohort (r = 0.85) was good (Table 2). Known groups’ validity demonstrated that with pain intensity as a covariant, patients with lower levels (“no/mild”) of depression (Figure 1) and anxiety (Figure 2) reported better HRQoL compared to patients with “moderate/severe or extremely severe” levels. This difference was significant in almost all dimensions of the Haem-A-QoL for anxiety and depression.
Psychometric Characteristics of the Haem-A-QoL in Persian Patients With Hemophilia Compared to the Original Italian Cohort [25].
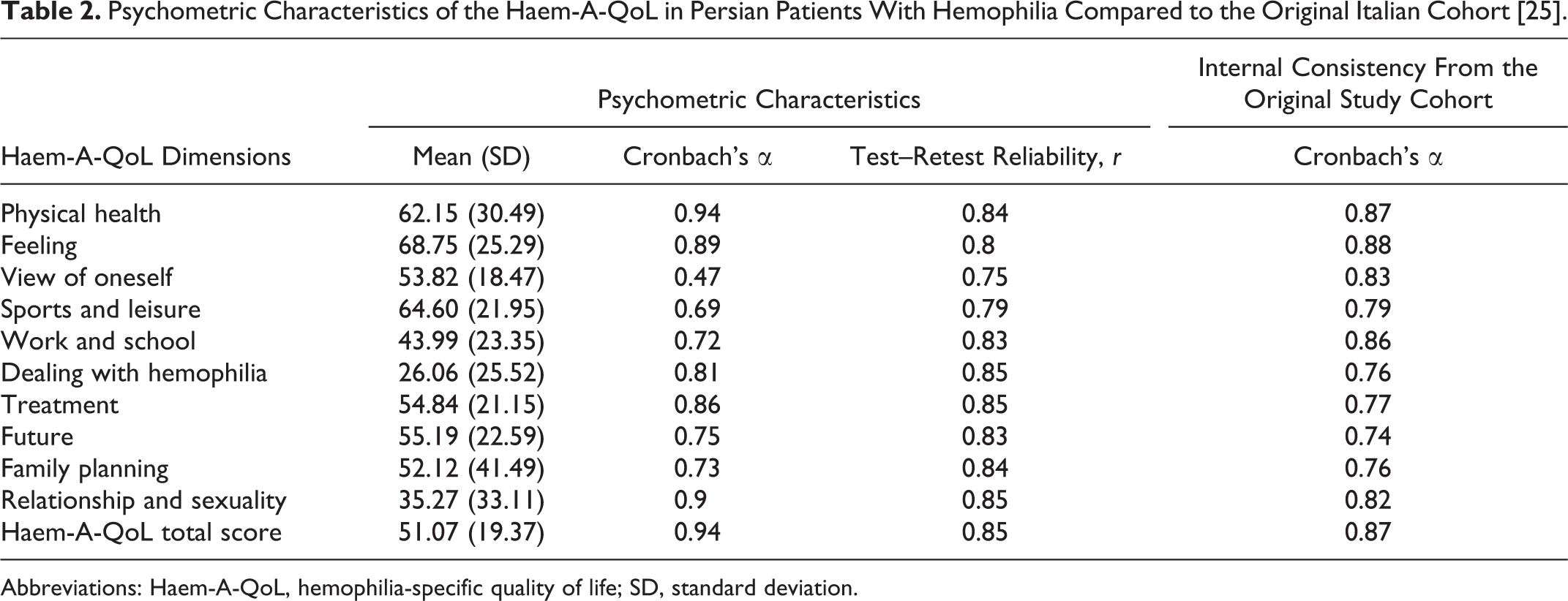
Abbreviations: Haem-A-QoL, hemophilia-specific quality of life; SD, standard deviation.
