
Abstract
Methylenetetrahydrofolate reductase (MTHFR) gene polymorphism (C677T)] is a well-recognized genetic risk factor for venous thrombosis; however, its association with arterial thrombosis is still under debate. Herein, we evaluated the prevalence of MTHFR C677T polymorphism in Georgian patients in comparison with healthy individuals and its association with arterial thrombosis. We enrolled 214 participants: 101 with arterial thrombosis (71.3% males; mean age: 66.3 ± 12.1 years) and 113 controls (67.3% males; mean age: 56.6 ± 11.3 years). Genomic DNA was extracted from dry blood spot on Whatman filter paper. Polymerase chain reaction was performed to determine MTHFR C677T polymorphism. Frequency of C677T allele polymorphism in controls was 21.2%, which corresponded to heterozygous and homozygous stage frequencies of 35.4% and 3.5%, respectively. In patient group, an allelic frequency of 33.2% was found, which corresponded to the presence of 48.5% of heterozygous and 8.9% of homozygous individuals. Comparing the frequency of mutated alleles between the 2 groups, a significantly high frequency of mutated alleles was found in patient group (P < .05). In conclusion, high frequency of MTHFR C677T polymorphism found in arterial thrombosis patient group suggests that this polymorphism might increase the risk of arterial thrombosis in Georgian patients.
Keywords
Introduction
Interactions of predisposing genetic polymorphisms and acquired risk factors often result in thrombosis, a leading cause of cardiovascular and hematologic events. Homocysteine is a molecule produced by the breakage of methionine, and this pathway is dependent on vitamins B6 and B12 and folate. 5-Methylenetetrahydrofolate is the main form of folate in plasma that participates in the remethylation process, which is formed from the reduction of 5,10-methylenetetrahydrofolate by the enzyme methylenetetrahydrofolate reductase (MTHFR). In this process, homocysteine receives a methyl group by the activity of the enzyme methionine synthase (MTR). Methionine synthase reductase (MTRR) is involved in reducing cob(II)alamin (B12r) to methylcobalamin, the cofactor form used in MTR. 1,2
The MTHFR and MTRR enzymes are responsible for keeping homocysteine at normal levels. Genetic variations in the genes encoding these enzymes modulate homocysteine plasma levels. 3 According to the peer-reviewed literature, the common polymorphism c.677C>T in the MTHFR gene results in the conversion of the amino acid “alanine” to a “valine” at position 226 of the protein. 4 Based on our recent findings, the presence of this polymorphism is related to lower enzyme activity, higher plasma concentrations of homocysteine, and lower plasma concentrations of folic acid. 5 Individuals showing the TT genotype presented 20% higher homocysteine levels than those with the common CC genotype. 5
Studies have demonstrated an association between hyperhomocysteinemia and the development of cardiovascular diseases, thereby implicating that it is a risk factor for atherosclerosis and thrombosis. 6 Furthermore, there is evidence that high plasma homocysteine levels are associated with an increased risk of developing peripheral arterial disease (PAD) 7,8 ; however, its causal relationship is not fully understood yet.
Given the ambiguous relationship between the MTHFR C677T and arterial thrombosis, and the lack of sufficient information about the prevalence of this polymorphism in the Georgian population, in this study we sought to evaluate the prevalence of the MTHFR C677T polymorphism in a Georgian cohort of patients alongside the healthy individuals and its potential association with arterial thrombosis.
Materials and Methods
Participants
We enrolled 101 arterial thrombosis patients (71.3% males; mean age: 66.3 ± 12.1 years), 83% with myocardial infarction (MI) and 13% with ischemic stroke, with a comparative group of 113 healthy control participants (67.3% males; mean age: 56.6 ± 11.3 years). The mean age of the first MI and ischemic stroke was 62.6 ± 12.6 years and 71.5 ± 11.7 years, respectively. Notably, 12 patients with MI experienced recurrent MI episodes. Standard troponin measurements and computed tomography scans were used for the diagnosis of patients with MI and ischemic stroke.
From all the participants, dry blood samples were collected at the Heart Disease Department and Medical Ward of Batumi Hospital, Government of Autonomous Republic of Adjara, Georgia. The specimens were subsequently processed at the Faculty of Pharmacy, University of Porto, Portugal. All participants gave their written informed consent for participation in this study, which has been duly approved by the ethics committee from the “Unimed Adjara” (Adjara, Georgia, Ltd).
