
Abstract
This study aims to examine the effects of atrial fibrillation (AF) on the expression of the cellular mediators plasminogen activator inhibitor 1 (PAI-1) and CD40 ligand (CD40-L). Additionally, the effect of catheter ablation on the levels of the aforementioned biomarkers was also examined. In this prospective study, plasma samples were collected from patients with AF at baseline prior to ablation and at 1 and 3 months postablation. There was a statistically significant increase in CD40-L at baseline in patients with AF compared to control (P = .0034). There was a statistically significant decrease in CD40-L levels postablation at both 1 month (P < .0001) and 3 months (P < .0001) compared to baseline. Baseline levels of PAI-1 were elevated compared to the control group (mean 19.55 ± 2.17 ng/mL vs 4.85 ± 0.41 ng/mL) and a statistically significant decrease in circulating PAI-1 levels 1 month postablation (P = .05) was noted compared to preablation levels. These data suggest that inflammation plays an important role in the pathogenesis of AF and that these cellular mediators are modulated by catheter ablation.
Introduction
Atrial fibrillation (AF) is currently the most common cardiac arrhythmia encountered in clinical practice and is a major cause of both morbidity and mortality in the adult population. It is estimated to affect more than 2.7 million Americans in 2010, and the prevalence is expected to rise to 12.1 million by 2030. 1 Atrial fibrillation has an enormous impact on the lives and quality of life of patients as the complications from AF include stroke, sudden cardiac death, progressive heart failure, and noncardiovascular death. 1,2 The pathophysiological mechanisms that underlie AF include structural and electrical remodeling of the left atrium. 3 Inflammation has been implicated in the progression of AF and is associated with an increased risk of thromboembolic complications that increase morbidity and mortality. 4
One current treatment modality for patients with AF is catheter ablation, an invasive electrophysiologic approach generally preferred for refractory AF. 5,6 Electrical cardiac mapping is performed to locate the site of the aberrant electrical potentials, followed by radiofrequency or cryothermal ablation of that site. A meta-analysis found that 53% of patients undergoing a single procedure remained AF-free. 7
CD40 ligand (CD40-L), also known as CD154, is a membrane-bound protein associated with immune, endocrine, and inflammatory pathways. 8 CD40 ligand is considered a part of the tumor necrosis factor family. 8,9 CD40-L has been observed on the surface of many cell lineages including monocytes, macrophages, neutrophils, smooth muscle cells, endothelial cells, and platelets. 10 Recent research has shown that CD40-L expressed on the surface of platelets mediates inflammatory and thrombogenic pathways in the body. 11 In addition to CD40-L binding to its CD40 receptor, it is also capable of binding to inflammatory receptors for von Willebrand factor, fibrinogen, and various integrins. 11 Studies have shown increased levels of circulating thrombogenic biomarkers in patients with AF. The role of CD40-L in these various pathways prompted our investigation of its levels in patients with AF, a disease of both inflammation and thrombogenic dysregulation, both of which have significant clinical implications for patients with this arrhythmia.
Another important regulator of thrombogenesis in patients with AF is plasminogen activator inhibitor (PAI), an inhibitory molecule that downregulates the fibrinolytic pathway. 12 Plasminogen, a protease enzyme, plays a crucial role in fibrin clot dissolution when converted to its active form, plasmin, and lyses the fibrin meshwork of clots. 13 The most active form of PAI is PAI-1. Plasminogen activator inhibitor 1 can irreversibly bind to tissue-type plasminogen activator (t-PA), inhibiting the conversion of plasminogen to plasmin. 14,15 This irreversible binding inactivates t-PA, thus inducing a fibrinolytic deficit, and has been shown to increase the risk of stroke in patients with AF. 16 In addition to its role in thrombus formation, PAI-1 also plays an active role in tissue fibrosis with prolonged inflammation. 4,15 The role of PAI-1 role is not limited to downregulating fibrin degradation but also extends to downregulating collagen turnover leading to scar formation. 15 As previously mentioned, the risk of stroke, thrombotic complications, and myocardial scarring in patients with AF is elevated and examining the role of PAI-1 may help characterize such risks and outcomes.