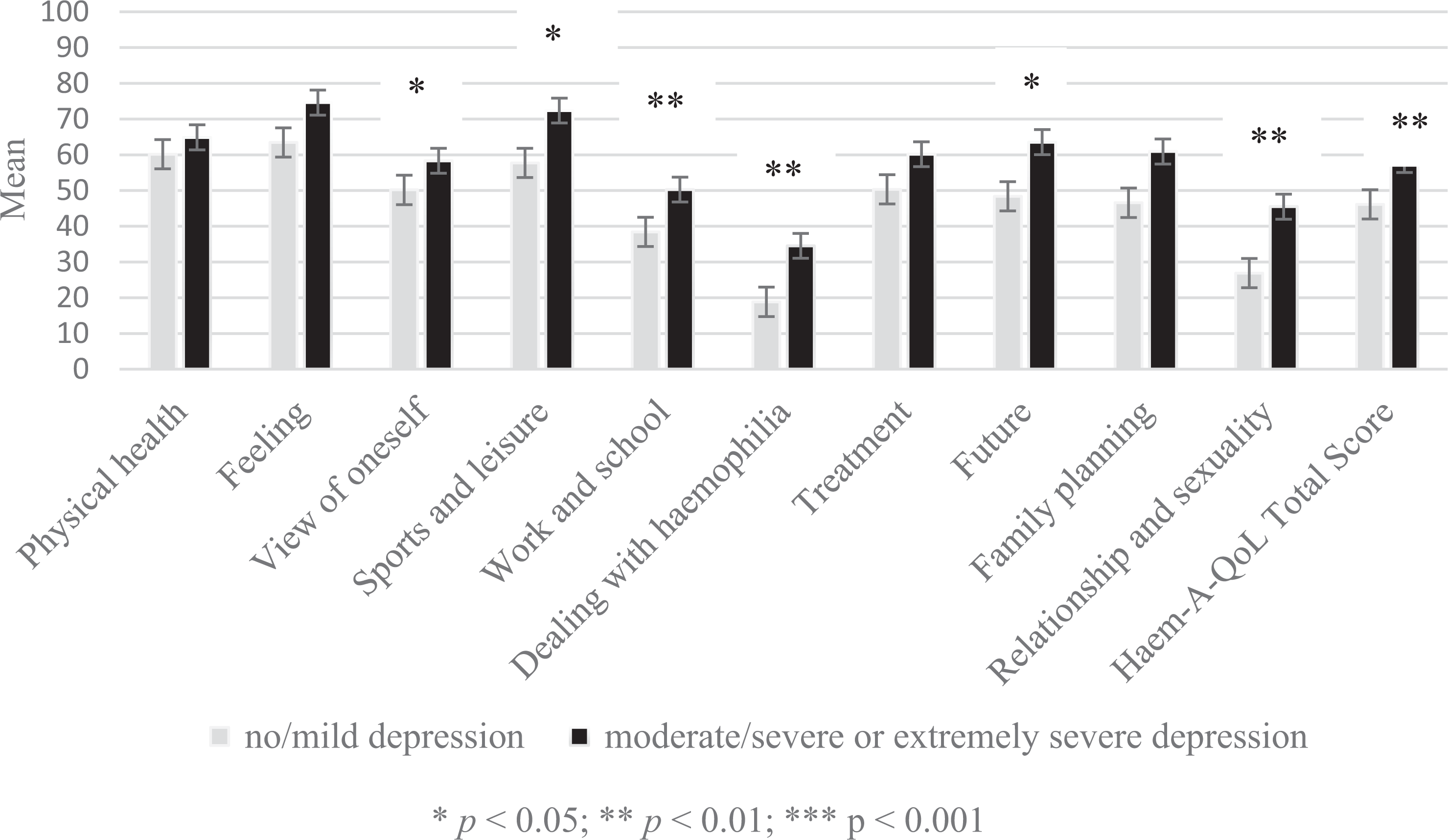
Differences in quality of life (Haem-A-QoL) regarding depression.