DNA Extraction
The genomic DNA was extracted from all the participants’ dry blood spots on Whatman filter papers according to the instructions from the KAPA Express Extract Kit (Kapa Biosystems, Wilmington, Massachusetts ). The DNA samples thus obtained were stored at −20°C until further use.
Polymerase Chain Reaction
The polymerase chain reaction (PCR) was performed to determine the polymorphisms of the MTHFR (C677T) gene as described previously. 9 To discriminate the single base changes between the normal (N) and mutated (M) alleles, 2 reverse primers (normal: 5′-AAGGAGAAGGTGTCTGCGGGCGC-3′ and the mutated: 5′-AAGGAGAAGGTGTCTGCGGGCGT-3′) were utilized, and these were paired with a common forward primer (5′-AAGATCCCGGGGACGATGGGG-3′). The PCR reaction was performed with an initial denaturation of 95°C for 3 minutes, followed by 39 cycles of 95°C for 30 seconds, 67°C (annealing temperature) for 30 seconds, and 72°C for 1 minute, and a final extension at 72°C for 5 minutes was also performed. Primers for the human factor IX (FIX) gene, used as an internal control, were FIX-forward 5′-CTCCTGCAGCATTGAGGGAGATGGACATT-3′ and FIX-reverse 5′-CTCGAATTCGGCAAGCATACTCAATGTAT-3′. The amplification products were analyzed by electrophoresis on a 2% agarose gel with ethidium bromide for visualization (Figure 1).
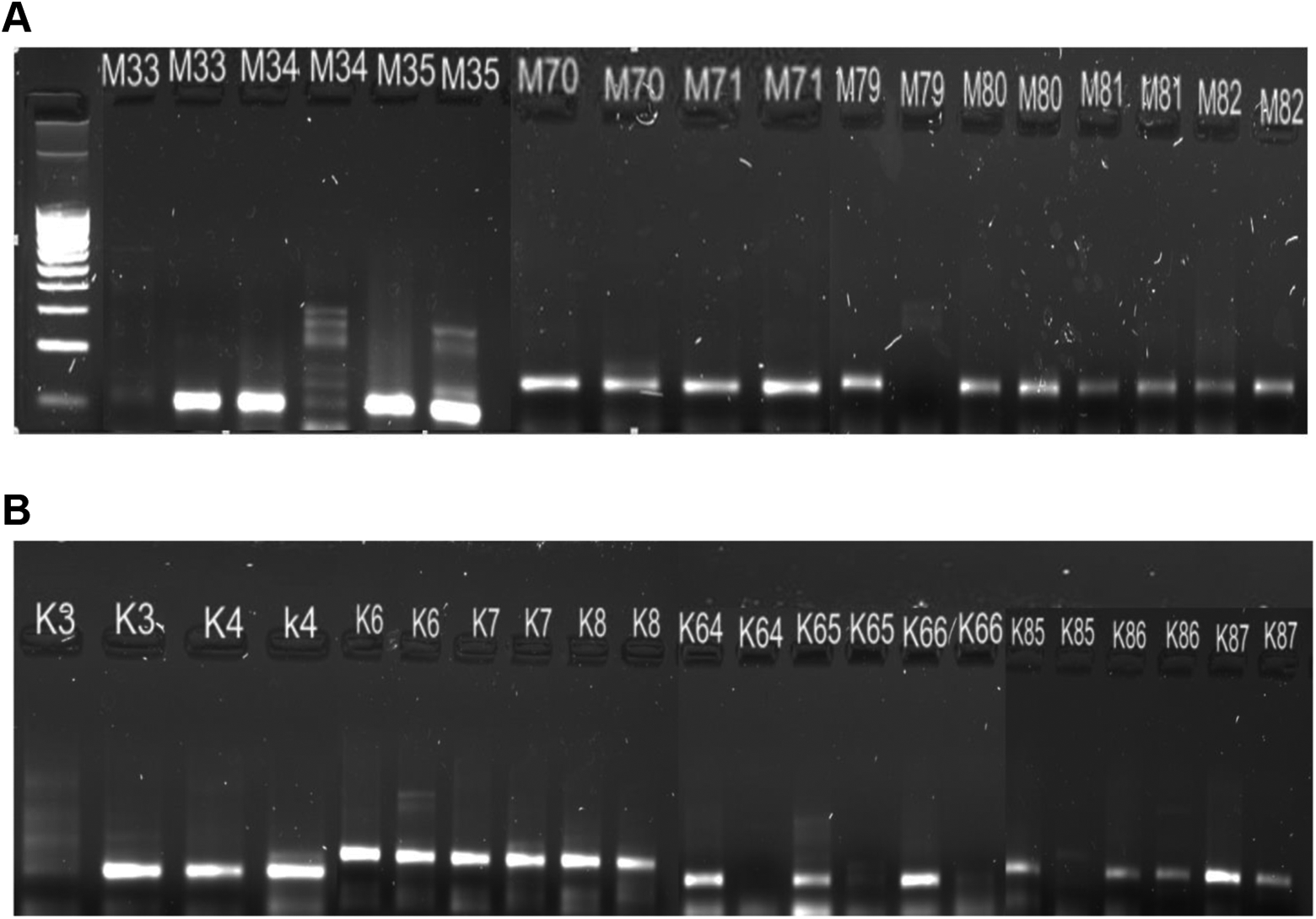
The MTHFR C677T gene fragment in gel electrophoresis for dominant homozygous (CC), heterozygous (CT), and recessive homozygous mutated (TT) in patients (A): M33-TT genotype, M34-CC genotype, M35-CT genotype, M70-71: CT genotype, M79-CC genotype, M80-81-82: CT genotype; and in control group (B): K3-TT genotype, K4-6-7-8: CT genotype, K64-65-66-85: CC genotype, K86-87: CT genotype.
Statistical Analyses