Patients, Materials, and Methods
Patients
Patients with nonvalvular AF undergoing ablation at Loyola University Medical Center, Maywood, Illinois (n = 53, age: 18-81 years, mean age: 60.5 years) were consented and enrolled in this study prior to ablation procedure. Demographic and disease characteristic data are included in Table 1. The demographic and medical histories for 3 patients included in the study were not retrievable, which is reflected on Table 1. Baseline blood samples were obtained prior to ablation. Postablation samples were collected at 1- and 3-month follow-up visits. At each collection, whole blood was drawn and placed into tubes containing 3.2% (0.109 M) sodium citrate. Samples were centrifuged at 3000g for 15 minutes and supernatant platelet-poor plasma was harvested and aliquots were stored at −70°C until analysis. The samples were de-identified and stored frozen until analysis. This study was approved by the institutional review board of Loyola University Medical Center.
Demographic and Clinical Characteristics of Patient Cohort at Enrollment.
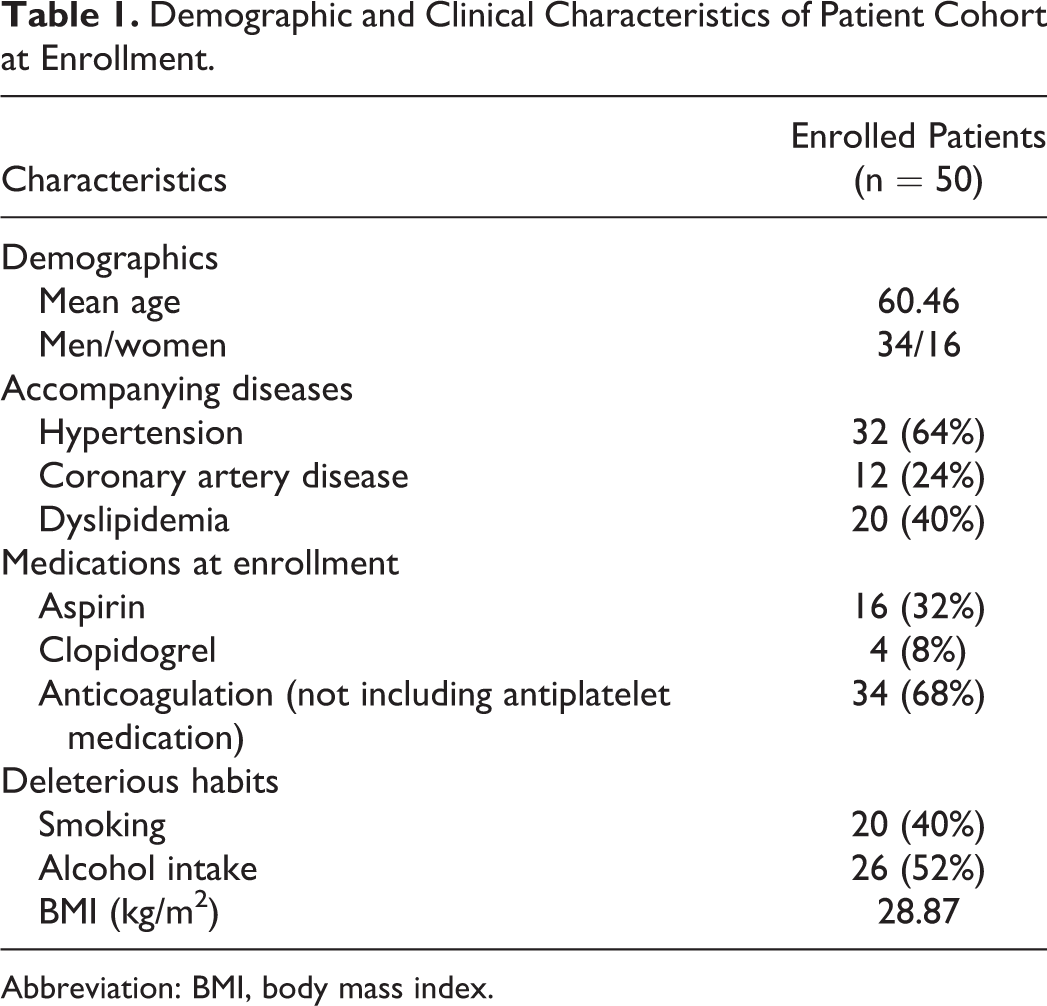
Abbreviation: BMI, body mass index.