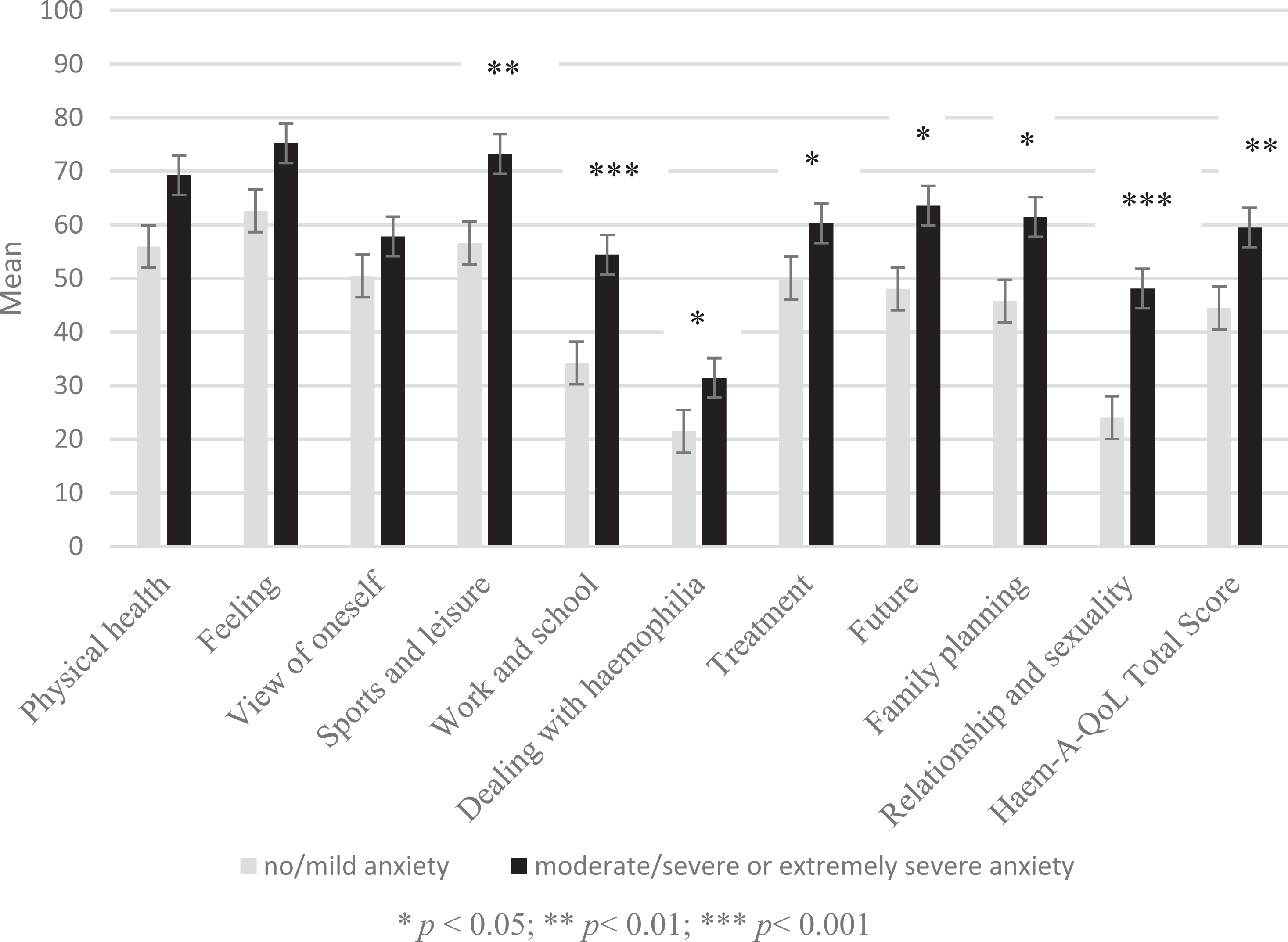
Differences in quality of life (Haem-A-QoL) regarding anxiety.
In the present study, the test–retest reliability of the DASS was r = 0.80, and its Cronbach's α was 0.90. Indeed, Cronbach's α coefficients of 0.85, 0.87, and 0.82 were obtained for stress, depression, and anxiety, respectively.
Health-Related Quality of Life
The total mean score of HRQoL of patients with hemophilia in the Haem-A-QoL was 51.09 (SD = 19.37). The highest impairments were found in the dimensions “feeling” (mean = 68.75 [SD = 25.29]), “sports and leisure” (mean = 64.60 [SD = 21.95]), and “physical health” (mean = 62.15 [SD = 30.49]). On the other hand, the best scores in HRQoL were related to “dealing” with hemophilia (mean = 26.06 [SD = 25.52]) and “relationship and sexuality” (mean = 35.27 [SD = 33.11]), which indicated the lowest impairment in these domains (Table 2).