The statistical analyses of the data were performed using the Statistical Package for Social Sciences (SPSS, version 21.0) for Windows (SPSS Inc, Armonk, New York ). All the data are presented as proportions, and the association between the categorical variables was analyzed using the χ2 or the Fisher exact test. The Hardy-Weinberg equilibrium of the MTHFR C677T polymorphism was evaluated in the control and patient groups using the web tool available at www.oege.org/software/hardy-weinberg.html. The statistical significance was declared at P < .05 level.
Results
Figure 1A shows the MTHFR C677T gene fragment in gel electrophoresis for dominant homozygous (CC), heterozygous (CT), and recessive homozygous-mutated (TT) in the patients (M33-TT genotype, M34-CC genotype, M35-CT genotype, M70-71: CT genotype, M79-CC genotype, M80-81-82: CT genotype). Figure 1B shows the pattern of agarose gel electrophoresis in the control group (K3-TT genotype, K4-6-7-8: CT genotype, K64-65-66-85: CC genotype, K86-87: CT genotype).
Table 1 summarizes the data on the MTHFR C677T genotype and allelic frequencies of the patient and control groups. We found that the frequency of the C677T allele polymorphism in the control group was 21.2%, which corresponded to the heterozygous and homozygous stage frequencies of 35.4% and 3.5%, respectively. In the patient group, an allelic frequency of 33.2% was found, which corresponded to the presence of 48.5% of heterozygous individuals and 8.9% of homozygous individuals (Figures 2 and 3). The MTHFR C677T polymorphism was in the Hardy-Weinberg equilibrium in both groups of participants.
Genotype and Allelic Frequencies of C677T of Methylenetetrahydrofolate Reductase (MTHFR) in the Control and Patients With Arterial Thrombosis Groups.