Eligibility criteria
Patients ages 18 or above, who received care for AF as either inpatients or outpatients at Loyola University Medical Center, were included in this study. Exclusion criteria for this study were critically ill patients suffering from acute stroke, acute myocardial infarction, severe heart failure, or sepsis or those being mechanically ventilated. Because of the effect pregnancy can have on biomarker levels, pregnant females or nursing mothers were not included in this study.
Controls
Citrate plasma samples from healthy humans (n = 50, ages: 19-54 years, mean: 33 years) were purchased from George King Biomedical Inc (Overland Park, Kansas).
Material and Methods
Enzyme-Linked Immunosorbent Assay (ELISA) kits were obtained from R&D Systems (Minneapolis, MN) to profile CD40-L (Minnesota). This kit uses the quantitative sandwich enzyme immunoassay technique to quantify levels of CD40-L within our plasma samples. The kit provides antibody-coated plates along with standards for calibration purposes. ELISA kits for the assessment of PAI-1 were obtained from Aniara (Neuville-Sur-Oise, France). This PAI-1 kit employs the quantitative sandwich enzyme immunoassay technique for the measurement of PAI-1 levels within our plasma samples. Standards and controls are provided for calibration purposes. Statistical analysis was performed using GraphPad Prism (version 7) and Microsoft Excel. Nonpaired and nonparametric Mann-Whitney U tests were used when comparing the 2 groups. Correlation analysis was performed with nonparametric Spearman tests. In all analysis, data were considered statistically significant if P values were less than .05.