Psychological Aspects
The results of this study showed that most patients with hemophilia (n = 56) experience normal levels of stress in the DASS (55.4%). Nonetheless, almost half of the patients have a moderate to extremely severe form of depression (47.5%) and anxiety (48.5%).
The Association Between Quality of Life and Psychological Aspects
The results of ANCOVA indicated a significant association between HRQoL (Haem-A-QoL total score) and the psychological aspects in patients with hemophilia in terms of depression (F = 3.05, P = .001), anxiety (F = 1.84, P = .04), and pain intensity (r = 0.47, P < .0001). However, no significant association was found between HRQoL and stress (F = 1.74, P = .05). Furthermore, the results of ANCOVA model showed that some subscales of HRQoL were also associated with depression and anxiety (Table 3).
The Association Between Health-Related Quality of Life (Haem-A-QoL) and Psychological Aspects and Pain Severity in Patients With Hemophilia.
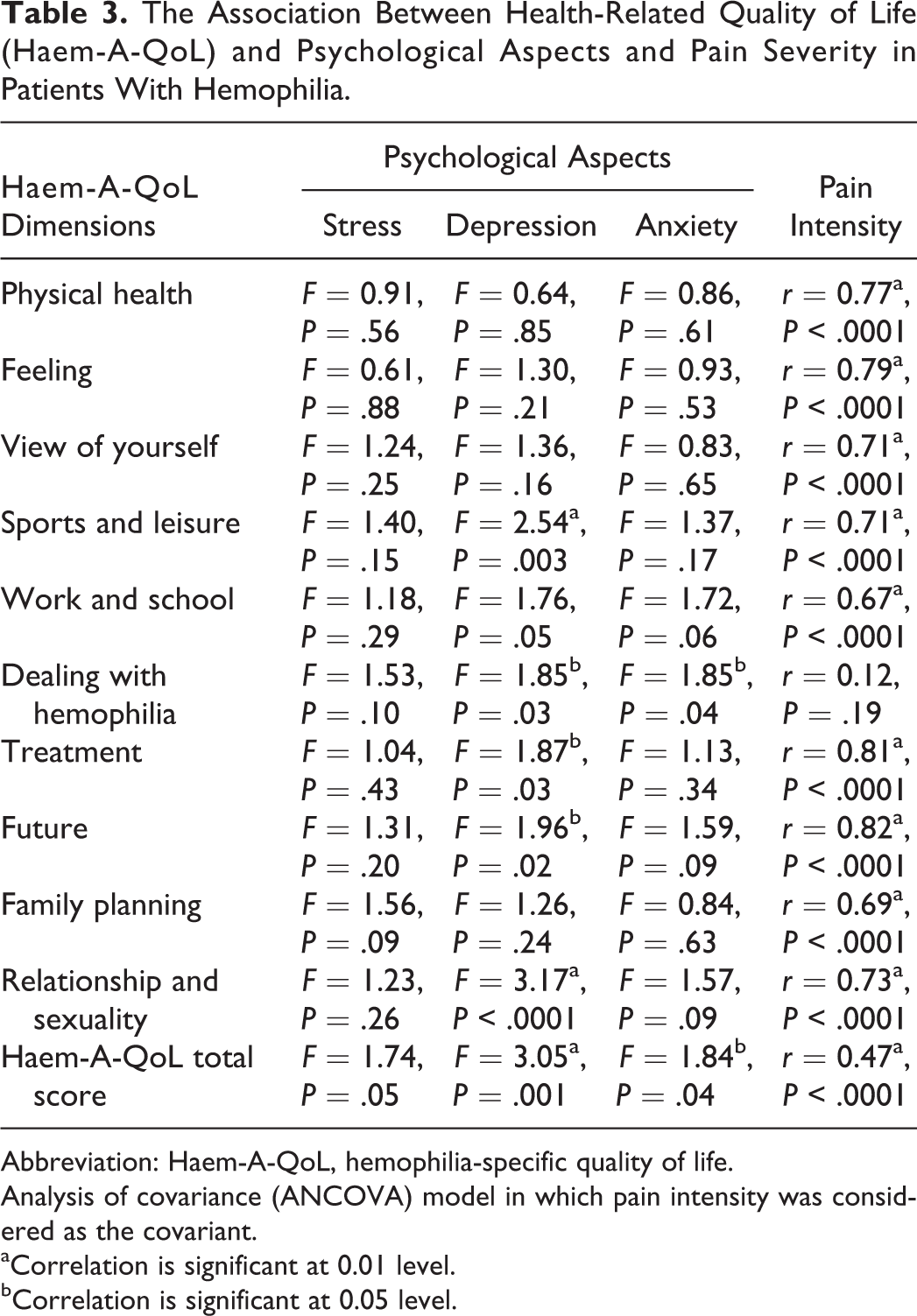
Abbreviation: Haem-A-QoL, hemophilia-specific quality of life.