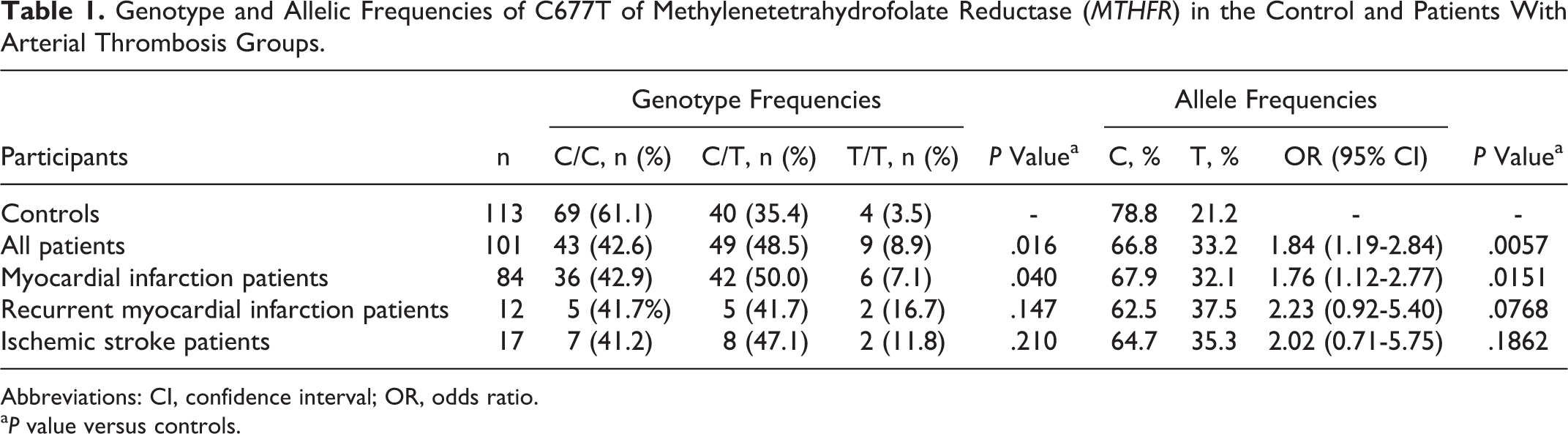
Abbreviations: CI, confidence interval; OR, odds ratio.
a P value versus controls.
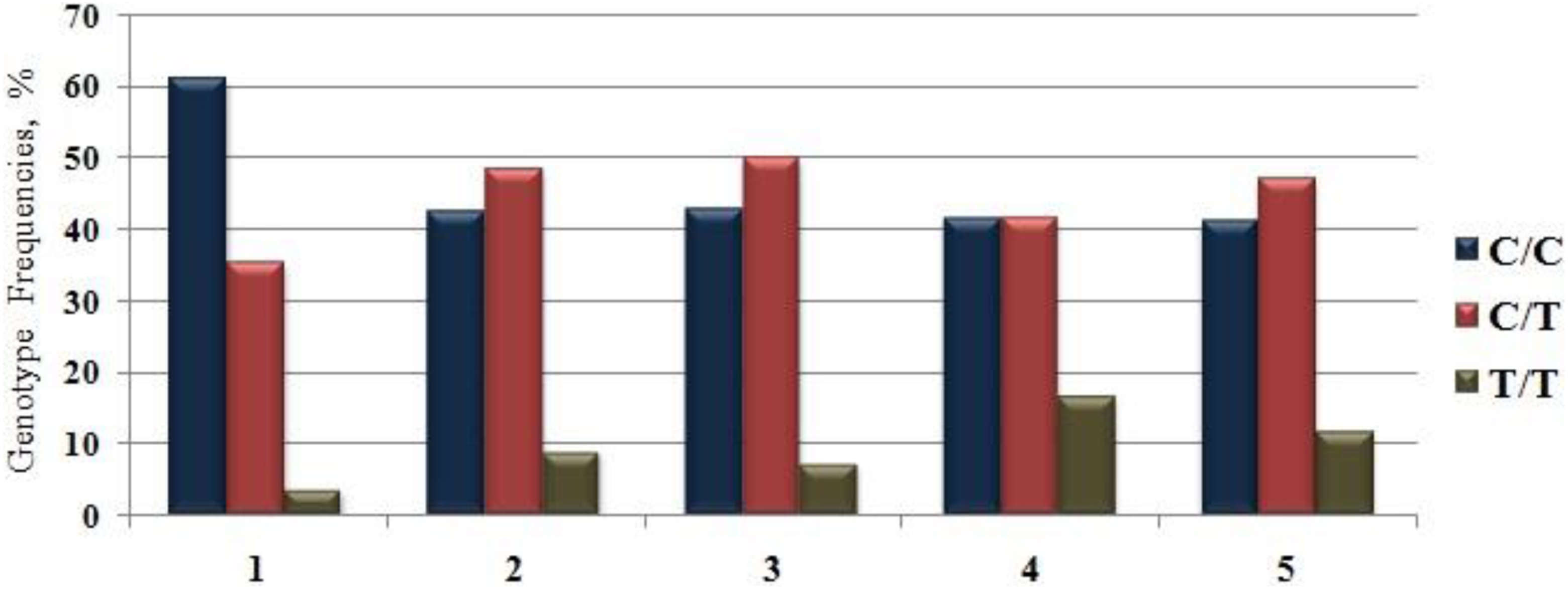
Genotype (C/C, C/T, T/T) frequencies of C677T of MTHFR in the control and patients with arterial thrombosis groups: 1 (controls; n = 113), 2 (all patients; n = 101), 3 (myocardial infarction patients; n = 84), 4 (recurrent myocardial infarction patients; n = 12), and 5 (ischemic stroke patients; n = 17) groups.