Patient plasma samples used in this investigation were studied in prior research endeavors. For our study, we randomly selected a subset of these matched sets of samples based on availability and continuity of samples from baseline to 1 month to 3 months postablation.
Results
Comparison of CD40-L Levels in AF at Baseline, 1 Month, and 3 Months Postablation
As seen in Figure 1, CD40-L levels were statistically elevated in the baseline AF samples compared to the control group (P < .0001). The level of CD40-L was significantly lower in the 1-month and 3-month postablation samples compared to baseline (P < .0001, P < .001, respectively). There was no significant difference in levels of CD40-L at 1 month compared to 3 months postablation (P = .8573) and no changes when comparing the 1- and 3-month groups to the control group (P = .2095 and P = .2926, respectively). Mean values for these time points are outlined in Table 2.
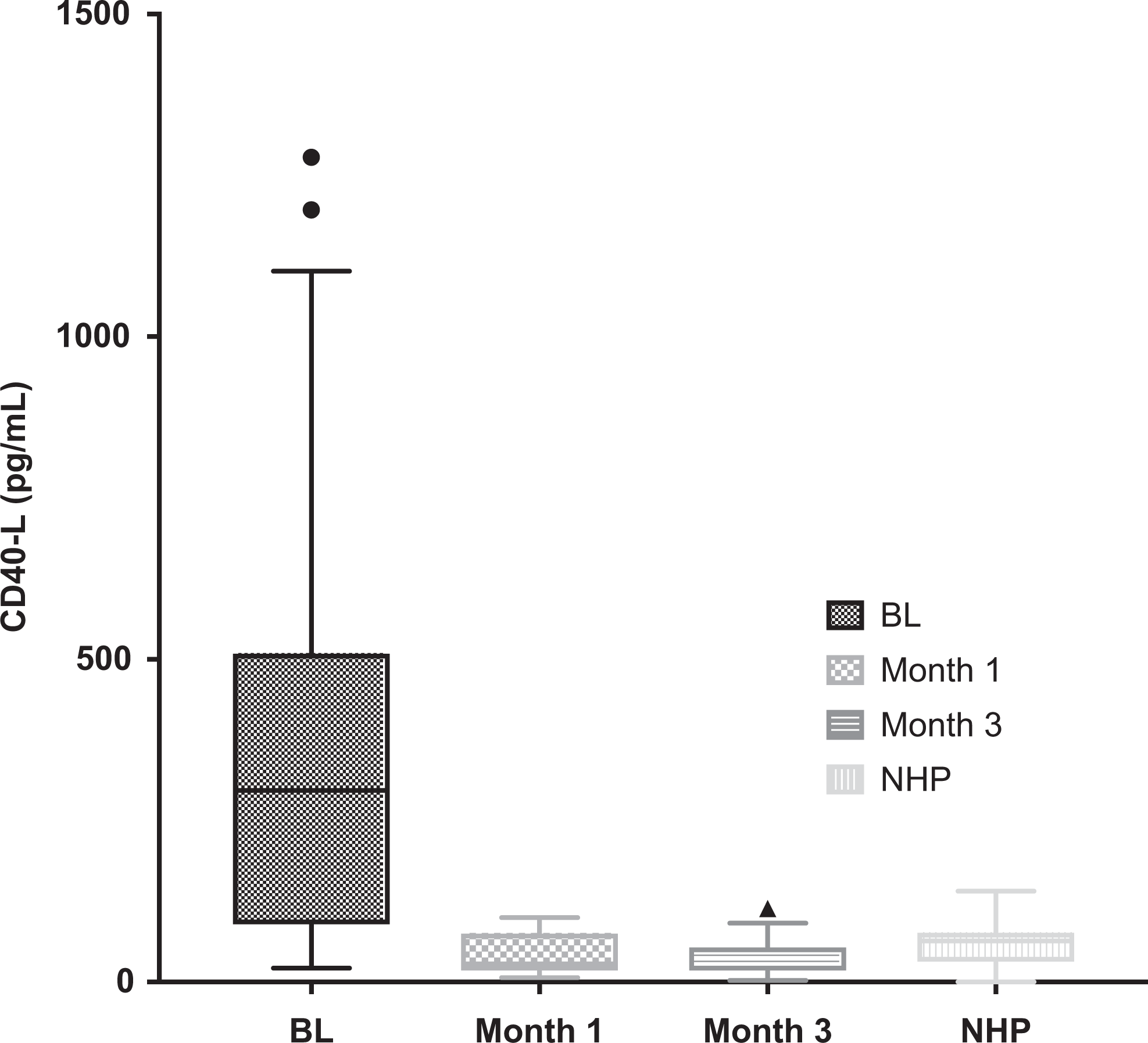
Box plots of CD40 ligand (CD40-L) levels in the control group versus atrial fibrillation (AF) group at baseline (BL) and month 1 and month 3 postablation. Boxes show interquartile ranges, and I bars represent highest and lowest values.
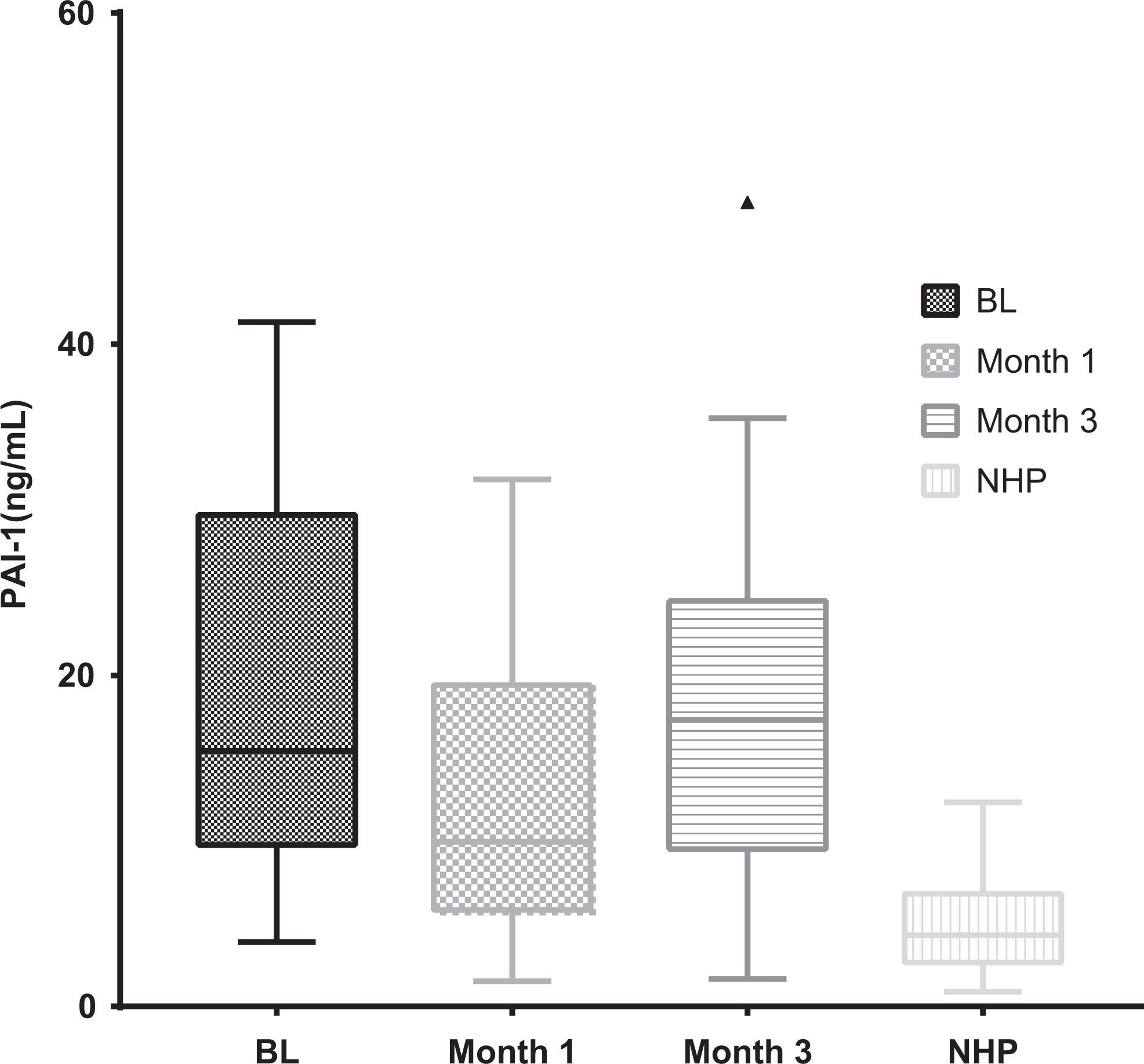
Box plots of plasminogen activator inhibitor 1 (PAI-1) levels in the control group versus atrial fibrillation (AF) group at baseline (BL) and month 1 and month 3 postablation.
Control Versus Baseline, Month 1, and Month 3 Levels of CD40-L and PAI-1 Biomarkers in Circulation.a