Analysis of covariance (ANCOVA) model in which pain intensity was considered as the covariant.
aCorrelation is significant at 0.01 level.
bCorrelation is significant at 0.05 level.
In this study, multiple regression analysis was used to determine the contribution of variables to explain the variance of HRQoL in patients with hemophilia. Based on our findings, hepatitis status, severity of disease, stress, depression, anxiety, severity of pain, and having bleeding were included in this analysis. Forty-seven percent of the variance in HRQoL could be predicted by severity of pain and depression (Table 4). In addition, the results of linear regression analysis showed a correlation coefficient of 0.69 between HRQoL and the psychological variables.
The Predictors of Quality of Life (Haem-A-QoL) in Patients With Hemophilia (The Results of Multiple Regression Analysis).
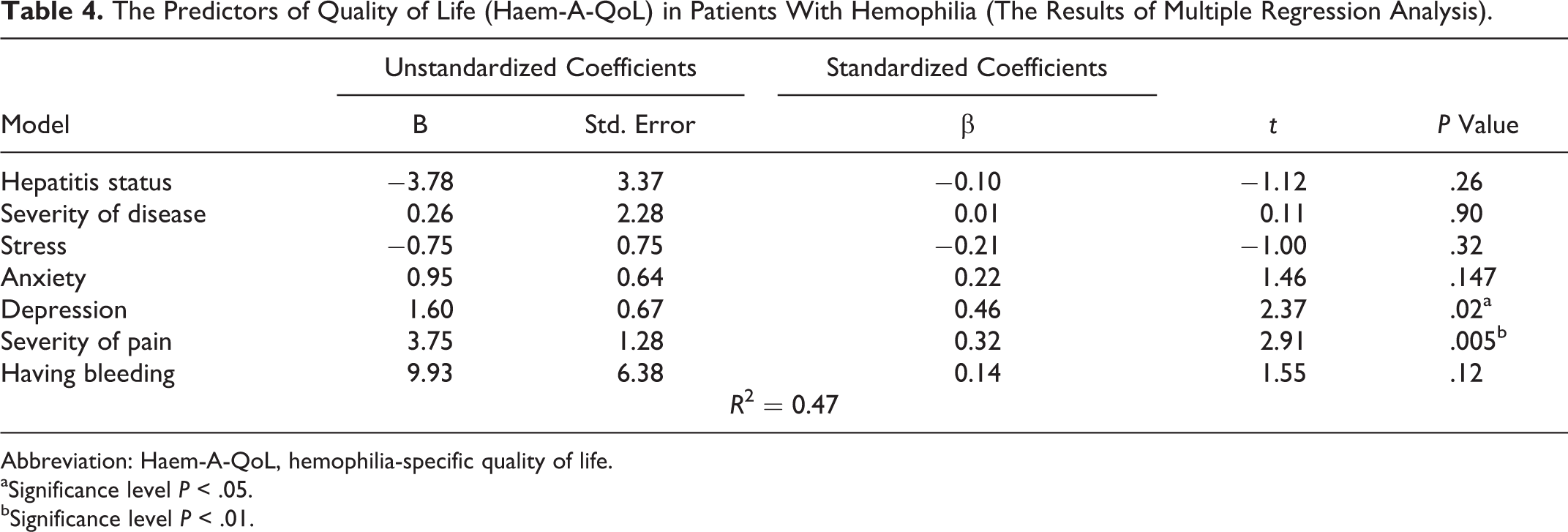
Abbreviation: Haem-A-QoL, hemophilia-specific quality of life.
aSignificance level P < .05.
bSignificance level P < .01.