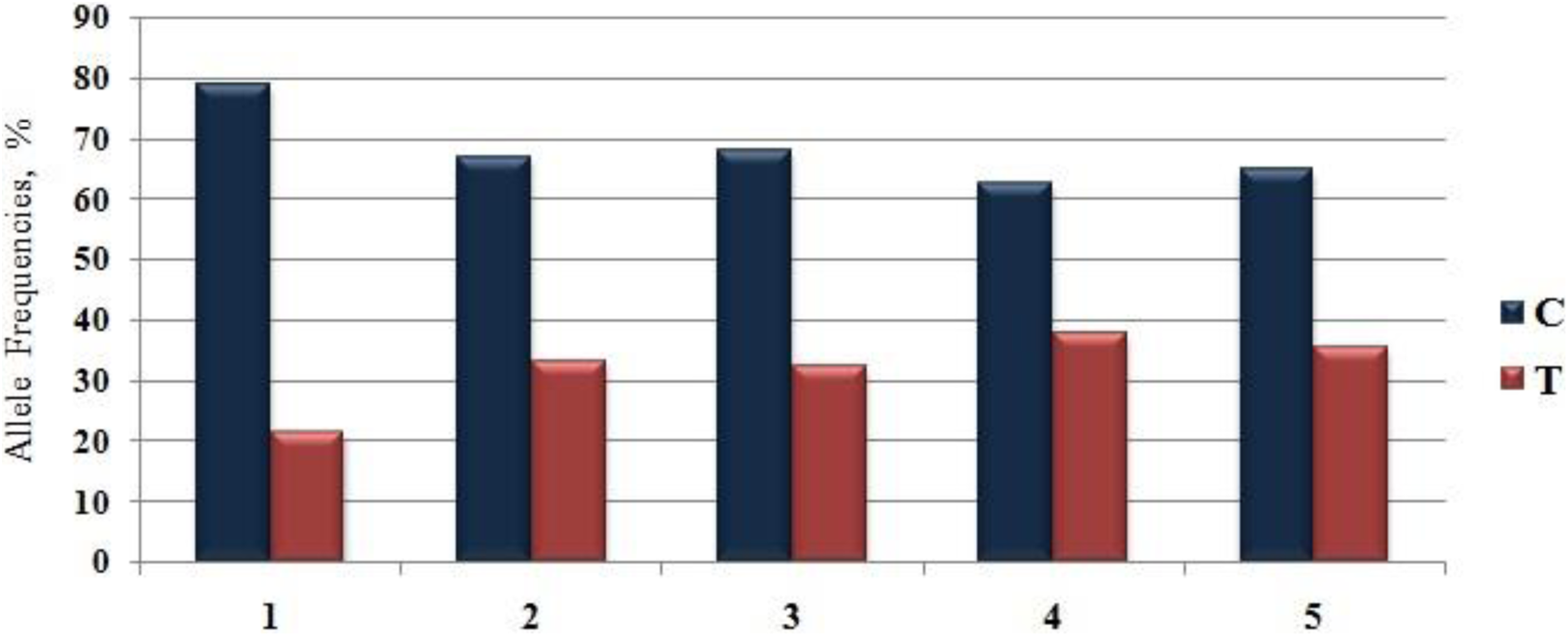
Allele (C, T) frequencies of C677T of MTHFR in the control and patients with arterial thrombosis groups: 1 (controls; n = 113), 2 (all patients; n = 101), 3 (myocardial infarction patients; n = 84), 4 (recurrent myocardial infarction patients; n = 12), and 5 (ischemic stroke patients; n = 17) groups.