Abbreviations: CD40-L, CD40 ligand; PAI-1, plasminogen activator inhibitor 1.
aValues presented as mean ± standard error (SE); values of P < .05 were regarded as significant; Mann Whitney U test.
Comparison of PAI-1 Levels in AF at Baseline and Month 1 and 3 Postablation
Compared to the pooled control sample, there is an increased level of circulating PAI-1 (mean at baseline = 19.55 ± 2.17 ng/mL vs normal control = 4.85 ± 0.41 ng/mL).This is illustrated in Table 2. We used the normal control samples in order to compare the baseline levels of patients with AF to similar healthy humans without heart conditions. The normal control sample group was obtained using the normal human plasma from George King Biomedical. The baseline AF patient population had a significantly elevated PAI-1 level when compared to the normal control sample (P < .0001). Compared to baseline, there is a statistically significant decrease in levels of PAI-1 at 1 month postablation (P = .0425). There was a decrease in the level of PAI-1 at baseline compared to the level at 3 months postablation; however, this decrease was not statistically significant (P = .7393). There was no significant difference in levels of PAI-1 in the 1-month post ablation group compared to the 3-month postablation group (P = .1067). Mean values for these time points are outlined in Table 2.
Correlation of CD40-L and PAI Levels in Patients With AF
When comparing the baseline values of CD40-L to the baseline values of PAI-1 in the AF patient group, there was no correlation noted (P = .1375). This lack of correlation is reflected in Figure 3.