Discussion
The current study results indicated that 71.7% of patients with hemophilia had pain on the VAS (possible range 0-10) with a mean score of pain intensity of 4.43 (SD = 1.61). This is much higher compared to only 35% of adults with hemophilia in a European pain study using the VAS (possible range 0 = no pain to 10 = worst pain possible) or the numeric rating scale or verbal rating scale (possible range 0 = no pain to 10 = pain as bad as it could be). 37 Curtis et al revealed that the rate of joint arthritis pain was 33.3% in the US young adult patients with hemophilia determined by self-reports using a 5-point scale (possible range 1 = no pain to 5 = severe pain all the time). 38 Additionally, approximately 20% of children and adolescents with bleeding disorders in both hemophilia centers in Shiraz, Iran, and Great Ormond Street Hospital for Children NHS Foundation Trust (GOSH) in London reported pain in the Wong-Baker Faces Pain Rating Scale (possible range 0 = does not hurt at all to 10 = hurts as much as you can imagine). The mean scores of pain intensity were 8.23 and 5.14 in Shiraz and GOSH, respectively. A larger number of adolescents had pain in comparison with children. 39 This implies that the frequency of pain rises by age and increasing joint disease following recurrent bleeding; therefore, a higher incidence of pain is expected among adults.
This study showed that the patients with severe pain had more stress, anxiety, and depression or the patients with highest level of stress, anxiety, and depression might experience pain with highest intensity. Similar to this study, it was reported that certain factors such as stress and anxiety effect the pain experience. 40 In another study, headache and back and shoulder pain were associated with current anxiety disorders. 41 When pain becomes chronic, distress, anger, and depression occur. 42
In the present study, 37.9% of patients with hemophilia had hepatitis. Curtis et al also reported that liver diseases and hepatitis affected 48% of young adult patients with hemophilia. 38
In this study, joints, nose, mouth, urinary and gastrointestinal systems, and muscles were the most common sites of bleeding. Similar to our finding, Dorgalaleh et al reported that the most common clinical symptoms of hemophilia were hemarthrosis, epistaxis, ecchymosis, and postdental extraction. 23
In our study, the mean score of HRQoL was 51.07 (SD = 19.37) among adult patients with hemophilia. Similarly, Mercan et al performed a study in Turkey as a developing country and indicated that the mean score of their patients’ HRQoL was 47.4 (SD = 14.2). 43 However, Brazilian and Greek patients with hemophilia had better QoL scores in the Haem-A-QoL. 29,44 von Mackensen et al also reported that the mean score of their patients’ HRQoL was 31.1 (12.0). 28 Moreover, another study showed that the scores of the physical component of HRQoL using the SF-12 were lower compared to national norms. 38 Chronic diseases, such as hemophilia, are a part of patients’ daily life 19 that impacts their psychological well-being as well. 45
The findings of the current study indicated that the domains with the highest impairments in HRQoL in patients with hemophilia were “sports and leisure,” “feeling,” and “physical health.” These findings were similar to those obtained by Ferreira et al and Mercan et al. 29,43 In another study on patients with hemophilia, the best and worst dimensions of HRQoL were “sexuality” and “sports and leisure,” respectively. 44 Varaklioti et al also reported that patients with hemophilia had impairment in their HRQoL specially in the physical heath domain and they could not perform some activities and sports. 46 In our study, patients had problems with “sports and leisure.” By increasing these patients’ access to factor, previous attempts prohibiting exercise have been excluded and more efforts are needed to encourage patients to exercise. 47 This not only has physical benefits but also helps patients participate in social activities. 48,49
The present study results demonstrated that 44.6%, 57.4%, and 64.4% of the patients with hemophilia experienced mild to extremely severe levels of stress, depression, and anxiety, respectively. Consistently, Hassan et al carried out a study on Egyptian adolescent patients with hemophilia and indicated that 68% of the patients had mild to severe depression. 14 On the other hand, the incidence of depression was less than 37% in other studies. 50,51 Researchers in developing countries whose backgrounds are roughly similar to those of Iran demonstrate that patients deal with more complications, such as disability and chronic pain than patients in developed countries. These complications lead to fear and uncertainty, resulting in depression and other psychological problems. 14