Comparing the frequency of the mutated allele between the 2 groups (patients vs controls), a significantly high frequency of mutated alleles was found in the patient group (P < .05). When patients were stratified according to the MI and ischemic stroke status, a significantly high prevalence was also noticed in the MI patient group (P < .05) as compared to the control group (Table 1).
No significant differences were observed in the frequency of the MTHFR C677T polymorphism between the ischemic stroke group of patients and the control group or between the recurrent MI patients and the control groups (Table 1, Figures 2 and 3). However, the prevalence of the MTHFR C677T polymorphism was very similar in these 2 groups of patients, suggesting that these nonsignificant differences are likely to be related to the relatively smaller number of participants enrolled in these 2 group of patients (ischemic stroke and recurrent MI).
Discussion
Cardiovascular disease remains the main cause of all mortality in the world. Based on a recent analysis, there were >54 million deaths globally and 32% of these deaths (or 17 million) were attributable to cardiovascular disease. 10 Higher levels of plasmatic homocysteine were strongly associated with the incidence/development of coronary, cerebral, and peripheral arteries and veins diseases, indicating that homocysteine is one of the major independent risk factors that predicts and precedes the occurrence of cardiovascular disease. 11 In the current study, we demonstrated that the presence of the common polymorphism c.677C >T in the MTHFR gene, previously associated with high homocysteine levels, might increase the risk of arterial thrombosis in the Georgian population.
Although over the last few decades the C677T MTHFR polymorphism has been widely evaluated globally, the results of this study are the first data about its frequency in healthy and arterial thrombosis individuals from Georgia (the Adjara region). The frequency of the T allele in our control group was 21.1%, and the frequencies of heterozygosity and homozygosity for the C677T MTHFR polymorphism were 35.4% and 3.5%, respectively. In a report, 12 the Mexican population showed the highest frequency of the C677T MTHFR polymorphism (with a T allele frequency of 59% and a frequency of homozygosity of 35%). In the same study, 12 the authors also reported high prevalence of the T allele in Korea (40.3%) and in the northern (40.4%) and southern (44%) regions of Italy. In contrast, a relatively lower prevalence of the T allele was found in an Inuit population of Canada (6%), in Sub-Saharan Africa (6.3%), and in the southern part of Africa (10.3%). An Asian population also displayed remarkable heterogeneity, with very low values for Indonesians (4.1%) and high values for the Chinese (37.5%). 13 The frequency of the T allele in different populations ranged from 0.06 to 0.59, and the frequency of the TT genotype ranged from 0.00% to 35%. 13,14 Thus, the prevalence of the T allele found in our Georgian population (21.1%) is within the reported ranges globally, however is relatively lower than that found in most European countries and higher than those found in the Indonesian and African populations.
The frequency of the T allele in our group of arterial thrombosis patients is 21.1% and the frequencies of heterozygosity and homozygosity for the C677T MTHFR polymorphism are 48.5% and 3.5%, respectively, which are significantly higher than those found in the control group. We also observed significantly higher prevalence of this polymorphism in the MI patient group as compared to the control group. These data suggest that this polymorphism might be associated with an increased risk of arterial thrombosis.
Myocardial infarction is one of the most prevalent cardiovascular diseases worldwide 15 and it is a major contributor to cardiovascular mortality. 16 It is a complex, multifactorial, and polygenic disease that involves interaction between the genetic predisposition and environmental influences. 17 Traditional risk factors, including diet, diabetes, dyslipidemia, hypertension, obesity, inflammation, alcohol consumption, and smoking, predict around 50% of the absolute risk for a cardiovascular event, and the remaining risk can be attributed to genetic factors, including the presence of the C677T MTHFR polymorphism, as evidenced from our findings. Indeed, the C677T polymorphism in the MTHFR gene has been suggested as a potential genetic factor for the MI susceptibility.