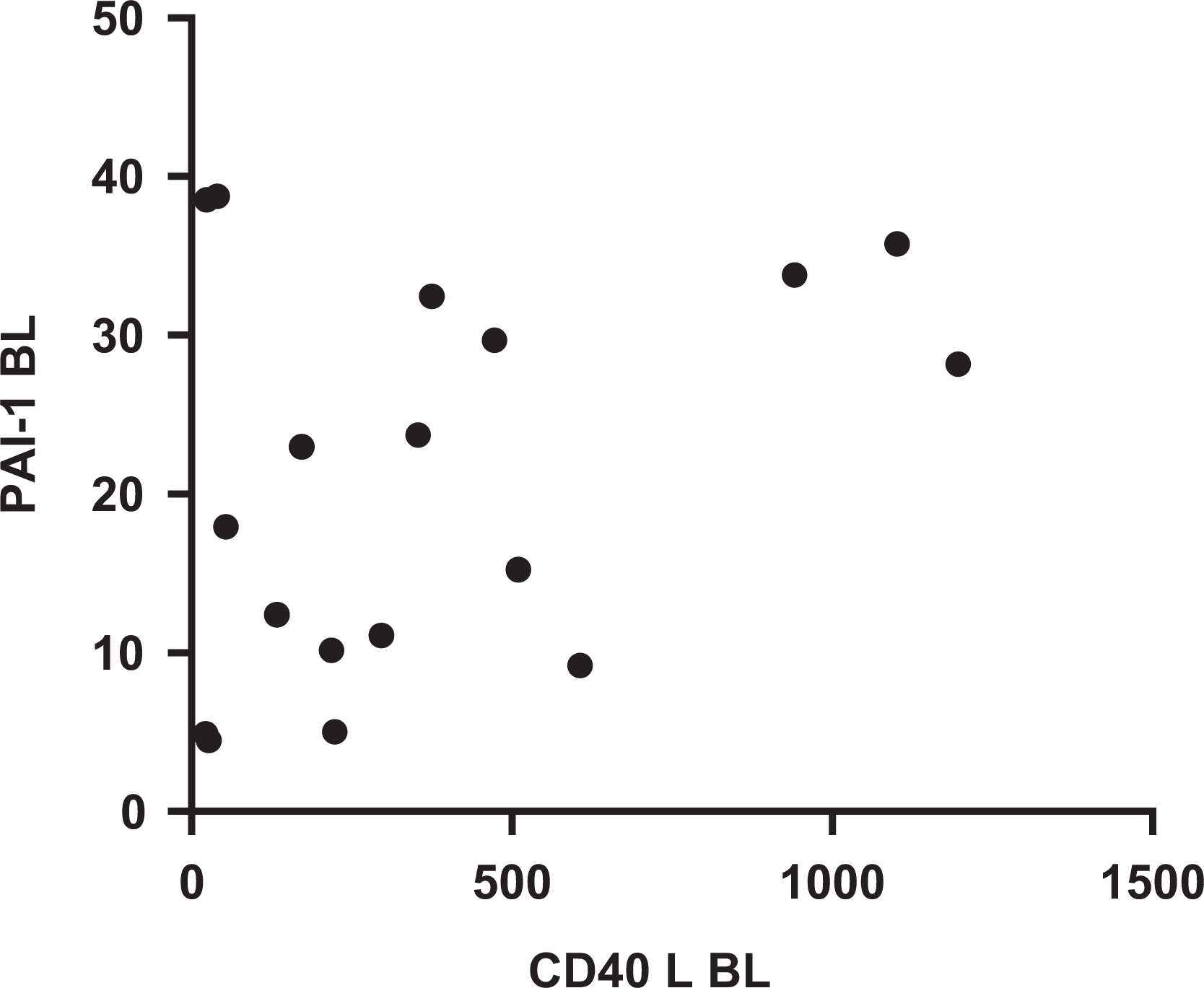
XY scatterplot of CD40 ligand (CD40-L) versus plasminogen activator inhibitor 1 (PAI-1) baseline values.
Baseline CD40-L Levels in Subtype of AF
The patients’ demographic and disease data including risk factor were collected from electronic medical records and charted against all biomarker information. When analyzing the relation between the level of CD40-L and the subtype of AF (persistent or paroxysmal), a significantly elevated mean level of CD40-L was noted in the paroxysmal AF group compared to the persistent AF group (P = .05).