The findings of our study revealed that patients with severe pain had lower HRQoL and that the intensity of pain was one of the predictors of HRQoL. In the same line, it was reported that pain was associated with lower HRQoL. 20 Moreover, Elander et al revealed an association between physical HRQoL and disease severity, pain, and pain acceptance. They believed that pain acceptance affected psychological HRQoL as well. 52 Researchers have also demonstrated an association between chronic pain and physical, psychological, social, and environmental health in patients with hemophilia. A significant association was also reported between pain and severity of the disease. 39 Pain altered physical health by impairing physical function, changing body physics, and disturbing sleep quality. Pain led to psychological problems by increasing psychological distress, it also impaired social relationships by changing relationships and decreasing social activities. 22 Therefore, all aspects of HRQoL are affected by pain.
According to the present study findings, patients with lower levels of stress, depression, and anxiety had better HRQoL. Forty-seven percent of the variance in HRQoL could be explained by the predictors’ severity of pain and depression. Some studies of patients with hemophilia have indicated a significant association between depression and HRQoL. 15,19,45 Al-Gamal et al also mentioned that HRQoL was related to depression and anxiety, and they reported that patients with chronic diseases experienced more psychological tension in their lives that led to impairment in their life quality. 53
A limitation of this study was that it was performed only in a single center; thus, further multicenter studies (with larger sample sizes) are recommended to allow generalization of the results.
Implication for Practice
Considering high levels of stress, depression, and anxiety and impairment in HRQoL in patients with hemophilia, attention should be paid to psychological aspects of patients in order to improve their quality of life. Conducting other qualitative studies on HRQoL of patients with bleeding disorders is also suggested. Furthermore, performing an intervention to reduce stress, anxiety, and depression and improve HRQoL in patients with hemophilia would be effective.
Conclusion
The findings of this study demonstrated that almost three-quarter of the patients with hemophilia experienced pain on the study day and roughly half of patients with hemophilia had mild to extremely severe stress, depression, and anxiety. Highest impairments in HRQoL were found in the dimensions “feeling,” “sports and leisure,” and “physical health” of the Haem-A-QoL. Moreover, patients with better HRQoL had lower levels of depression, anxiety, and pain intensity. Severity of pain and moderate to severe levels of depression were predictors of HRQoL in these patients with hemophilia. Therefore, health-care providers are suggested to improve HRQoL of patients with hemophilia by reducing psychological problems and pain intensity. Inclusion of psychology services within the multidisciplinary hemophilia team would appear to enhance patients’ psychosocial health and outcomes.
Footnotes
Authors’ Note
The study was designed by M.R., S.vM., F.S., Z.M., and K.K. Data were collected and analyzed by M.R. Backward and forward translation of Haem-A-QoL questionnaire and evaluation of validity and reliability of its Persian version were performed by M.R. and S.vM. The data were analyzed by M.R. and F.S. The manuscript was written by M.R., S.vM., F.S., Z.M., and K.K. The early draft of the article was reviewed and the final version was approved by all authors.
Acknowledgments
Hereby, the authors would like to thank the personnel of the hemophilia center in Shahid Dastgheib hospital affiliated to SUMS. They would also like to thank Mr Enayati for data collection. They are also thankful for all the participants who took part in this research. Last but not least, Ms A. Keivanshekouh at the Research Improvement Center of SUMS is appreciated for improving the use of English in the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved and financially supported by SUMS, Iran (Grant Number. 93-01-86-8517).