The presence of the C677T MTHFR polymorphism reduces the thermostability of the MTHFR enzyme, which leads to an inability of the enzyme to catalyze the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate. Thus, homozygous mutated participants presented higher homocysteine levels, whereas the heterozygous mutated participants showed mild increase in the homocysteine levels compared to the normal and nonmutated controls. It should be noted that the common MTHFR variant has a risk factor for hyperhomocysteinemia, particularly when plasma folate status is low. Accordingly, mild hyperhomocysteinemia is a risk factor for cardiovascular disease, and additionally, in mutation carriers, folate should be an effective means of regulating plasma homocysteine level and therefore plays prominent role(s) in reducing the risk for development of cardiovascular disease. 18 Hyperhomocysteinemia has been reported as a risk factor for atherosclerosis and coronary artery diseases (CADs). 19 Indeed, 40% of patients with coronary, cerebral, or peripheral artery diseases showed high plasma homocysteine levels. 20 The exact mechanism of how an increased level of homocysteine leads to the development of vascular lesions remains unknown. Some researchers have postulated that homocysteine could cause atherogenesis and thrombogenesis, leading to substantial fibrosis and muscle cell hyperplasia. 20 In our study cohort, the plasma homocysteine levels were not tested, which would be the topic for our future study analyses.
In regard to the role of gene polymorphism in arterial thrombosis in other populations and the level of risks associated with it, several peer-reviewed studies have been reported. 21 –25 Huh et al 21 reported that individuals homozygous for the TT genotype had significantly elevated homocysteine levels (P < .05). It should be noted that the genotype-specific folate threshold level was significantly higher in TT individuals compared with CC or CT genotypes. It is noteworthy that the odds ratio (OR) of patients with low folate status and TT genotype have shown risk for CAD (2.2-fold), also the OR of individuals who had high folate status and TT genotype was 1.5-fold, and the CAD risk was 2.2 (95% confidence interval [CI], 0.5-9.6 and 0.7-3.2). 21 A study on the MTHFR C677T mutations showed strong association between the elevated homocysteine, the TT genotype, and PAD (OR: 2.82 [95% CI: 1.03-7.77], respectively) compared to homozygotes of the MTHFR 677 CC genotype. 22 More recently, Ramkaran et al 23 demonstrated that there was a significant association between patients with 677 MTHFR variant (T) allele and CAD compared to the healthy Indian participants (P = .0353, OR: 2.105, 95% CI: 1.077-4.114, respectively). Also, Bharatkumar et al 24 reported the association between plasma homocysteine, MTHFR C677T polymorphism, and cerebral veno-sinus thrombosis (CVT) in patients with aseptic CVT. This study demonstrated that fasting homocysteine was higher among the patients compared to controls (20.25 ± 5.97 mmol/L vs 9.81 ± 5.19 mmol/L, P < .001, respectively) and correlated with 4.54-fold (95% CI 2.74-7.53) increase risk of CVT. Notably, plasma homocysteine was higher in MTHFR 677TT as compared to 677CT and 677CC genotypes (34.44 ± 32.8 mmol/L vs 25.81 ± 33.3 mmol/L vs 18.50 ± 23.7 mmol/L; P < .001), but the risk associated with MTHFR 677TT was insignificant (OR: 1.91, 95% CI: 0.53-7.06). 24 Furthermore, Wang et al 25 studied the plasma total homocysteine level and MTHFR gene C677T polymorphism in predicting hyperhomocysteinemia in Chinese patients with hypertension and suggested that C677T polymorphism could be a useful screening marker for severe hyperhomocysteinemia. It should be noted that TT genotype had a large increase in the OR for hyperhomocysteinemia. Also, the multivariate-adjusted ORs of the TT genotype for mild, modest, and severe hyperhomocysteinemia were determined to be as 3.9 (95% CI 2.4-6.4), 6.5 (95% CI 4.0-10.6), and 17.9 (95% CI 8.4-38.1), respectively. Collectively, these studies implicate the role of gene polymorphism in arterial thrombosis in several other populations and the level of risks associated with the disease.
In conclusion, our study demonstrated a high prevalence of the MTHFR C677T polymorphism in a group of patients with arterial thrombosis, which suggests that this polymorphism might increase the risk of arterial thrombosis in the Georgian population. Additional studies with larger number of patients with arterial thrombosis from a more diverse (broader) region of the country would be desirable to further strengthen our observation on the prevalence of C677T MTHFR polymorphism.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received financial support from the European Union (FEDER funds POCI/01/0145/FEDER/007728) and National Funds (FCT/MEC, Fundação para a Ciência e Tecnologia and Ministério da Educação e Ciência, Portugal) under the Partnership Agreement PT2020 UID/MULTI/ 04378/2013.