Discussion
Atrial fibrillation is one of the most commonly diagnosed and treated heart arrhythmias in clinical practice today. 1 There are multiple known factors that contribute to the pathogenesis and propagation of AF and likely more that have yet to be discovered. 3,4 Previous reports have indicated that inflammation plays a crucial role in various cardiac diseases, including AF. 17 This elevated inflammatory state has been implicated in both the progression of AF and the increased risk of thrombotic events in these patients. 18
In our patient population, we found that treatment of AF by ablation resulted in normalization of the observed arrhythmic response. The purpose of our study was to examine the effects of catheter ablation for the treatment of AF on the levels of circulating inflammatory biomarkers.
The activation of platelets induces the generation of a soluble CD40-L which is shed in order to activate other inflammatory cell lines as well as more platelets. Previous studies have shown that patients with AF have higher levels of inflammatory and thrombotic events and this knowledge led us to investigate CD40-L’s level pre- and postablative treatment in an AF population.
In regard to the inflammatory state as it relates to the expression of CD40-L in patients with AF, our results may have several clinical implications. Our study demonstrates that in comparison to controls, CD40-L levels in patients with AF were significantly elevated. In addition, there was a marked decrease in the CD40-L levels after ablation. This decrease in CD40-L returned the levels of patients with AF back to levels comparable to the controls. As reported in the Results section, the control group has a substantially lower mean level compared to the baseline levels in the AF population. At both 1 month and 3 months postablation, levels were considerably reduced to levels comparable to the control group. Contrary to other previous reports, we found that within our patient population, levels of CD40-L decreased significantly after atrial ablation. At this time, the mechanism of postablation decreases in CD40-L is not fully understood; however, we hypothesize that this decrease may be related to a lowering of platelet numbers and a reduction in activation due to a downregulation of the inflammatory state.
Plasminogen activator inhibitor 1 downregulates fibrinolytic pathways in an inhibitory fashion. Plasminogen activator inhibitor 1 is commonly known to be a strong marker of inflammation and is primarily involved in fibrinolytic deficit often seen in AF. In our study, we found that when compared to control, those patients with AF had higher levels of PAI-1. This indicates that in patients with AF, there is more downregulation of fibrinolysis. When comparing the patients with AF pre- and postablation, we also found a decrease in PAI-1 levels. The decrease in the PAI-1 levels in comparison to baseline was noted at both 1 and 3 months postablation. This suggests that treatment with atrial ablation may correct the fibrinolytic deficit observed in patients with AF. However, due to the small sample size, our results require further statistical validation.
Although both CD40-L and PAI-1 are markers of inflammation, the correlation analysis used to compare the levels of these specific biomarker to one another did not show a positive correlation (Figure 3). This simply suggests that these 2 inflammatory biomarkers are regulated by different pathways but are nonetheless still activated simultaneously with the increased inflammatory and thrombogenic states observed in AF.
In future studies, we hope to continue to explore the significance of these inflammatory and thrombogenic biomarkers in our AF population with larger patient cohorts. Our data demonstrate a dramatic reduction in various biomarkers, but due to the limited number of patients, these studies require further validation in the setting of larger studies. We anticipate that with larger sample sizes, we may find more statistically significant data to confirm these observations.
There may be a diagnostic significance in observing the levels of CD40-L in patients with AF as a technique for risk stratification and as a means to track disease progression. We plan to correlate clinical data with our current results to explore how various treatment options and pharmacologic interventions might improve outcomes for this patient population. Previous studies by Liles et al have examined the use and effects of antithrombotic drugs in patient with AF and shown the drugs’ effects in downregulating the levels of various thrombotic biomarkers. 18 These results, when compared and combined with the current data from this study, may yield important information that will have clinical implications in both the diagnosis and treatment of AF.
Footnotes
Authors’ Note
This study was carried out under a T35 grant from the National Heart Lung and Blood Institute of the National Institutes of Health to foster student research at Loyola University Medical Center.
Acknowledgments
The authors gratefully acknowledge the skillful assistance of the nursing staff of the Department of Cardiology at Loyola University Hospital in facilitating this study. The authors are thankful to Dr Wojcik, the chairperson of the Department of Pathology, for her support. The authors are also grateful to Dr Gail Hecht for providing the research opportunity to the primary author of this study through the Student Training in Approaches to Research (STAR) summer program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.